Article Text

Abstract
AIM To determine if pulmonary haemorrhage after surfactant treatment increases short and long term morbidity and mortality in neonates weighing <1500 g at birth.
METHODS Neonates weighing <1500 g at birth who developed pulmonary haemorrhage after surfactant treatment were identified from a database. Based on the change in FIO2, pulmonary haemorrhage was classified as mild, moderate, or severe. Controls were matched for birthweight, gestational age, Apgar scores and hospital. Chronic lung disease (CLD) was defined as the need for supplemental oxygen at 36 weeks of corrected gestational age.
RESULTS From January 1990 to May 1994, 94 of 787 (11.9%) neonates treated with surfactant developed pulmonary haemorrhage. Ten were excluded because of incomplete data or lack of controls. Eighty four were included for further analysis; two acceptable matches were found in 75, while only one match was possible in nine. For the pulmonary haemorrhage group, the mean (SD) birthweight was 917 (238) g, gestational age 27 (1.9) weeks. Pulmonary haemorrhage was severe in 39 (46%), moderate in 22 (26%), and mild in 23 (27%). Moderate and severe pulmonary haemorrhage were associated with chronic lung disease or death, OR 4.4 (confidence interval 1.3–15.7) and OR 7.8 (CI 2.6–28), respectively, while mild pulmonary haemorrhage was not, OR 1.8 (CI 0.55–5.8). pulmonary haemorrhage was associated with major intraventricular haemorrhage (IVH), OR 3.1 (CI 1.5–6.4), but not with minor IVH, OR 1.3 (CI 0.6–2.6). In the survivors who could be assessed at ⩾2 years, the differences in neurodevelopmental outcome among the two groups were not significant.
CONCLUSIONS In neonates treated with surfactant moderate and severe pulmonary haemorrhage is associated with an increased risk of death and short term morbidity. Pulmonary haemorrhage does not seem to be associated with increased long term morbidity.
- prematurity
- respiratory distress syndrome
- pulmonary haemorrhage
Statistics from Altmetric.com
Exogenous surfactant is now an established treatment for respiratory distress syndrome (RDS). It seems to be safe and effective for the management of RDS and significantly reduces morbidity and mortality. 1 The risk of pulmonary haemorrhage, however, seems to be increased in premature neonates with RDS who are treated with surfactant.2 There is little reported information on the clinical outcomes of neonates treated with surfactant who subsequently develop pulmonary haemorrhage. We therefore conducted a retrospective case–controlled study comparing outcomes of patients with RDS who developed pulmonary haemorrhage after surfactant treatment with those who did not. We aimed to determine if pulmonary haemorrhage following bovine surfactant (bLES) treatment increases mortality and short and long term morbidity in neonates weighing <1500 g at birth.
Methods
All neonates weighing <1500 g at birth who developed pulmonary haemorrhage after being treated with surfactant were identified from the surfactant database of three regional neonatal intensive care units in Toronto: Women’s College and Mount Sinai Hospitals (perinatal centres), and the Hospital for Sick Children (outborn unit). Pulmonary haemorrhage was defined as blood suctioned from the endotracheal tube. The surfactant database contains information on all patients who had been treated with surfactant at the three intensive care units and who were part of the open IND trial using bovine lipid extract surfactant (bLES, bLES Biochemicals Inc., London, Ontario, Canada). Surfactant was prepared according to the methods described in a published trial,3 and administered at a dose of 100 mg/kg. It was used only as rescue treatment in RDS.
For the purpose of the database, pulmonary haemorrhage was classified as mild if the FIO2 increased by <0.1, moderate if it increased by 0.1–0.3, and severe if the increase was >0.3 from the baseline. Controls were identified from the same database, and matched for birthweight (±50 g), gestational age (±1 week), 5 minute Apgar scores (±1), and hospital. Patients and controls were also matched such that their dates of birth were within the same 6 month period. We attempted to find two matched controls for each patient with pulmonary haemorrhage. However, if only one matched control was found, this was also acceptable. If no matched control was found, the patient was excluded from the study. Infants were excluded if they had Apgar scores ⩽3 at 5 minutes, or if they had serious congenital malformations.
OUTCOMES
The primary outcome measures were death and chronic lung disease (CLD). Secondary outcome measures were corrected gestational age at extubation, corrected gestational age when supplemental oxygen was not required, the incidence of IVH, periventricular leucomalacia (PVL), and retinopathy of prematurity (ROP), and neurodevelopmental outcome.
Death was coded if it occurred before discharge from the neonatal unit. CLD was defined as the requirement for supplemental oxygen at 36 weeks of corrected gestational age, with compatible clinical and radiological findings.4 5 IVH, diagnosed by ultrasound scan or at necropsy, was graded according to Papile,6 and the highest grade recorded. Minor IVH was defined as grades 1 and 2, while major IVH was defined as grades 3 and 4. PVL was defined as the observation of cystic periventricular changes on cranial ultrasound scan. ROP was classified according to an international classification,7and for the purposes of this study, ROP stages ⩾3 were considered to be significant. Data for ROP were analysed for those neonates who survived until discharge from hospital. Necrotising enterocolitis (NEC) was defined according to modified Bell’s criteria and stages 2 and 3 were considered clinically significant.8
Neurodevelopmental assessment data were obtained from neonatal follow up clinic records by clinicians who were unaware of the group assignments of the patients. Major neurodevelopmental handicap was defined as clinically significant sensory loss (blindness or deafness), cerebral palsy causing an inability to walk at the age of 2 years, or a Bayley score of <70. Minor neurodevelopmental handicap was defined as sensorimotor abnormality not leading to clinically significant functional limitation (vision corrected by glasses or abnormal hearing tests not requiring hearing aids), cerebral palsy not leading to an inability to walk by the age of 2 years, or a Bayley score of 70–84.
Associations were analysed using odds ratios and 95% confidence intervals. Differences were analysed by Fisher’s Exact Test and χ2 analysis. p Values <0.05 were considered to be significant.
Results
Between January 1990 and May 1994, 1532 neonates were treated with bLES, and 113 (7.4%) developed pulmonary haemorrhage. Of the 787 neonates (535 inborn, 252 outborn) who weighed <1500 g at birth, 94 (11.9%) developed pulmonary haemorrhage and fulfilled inclusion criteria. Ten were excluded from subsequent analysis: three because of incomplete data and seven because a matched control could not be identified. Of the 84 who were included for further analysis, two acceptable matched controls were found in 75, while only one match was possible in nine.
For the pulmonary haemorrhage group, the mean (SD) birthweight was 917 (238) g, and gestational age was 27 (1.9) weeks. There were no differences in birthweight, gestational age, sex, maternal steroid treatment or mode of delivery (caesarean section or vaginal) between the pulmonary haemorrhage and control groups (table 1). The distribution of severity of pulmonary haemorrhage according to birthweight, with the denominator being all neonates <1500 g treated with surfactant, is shown in fig 1. The occurrence of severe pulmonary haemorrhage decreased with increasing birthweight. For those with severe pulmonary haemorrhage, the birthweights of all except one were <1250 g. Severe pulmonary haemorrhage occurred in 39 (46%), moderate in 22 (26%), and mild in 23 (27%). For those in the pulmonary haemorrhage group who survived, the mean (SD) birthweights and gestational ages were 1009 (212) g and 27.5 (1.8) weeks, respectively. For the surviving controls, these were 974 (228) g and 27.1 (1.8) weeks, respectively. These differences were not significant. For those with pulmonary haemorrhage who died, the mean birthweights and gestational ages were 770 (199) g and 25.7 (1.4) weeks. For the controls who died, these were 754 (130) g and 25.2 (1.2) weeks, respectively (p = NS). However, for those with pulmonary haemorrhage the birthweights and gestational ages of those who died were significantly lower than those who survived; p <0.005. For the controls, the birthweights and gestational ages of those who died were also significantly lower than those of the survivors; p <0.005. There were no differences in the incidence of patent ductus arteriosus, the use of indomethacin, or the incidence of NEC (table 2). Those with pulmonary haemorrhage were more likely to have had a pneumothorax (p = 0.003).
Patient characteristics
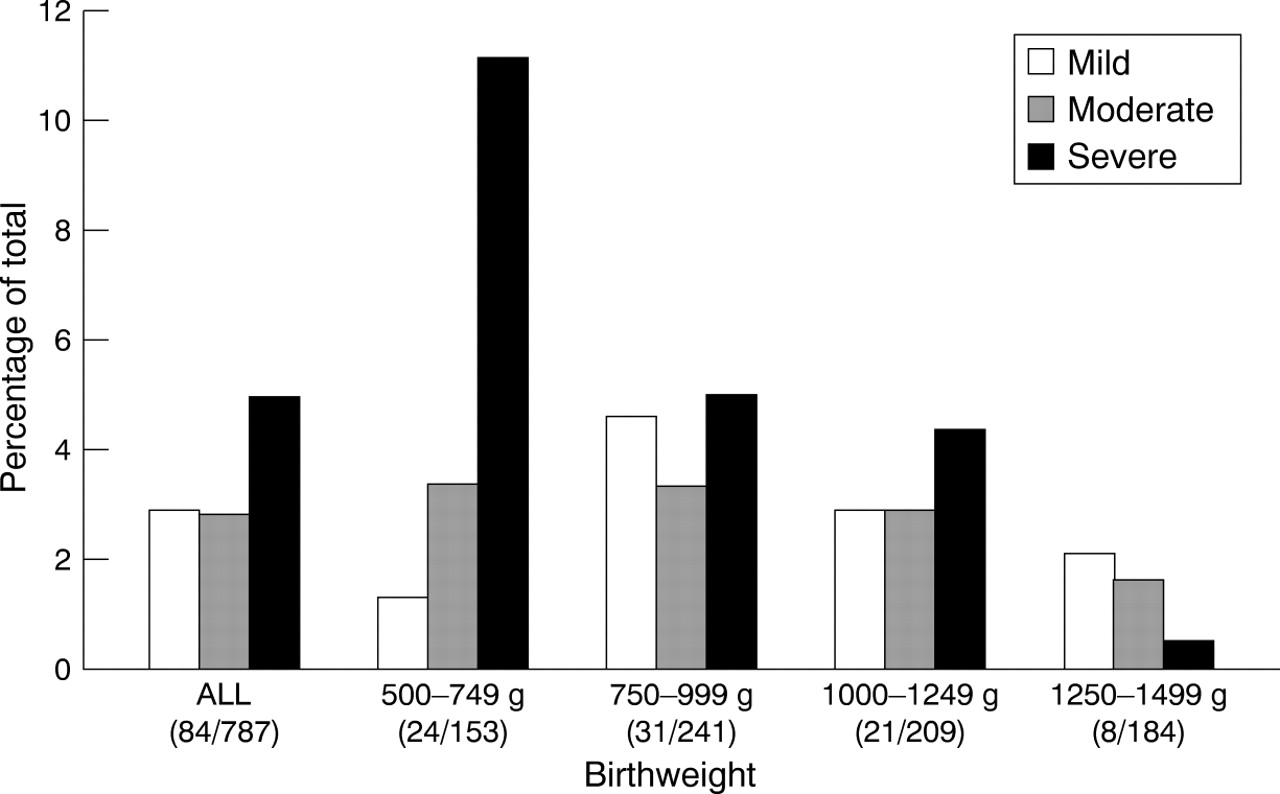
Distribution of mild, moderate, and severe pulmonary haemorrhage in various birthweight groups.
Neonatal complications
OUTCOMES
Table 3 shows the percentages of neonates with pulmonary haemorrhage and their controls who had the primary outcomes of death or CLD; fig 2 illustrates the association of the severity of pulmonary haemorrhage with CLD, death, and “death or CLD.” Of those with moderate pulmonary haemorrhage, 63% developed CLD, compared with 22% of the controls, OR 6.2 (CI 1.6–25). Of those with severe pulmonary haemorrhage, 64% died, compared with 20% of the controls, OR 6.9 (CI 2.7–18), while nine of the 14 survivors (64%) developed CLD, OR 3.7 (CI 0.94–15.8). Of the 32 who died in the pulmonary haemorrhage group, 25 had severe pulmonary haemorrhage. Those with pulmonary haemorrhage died earlier, at a median age of 3 days (range 1–42), compared with controls who died at 4 days (range 1–128); p = 0.02. Moderate and severe pulmonary haemorrhage were associated with “CLD or death,” OR 4.4 (CI 1.3–15.7) and OR 7.8 (CI 2.6–28), respectively. Mild pulmonary haemorrhage was not associated with “death or CLD,” OR 1.8 (CI 0.55–5.8).
Severity of PH and outcomes of CLD and death

{kind=link}
{kind=link}
Association between pulmonary haemorrhage of different severities and CLD, death or “death or CLD.”
For those who survived until discharge, the mean (SD) corrected gestational age at extubation was similar: 33 (3) weeks for the pulmonary haemorrhage group, and 32 (4) weeks for the controls. Neonates with pulmonary haemorrhage received supplemental oxygen for longer, until a mean (SD) corrected gestational age (in weeks) of 36 (4) weeks, compared with 34 (4) weeks in the controls; p <0.05.
For the pulmonary haemorrhage group, data for IVH were available for all survivors, and for 27 of 32 who died (table 2). For the controls, data for IVH were available for 154 of 159 neonates. Pulmonary haemorrhage was associated with major IVH (OR 3.1, CI 1.5–6.4), but not with minor IVH (OR 1.3, CI 0.6–2.6). For those who survived until discharge, there was no difference in the incidence of PVL in the two groups. ROP data were available for 47 of the 52 survivors in the pulmonary haemorrhage group, and for 122 of 137 controls. The distribution of severity of ROP is shown in table 2. No patient developed stage 4 ROP. The incidence of ROP in the two groups was similar.
Data for neurodevelopmental assessment are shown in table 4. Of those who survived until discharge from the neonatal unit—52 in the pulmonary haemorrhage group and 137 controls— follow up clinic data were available for 41 and 122, respectively. Data for neurodevelopmental assessment at ⩾2 years corrected gestational age were available for 39 (75%) in the pulmonary haemorrhage group and 103 (75%) controls. Although 28% in the pulmonary haemorrhage group developed major neurodevelopmental handicap compared with 17% of the controls, this difference was not significant.
Neurodevelopmental outcome
Discussion
Before surfactant had been introduced into clinical practice, pulmonary haemorrhage was associated with low birthweight, small for gestational age neonates, asphyxia, infection, and the presence of hyaline membrane disease at necropsy.9-12 The occurrence of pulmonary haemorrhage was often fatal, with mortality rates of up to 92%.10 With the advent of exogenous surfactant, the risk of pulmonary haemorrhage in neonates with RDS seems to have increased.2 Clinical associations with pulmonary haemorrhage in neonates treated with surfactant may include vaginal birth, low birthweight, younger gestational age, male sex, and the presence of a patent ductus arteriosus.13 14
The incidence of pulmonary haemorrhage reported in some of the larger surfactant trials varies from 1 to 11%.15-17 This reported incidence, however, may not be accurate as there is no generally accepted method of grading its severity. Some investigators could have classified as pulmonary haemorrhage even small amounts of blood from the endotracheal tube that could have been due to trauma following suction. Others may have reported only massive pulmonary haemorrhage. This may lead to either over- or under reporting, so that the true incidence of severe pulmonary haemorrhage remains hidden.2 Some investigators have used a combination of clinical and radiological criteria to report pulmonary haemorrhage. Our surfactant database does not include data on all patients who may have shown chest x-ray changes following pulmonary haemorrhage. The incidence of pulmonary haemorrhage (11.9%) in our cohort of <1500 g birthweight babies may seem high. It should be noted, however, that this includes all severities of pulmonary haemorrhage, including those neonates who did not sustain a clinically significant deterioration. Furthermore, all the patients in this study had RDS, and received surfactant only as rescue treatment. The overall incidence of pulmonary haemorrhage in all neonates treated with surfactant at the three neonatal intensive care units was 6.5%. This is comparable with that reported by other investigators.2
Those neonates with RDS who develop pulmonary haemorrhage might be sicker. We did not control specifically for severity of illness. This group also had a higher incidence of pneumothorax and of major IVH. Although these may reflect differences in severity of illness, the two groups were well matched for the major surrogates of severity of illness—namely, gestational age, birthweight, Apgar scores, and the diagnosis of RDS.
Management of pulmonary haemorrhage in the three hospitals included attempts to improve oxygenation and ventilation by increasing the FIO2, increasing positive end expiratory pressure, and changing other ventilatory parameters. Fluid resuscitation with blood or albumin was performed if indicated. After pulmonary haemorrhage, additional doses of surfactant were given to eight patients.18 Our results indicate that over 60% of neonates who have a severe pulmonary haemorrhage die, usually within the first 72 hours of life. Furthermore, 60% of those who survive a severe or moderate pulmonary haemorrhage develop CLD. Death after clinically significant pulmonary haemorrhage may occur despite attempts at resuscitation, as a result of severe cardiorespiratory deterioration. Those who survive this are likely to require an increased amount of oxygen as well as a greater degree of ventilatory support. This may lead to further lung injury and a greater risk for CLD.
In our cohort, those with pulmonary haemorrhage were three times more likely to develop major IVH. This association between IVH and pulmonary haemorrhage has been reported before.19 Although there is no clear explanation for this association, it is possible that in a neonate with a pressure passive cerebral circulation, IVH may be the result of the haemodynamic instability and hypotension that occurs following a clinically significant pulmonary haemorrhage. Another explanation could be that major IVH occurs first, causing the consumption of clotting factors and leading to pulmonary haemorrhage. In the survivors the incidence of PVL in the two groups was similar. Although 28% in the pulmonary haemorrhage group developed major handicap, compared with 17% of the controls, neurodevelopmental outcome at ⩾2 years was not significantly different between the two groups. This may have been due to the small sample size.
Our sample consists of patients who were treated with surfactant and weighed <1500 g. Although we have attempted to compare the outcomes in this study, there are few published data on comparable groups of patients. In their trial of human surfactant in <30 week gestation neonates, Vaucher et al 20reported that 33% had CLD, 17% grades 3 or 4 IVH, and 12% grades 3 or 4 ROP. At the age of 12 months, 25% had mild and 32% moderate to severe mental or motor delay. Of the controls in our study, 32% had CLD, 15% major IVH, and 13% significant ROP. At ⩾2 years, 18% had minor and 17% major neurodevelopmental handicap. The incidences of these markers of morbidity are similar in both studies. As noted in the results, the incidence of CLD, major IVH, and major neurodevelopmental handicap was higher in the pulmonary haemorrhage group.
In conclusion, in very low birthweight neonates with RDS and treated with surfactant, moderate and severe pulmonary haemorrhage, but not mild pulmonary haemorrhage, is associated with an increased risk of short term morbidity and mortality. Of those who develop moderate or severe pulmonary haemorrhage, 46% are likely to die and 60% of the survivors are likely to develop CLD. Although there is a greater incidence of major neurodevelopmental handicap in those who survive pulmonary haemorrhage, this difference is not significant. It is unclear whether pulmonary haemorrhage itself causes a poor outcome, or whether it is a marker for poor outcome in very low birthweight neonates who are treated with surfactant. Further research in the pathogenesis of pulmonary haemorrhage may help identify interventions that could improve outcome.