Article Text

Abstract
Background The National Trauma Data Bank (NTDB) has served as a global benchmark for trauma care quality and outcomes. Herein, we compared patient characteristics, trauma management, and outcomes between Japanese emergency and critical care centers and US level 1 trauma centers using the Japanese Trauma Data Bank (JTDB) and NTDB.
Methods A retrospective cohort matching (1:1) study was performed. Patients treated in 2013 with an Injury Severity Score ≥9 were included. The primary outcome measure was in-hospital mortality. The secondary outcome measures included the hospital length of stay and the rate of use of radiological diagnostic modalities.
Results A total of 14 960 pairs with well-balanced characteristics were generated from 22 535 and 112 060 eligible patients in the JTDB and NTDB, respectively. Before matching, the in-hospital mortality was higher in the JTDB than in the NTDB (7.6% vs. 6.1%; OR, 1.28; 95% CI 1.21 to 1.35). However, after matching, the in-hospital mortality was lower in the JTDB cohort (4.2% vs. 5.8%; OR, 0.72; 95% CI 0.65 to 0.80). CT scans were used in >80% of JTDB patients, which was more than 1.5 times as often as the use in the NTDB cohort. In subgroup analyses, only patients who received a blood transfusion had a poorer survival outcome in the JTDB compared with the NTDB (OR, 1.32; 95% CI 1.07 to 1.64).
Discussion We observed marked differences in trauma care between Japan and the USA. Although the quality of the recent Japanese trauma care appears to be approaching that of the USA, it may be further improved, such as by the establishment of transfusion protocols.
Level of evidence Level IV.
- trauma/ critical care
- japan
- comparison
- united states
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The USA has long had an advanced trauma system. The American College of Surgeons Committee on Trauma (ACS-COT) was established in 1922 and created a verification system for trauma centers, which is thought to provide survival benefit in the USA. Level 1 is the highest designation for trauma care, with stringent facility criteria established by the ACS-COT. Level 1 trauma centers are required to have a quality improvement program to monitor, evaluate, and improve trauma care. Thus, the collection of data is absolutely imperative. The National Trauma Data Bank (NTDB) is the largest trauma-related data set in the USA and has been used as a national benchmark to improve trauma care in the USA and as a worldwide benchmark to improve trauma care in other countries.
Historically, the quality of trauma outcomes has been poor in Japan; however, Japan has made concerted efforts to improve outcomes, especially over the past decade. Encouragingly, several recent articles have reported that mortality has decreased in trauma patients in Japan.1 Initially, the Japanese government established the concept of emergency and critical care centers (ECCCs) nationwide in 1977, and the Japanese Association for the Surgery of Trauma (JAST) was established in 1986 for the improvement of care in critically injured patients.2 However, the preventable trauma death rate in Japan was estimated as 38.1% in a 2001 survey of 107 ECCCs.3 The preventable death rate is much lower in the USA. A recent study on preventable death rates of an academic level 1 trauma center in San Diego county showed a remarkable preventable death rate of 0.7%.4 To further improve the quality of trauma care, Japan has implemented initiatives based on the experiences of the USA. In 2002, the JAST produced standardized guidelines for hospital trauma care, known as the Japan Advanced Trauma Evaluation and Care guidelines, using the Advanced Trauma Life Support guidelines as a model. Additionally, the Japan Trauma Data Bank (JTDB) was established in 2003 using the NTDB as a model, and many studies have been published using the JTDB data. However, to date, the JTDB has not been used effectively for quality improvement. Issues in the Japanese trauma care system may still remain.
There are many differences in trauma care between Japan and the USA, such as the trauma system, education, and social background. One of the significant differences is the existence of the trauma center. In Japan, there are no clearly established criteria for the designation of a trauma center, and an emergency physician usually conducts the initial trauma management as there are few inhouse trauma surgeons in ECCCs. Additionally, there is a potential for the overuse of CT scans in trauma care in Japan. Japan has, by far, the highest number of CT scanners per capita in the world.5 Patients and physicians in Japan favor the use of CT scans in various medical fields. Although such differences may strongly affect trauma outcomes, few international comparisons of trauma care and outcomes using registry data have been conducted.
We hypothesized that Japanese trauma care outcomes still lag behind those of US trauma centers. In the present study, we compared the patient characteristics, trauma management, and mortality outcomes between Japanese ECCCs and US level 1 trauma centers using the two national trauma registries. The aim of this study was to evaluate the current status of Japanese trauma care, using the NTDB as a benchmark, in an effort to further improve Japanese trauma care.
Methods
We conducted a retrospective cohort study, comparing national trauma registry data between Japan and the USA (the JTDB and NTDB, respectively) to evaluate Japanese trauma quality.
Data source and patient selection
Both data sets are voluntary data repositories that exist for the improvement of the quality of trauma care. The JTDB, managed by the JAST, comprises data regarding trauma admissions from more than 200 participating hospitals. The NTDB, managed by the ACS, comprises data regarding trauma admissions at levels I to V trauma centers, assembled from more than 900 participating hospitals across the USA.6 Both the JTDB and NTDB are considered representative of the national status of trauma care in their respective countries.
The JAST and ACS are not responsible for any claims arising from work based on the original data, text, tables, or figures related to the JTDB and NTDB.
We selected patients aged ≥16 years and an Injury Severity Score (ISS) ≥9 who were admitted to the JTDB or level I NTDB trauma centers in 2013. We did not control the hospital level in the JTDB because Japan does not have official trauma centers authorized by the government or any societies. However, almost all of the JTDB participating hospitals are ECCCs certified by the Japanese government. Patients who were dead on arrival (DOA), had an Abbreviated Injury Scale (AIS) score of 6 (AIS6) for any body region or had missing outcome data were excluded. We also excluded patients with gunshot wounds (GSWs), as the number of such cases was small in Japan.
Data collection and study endpoints
Demographics and injury-specific factors were compared between the two data sets. Demographic variables included age, sex, systolic blood pressure (SBP), ISS, Glasgow Coma Scale (GCS) score, type of injury, mechanism of injury, intent of injury, and maximum AIS severity score of each body region. Three surgeons reviewed the JTDB and NTDB dictionaries to convert and match the variables (online supplementary file 1).
Supplemental material
The primary outcome measure was in-hospital mortality. The secondary outcome measures included hospital and intensive care unit (ICU) length of stay, disposition at discharge, the rates of radiographic use, and major surgical procedures, including craniotomy, thoracotomy, and laparotomy. CT scans and angiography could have been obtained for any body part.
Statistical analyses
Data are presented as counts and percentages. Differences between data sets were evaluated using χ2 and Mann-Whitney U tests, as appropriate. To minimize the confounding effect of large differences in the patient characteristics between the two countries, an exact matching strategy was used. Patients in the JTDB were matched to those in the NTDB at a 1:1 ratio, without replacement, and priority was given to an exact match. Patients were matched based on age, sex, SBP, GCS score, ISS, injury type, injury mechanism, injury intent, and AIS severity score for each body part (head, face, neck, thorax, abdomen, spine, extremity, and skin), as shown in table 1.
Patient and injury characteristics in the JTDB and NTDB
To evaluate specific aspects of Japanese trauma care, we performed subgroup analyses according to patient characteristics and type of injury, using the exactly matched subset of patients. An interaction analysis was performed between subgroups.
Values of p<0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS for Windows V.24.0.
Results
Patient selection and matching
Figure 1 depicts the patient selection flow chart, as well as the reasons and numbers of the excluded patients. During the study period, enrolled patients were treated in 159 hospitals in the JTDB and 749 hospitals in the NTDB. The JTDB had few patients with GSWs (<0.001%), and 3.6% of the patients had an AIS6 or were DOA. The NTDB had a higher rate of patients with GSWs (5.0%) and fewer patients had an AIS6 or were DOA (1.4%) than those in the JTDB. After exclusion, 22 535 patients in the JTDB and 112 060 patients in the NTDB were eligible for inclusion in the present study. Using 1:1 exact matching, 14 960 well-balanced pairs of patients were generated.
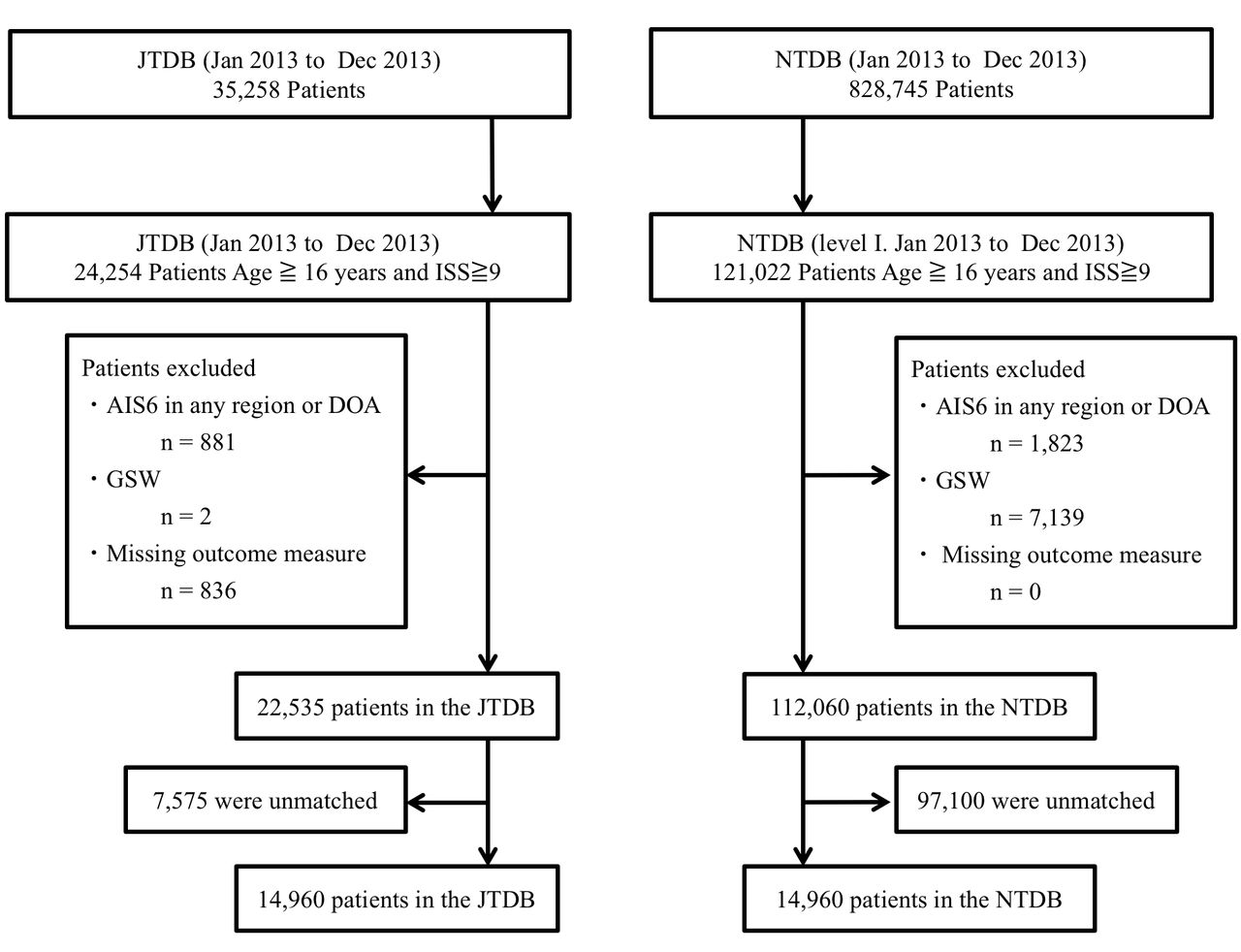
Flow chart of patient selection in the JTDB and NTDB. AIS6, Abbreviated Injury Scale score of 6; DOA, dead on arrival; GSW, gunshot wound; ISS, Injury Severity Score; JTDB, Japanese Trauma Data Bank; NTDB, National Trauma Data Bank.
Patient characteristics
The clinical characteristics of the patients in the JTDB and NTDB are summarized in table 1. As expected, there were significant differences between the two data sets. In particular, the JTDB had older age and a higher rate of self-inflicted injuries than those in the NTDB. On the other hand, the NTDB had higher rates of assault and deep unconsciousness, and a lower ISS, than those in the JTDB. After exact matching, the patient characteristics were well balanced across the JTDB and NTDB subsets.
Diagnostic image use and therapeutic interventions
Table 2 shows the rates of CT scan and angiography use and the therapeutic interventions in the unmatched and matched patients. The results before and after matching were mostly unchanged. CT scans were used in more than 80% of the patients in the JTDB, which was more than 1.5 times as often as that in the NTDB. However, angiography was more commonly used in the NTDB than in the JTDB.
Diagnostic images and therapeutic interventions in the JTDB and NTDB
Among the evaluated major surgical procedures, craniotomy was the most common surgery in the JTDB (3.3%), whereas laparotomy was the most common surgery in the NTDB (3.7%) before matching. After matching, craniotomy remained as more commonly performed in the JTDB than in the NTDB, but the rates of thoracotomy and laparotomy were similar in the two subsets.
Outcomes
Table 3 provides the in-hospital mortality and disposition at discharge in the JTDB and NTDB. Before matching, the in-hospital mortality was higher in the JTDB than in the NTDB (7.6% vs. 6.1%; OR, 1.28; 95% CI 1.21 to 1.35). The proportion of patients transferred to another medical institution was higher in the JTDB than in the NTDB (50.9% vs. 33.5%, p<0.001). However, after matching, the in-hospital mortality was lower in the JTDB than in the NTDB (4.2% vs. 5.8%; OR, 0.72; 95% CI 0.65 to 0.80), whereas the disposition at discharge was similar in the two subsets.
In-hospital mortality and length of stay in the JTDB and NTDB
Table 3 shows the hospital and ICU length of stay in the JTDB and NTDB. The results before and after matching were mostly unchanged. After matching, the median hospital length of stay in the JTDB subset was more than three times as long as that in the NTDB (17.0 (7.0–32.0) vs. 5.0 (3.0–8.0), p<0.001). However, the ICU length of stay was shorter in the JTDB than in the NTDB (2.0 (1.0–8.0) vs. 3.0 (2.0–6.0), p<0.001).
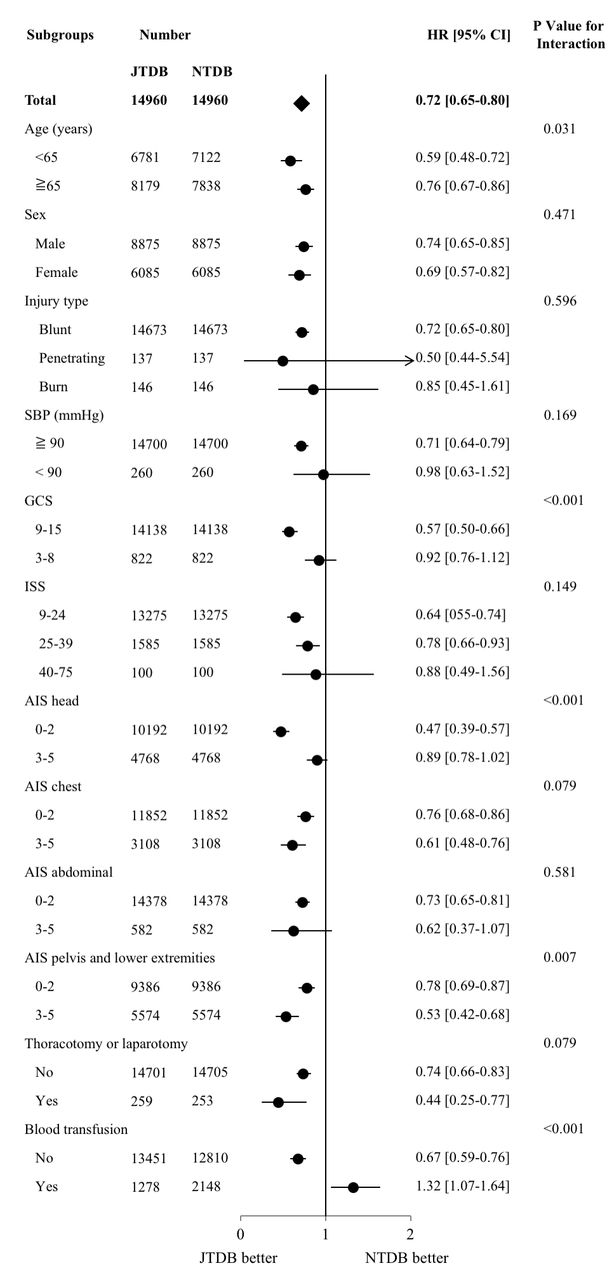
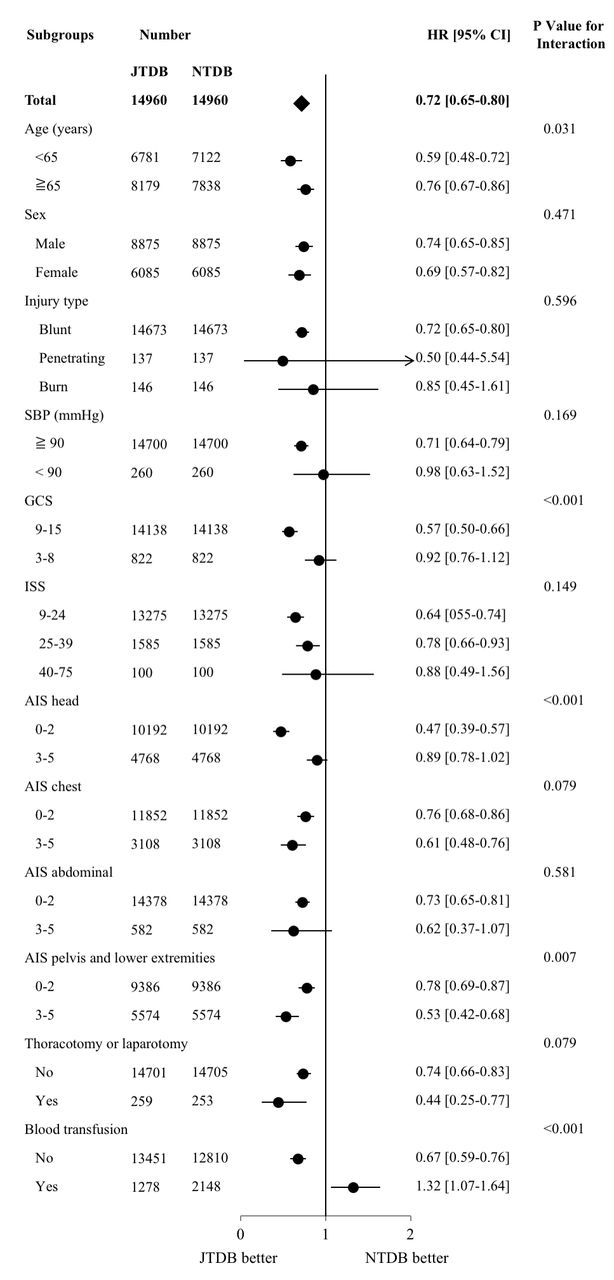
In the prespecified subgroup analyses, significant interactions were observed in the subgroups classified by age, GCS score, AIS score for the head, AIS score for the pelvis and lower extremities, and blood transfusion. Only patients who received a blood transfusion within 24 hours had a lower survival rate in the JTDB than in the NTDB (OR, 1.32; 95% CI 1.07 to 1.64) (figure 2).
{kind=link}
{kind=link}
Subgroup analyses according to various characteristics in matched patients. AIS, Abbreviated Injury Scale; GCS, Glasgow Coma Scale; ISS, Injury Severity Score; JTDB, Japanese Trauma Data Bank; NTDB, National Trauma Data Bank; SBP, systolic blood pressure.
Discussion
The present study is the first to evaluate the quality of Japanese trauma care using large trauma registries from Japan and the USA. The results show that Japanese trauma care is largely comparable with that provided in the USA. However, the outcomes for patients who receive a blood transfusion in Japan are worse when compared with those in the USA. Both data sets had relatively low mortality rates compared with those in previous studies, which might be due to our exclusion criteria and the fact that the data were collected in recent years.1 7 However, trauma care quality in Japan is most likely improving with the adoption of various efforts, some of which were mentioned in the Introduction section.
Although it is difficult to compare the performance of different systems of trauma care delivery, the NTDB, which is currently the largest trauma-related registry, is an excellent global benchmark and is useful in the quality improvement process. Several international comparison studies show the potential for assessing the strength and weakness of different systems. In one international comparison study, trauma mortality outcomes were compared between a trauma center in France and the NTDB.7 There are significant differences in trauma management between France and the USA, especially in prehospital care and the initial attending physician who usually does not practice in the prehospital setting in the USA. The Japanese trauma system may be more similar to that in France rather than that in the USA.8 Japanese prehospital care includes ambulance and helicopter medical services with a physician. Thus, physicians can provide the initial resuscitation and make decisions regarding the necessity of surgery at the injury scene. Recently, it has been reported that helicopter transport with a physician is associated with a survival benefit in Japan.9 In another study, in-hospital trauma mortality at a South African trauma center was compared with that in matched patients from the NTDB.10 Compared with that in the NTDB, the South African trauma center had a survival disadvantage in patients with blunt trauma injuries and a lower GCS score. Thus, the authors suggested that the outcome of traumatic brain injury may be improved by creating specific protocols.10 Similarly, we found that the JTDB had a significantly higher mortality among patients who received a blood transfusion compared with that in the NTDB. There must be a specific reason for this difference and room for improvement. Finally, another international study compared outcomes of severely injured patients between a South Korean trauma center and the NTDB, and found that the implementation of a trauma system in South Korea improved trauma mortality.11 The trauma system in South Korea comprises trauma centers and was established nationwide in 2012. Japan does not have a trauma system with nationwide coverage or trauma centers as typically defined; instead, ECCCs play an alternative role. However, the facility criteria are not specific for trauma care and are very vague regarding staff assignments (online supplementary file 2). The implementation of a trauma system with government and public support could significantly improve trauma outcomes in Japan as well. Additionally, by comparing trauma outcomes in Japan with those in the USA, we were able to identify important issues for quality improvement.
Supplemental material
There were large differences in the patient characteristics between the two countries. The most notable finding concerned the differences in the etiology and mechanism of injury. Given that Japan has a high suicide rate and a very low violent crime rate, the finding that the JTDB had a higher rate of self-inflicted injuries and fewer assaults and GSWs compared with that in the NTDB is remarkable.12 The second notable finding was the large difference in age distribution. As Japan has the highest population of elderly adults in the world, this finding is also important.13 Third, the rate of patients in extremis was higher in the JTDB than in the NTDB. Japanese prehospital providers rarely terminate resuscitative efforts at the scene and during transfer of most traumatic patients, even those with cardiac arrest due to unwitnessed blunt trauma.
Even though the inclusion criteria limited the study population to patients with ISS ≥9, the patients underwent thoracotomy or laparotomy at a very low frequency. Unlike that in the USA, Japan has an extremely low rate of GSWs. Attending trauma surgeons have a limited number of surgery cases in Japan, and this is a major issue in the training of trauma surgeons. Therefore, inhouse attending trauma surgeons are still uncommon and emergency physicians usually provide initial trauma management for severely injured patients in Japan. ECCCs in Japan do not have any facility criteria requiring a surgeon to be present for major resuscitations, which the ACS-COT mandates for trauma center verification.14 Not having an on-call trauma surgeon potentially causes a delay in urgent or emergent surgery.15 However, patients in the JTDB who underwent thoracotomy or laparotomy did not have worse outcomes. On the other hand, patients who required blood transfusion, who may be regarded as patients with active hemorrhage, had worse outcomes in the JTDB than in the NTDB. The lack of an inhouse attending trauma surgeon may cause a delay in surgery for hemorrhage control in Japan. Additionally, a massive transfusion protocol (MTP) still remains uncommon in Japan. Thus, the establishment of an inhouse trauma surgeon and MTP may improve survival outcomes in Japan.
There were large discrepancies in the length of hospital stay between the JTDB and NTDB (18.0 (7.0–35.0) days vs. 5.0 (3.0–9.0) days, before matching). The long length of stay in Japan and short length of stay in the USA are consistent with the Organisation for Economic Co-operation and Development (OECD) 2015 data.5 This result may be due to differences in the healthcare system between Japan and the USA. The OECD reported that Japan has the highest number of hospital beds per capita, nearly five times as many as that in the USA (13.2 vs. 2.8 per 1000 people); however, healthcare spending in Japan is less than that in the USA (11.4% vs. 16.6%, as a share of the gross domestic product). The self-pay burden of patients is also low in Japan, as Japan has a universal health insurance system and the High-Cost Medical Expense Financial Plan extends to almost all citizens.16 Therefore, most trauma patients and families hope to stay in the hospital for as long as possible in Japan. In fact, Japan has the highest average length of stay in the OECD countries (17.2 days). Similarly, the ICU length of stay was statistically longer in JTDB than in the NTDB; however, the difference was small compared with that for the length of hospital stay (3.0 (1.0–11.0) days vs. 3.0 (2.0–7.0) days, before matching). This may be due to that fact that decisions regarding ICU discharge made by emergency physicians are largely independent of the patient’s wishes.
In spite of a lack of a large difference in overall mortality between the two countries, it appears that the treatment strategy differs between Japan and the USA. There is one aspect worthy of note: the use of diagnostic imaging. CT scans were used nearly 35% more often in the JTDB than in the NTDB cohort. These data suggest that CT may be overused in Japan. Several reasons have been proposed for the higher use of CT in Japan. First, most Japanese ECCCs are equipped with high-speed CT scanners located very close to the trauma bay. In recent years, several hospitals have also installed hybrid emergency room-enabled interventional radiology systems. This technology has dramatically reduced the time required for completion of CT scans in Japan.17 Thus, most Japanese emergency physicians will readily consider CT as safe as long as the patient has preresuscitation SBP greater than 75 mm Hg.18 Trauma surgeons do not necessarily attend the initial care for severely injured patients in Japan. Therefore, there may be enough time to undergo CT scanning before the completion of the definitive surgical assessment. Although an overuse of CT scanning becomes an issue of facility resources and cost, CT scanners are widely available, cost is moderate, and reimbursed by the universal health insurance in Japan. Japan has the highest number of CT scanners in the world, more than twice as many as those in the USA (101 vs. 44 per million people).5
The present study has several limitations, including its retrospective nature. Additionally, although exact matching was performed to minimize confounding effects, there may be other unmeasured confounders. For example, Japan has the highest life expectancy in the world.5 Therefore, patients included in the JTDB may be in better physical health than those in the NTDB data set. Furthermore, the data sets have other potentially important differences, including social, economic, and racial differences. As for trauma management, differences in clinical protocols largely depend on each hospital, as well as the care delivery system in each country. These factors may strongly affect overall outcomes. Furthermore, both data sets have a number of limitations. They comprise voluntarily submitted data from hospitals that are actively involved in trauma care (convenience sample). Furthermore, the injury-related data have variability and inaccuracy in scoring.19 The JTDB also lacks a data verification system. Therefore, selection and information biases are evident. Additionally, in-hospital mortality was the only outcome evaluated. The in-hospital mortality may underestimate the importance of other patient outcomes to a greater extent in the NTDB compared with the JTDB because the JTDB had a significantly longer hospital length of stay than that in the NTDB. Finally, the NTDB may have higher rates of occult injuries due to a lower use of CT scans. Therefore, the ISS in the NTDB may be underestimated. Despite these limitations, the present study clarifies differences in clinical practice with a national perspective. The study results should provide a better understanding of Japanese clinical practices and facilitate international clinical studies.
Conclusions
In the present study, we reported marked differences in trauma care between Japan and the USA. Japanese trauma care appears to be adequate for patients with stable circulation, high GCS score, and mild traumatic brain injury. Despite these strengths, it is important to note the apparent weakness in trauma care for patients who undergo blood transfusion. The differences in trauma outcomes between Japan and the USA may be related to differences in the use of diagnostic modalities and trauma surgeon’s presence in the resuscitation room, as well as the experience with penetrating injury mechanisms. In summary, the quality of the recent Japanese trauma care appears to be approaching that of the USA; however, the establishment of a mandatory inhouse trauma surgeon as well as the development and implementation of MTPs may further improve Japanese trauma care.
Footnotes
Contributors Study conception and design: SM, KJ, RC. Acquisition of data: SM, KJ, AS. Analysis and interpretation of data: SM, AS, MY, RC. Drafting of the article: SM, RC. Critical revision: SM, KJ, RC, MK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This retrospective study was approved by our institutional review board (UCSD Human Research Protections Program, Project #151611X).
Provenance and peer review Not commissioned; internally peer reviewed.