


The public system of health care insurance that exists in Canada today was implemented nationally in 1968 and was greatly influenced by the 1964 Royal Commission on Health Services, headed by Justice Emmett Hall. When, in his final report, Justice Hall described the evolution of health care in Canada, he made brief reference to a health insurance system that existed in the Glace Bay colliery district of Cape Breton. Known as the “Check-Off,” this was a mandatory system whereby deductions were made from miners' wages for a subscription to physician services, medications and hospital care. A reference to the Check-Off in minutes of the Nova Scotia Provincial Workmen's Association1suggests that it dates from about 1883, although at least one other historical reference places its origin even earlier, in the mid-19th century.2 It proved to be a durable system, surviving in Cape Breton mining towns until 1969, when it was replaced by provincial medical insurance administered by Maritime Medical Care.
One of us (C.M.) was first introduced to the Check-Off system by a Halifax-based surgeon, Dr. Allan MacDonald, who had done some general practice locums in Glace Bay in the 1960s. He suggested an interview with Dr. Joe Roach, a veteran of the system, who at 83 was still seeing 11 000 to 12 000 patients a year and doing regular house calls. In researching the Check-Off system and preparing a CBC Radio documentary,3 C.M. gained information through recorded personal interviews with participants in the system, including patients, physicians, hospital administrators, politicians and union organizers. In this article, we convey the essence of the interviews; the unedited conversations can be accessed through the Dalhousie University Medical Humanities Web page (www.library.dal.ca/kellogg/subjects/medhumanities/cbcheckoff/intro_cbcheckoff.htm).
The Check-Off system reflected the paternalistic philosophy of the times.4 The coal company built and owned the houses in the town, the power plant, the water facility and the grocery stores. The employer deducted from each miner's weekly pay the costs associated with daily life, including rent, water, sanitation, supplies, coal, company store bills and check-weighman (see Fig. 1). (The check-weighman would verify the weight of each miner's load of coal to determine how much money he would make. Miners were paid according to the amount of coal they extracted each day.) The Check-Off evolved to include union dues, relief associations, and physician and hospital services.
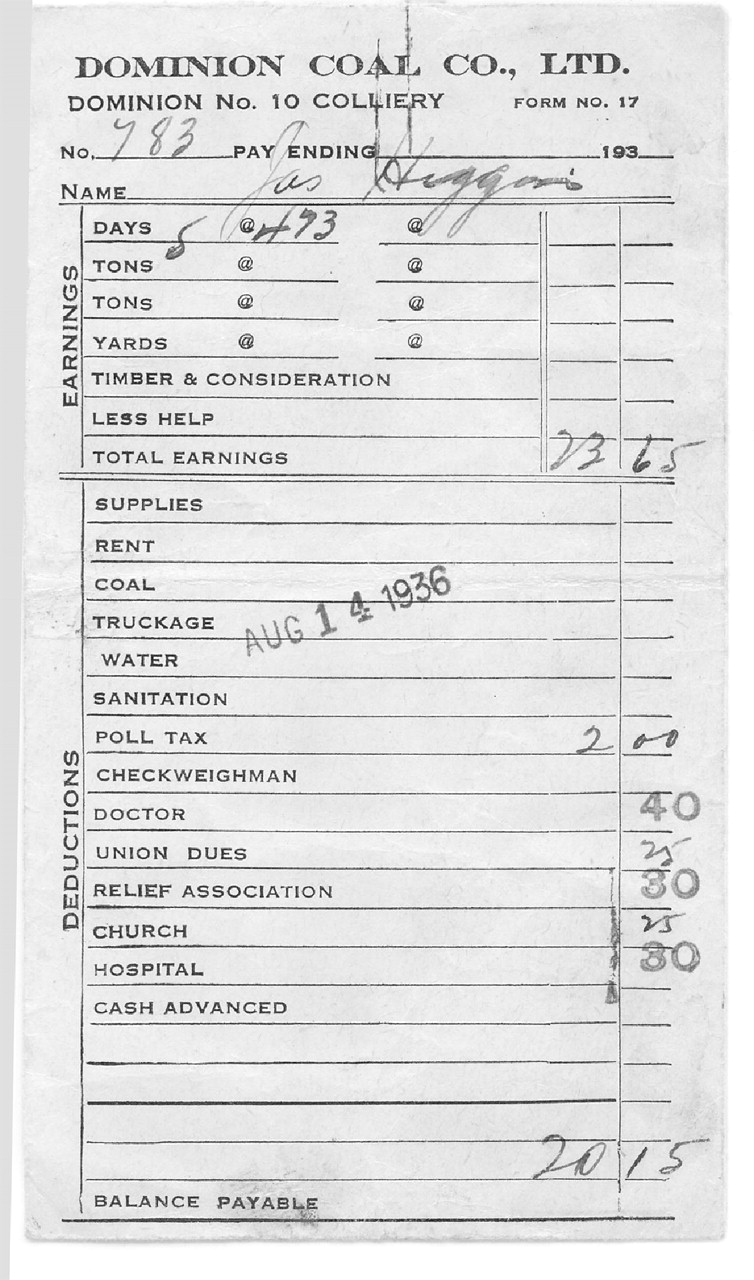
Fig. 1: Weekly pay packet of a Dominion Coal Company miner from the Dominion No. 10 colliery, dated Aug. 14, 1936. Deductions for doctor and hospital were 40 cents and 30 cents, respectively. The balance payable, if present, would be included inside the pay packet.
Deductions for physician and hospital services became a condition of employment with the Dominion Coal Company that continued in superseding companies. New workers were obliged to select a doctor and hospital in the area for subscription when they signed on with the company; this entitled them to unlimited physician visits, a range of medications, surgical procedures and supplies, and hospital services. However, if a miner required medical attention that could not be provided by the subscribed doctor and hospital, he was responsible for the fees.5
The Check-Off was arranged through the union, so that all miners in the Provincial Workmen's Association, later to become the United Mine Workers Association, were subscribers. The fee was the same regardless of age, medical condition, marital status or number of dependents (who were covered under the worker's subscription).6
Check-Off medical fees were negotiated between the physicians, the union and the coal company. The doctor fee was 40 cents per week and the hospital fee 50 cents per week until the early 1950s, when the doctors rallied for higher pay. In 1952 doctor and hospital fees were both increased to $1. These fees remained in place up until the end of the Check-Off for medical services in 1969.6
The system operated with difficulty during a strike, when Check-Off subscriptions were terminated. The infrastructure of the community was wholly dependent on Check-Off subscriptions, because towns such as Glace Bay consisted mainly of miners and their families. Churches as well as hospitals suffered from the loss of deductions from pay packets (see Fig. 1). One miner recounted how, during a strike in the 1920s, a member of the clergy stood in the pulpit and urged the miners to return to work and take a pay cut in order to reinstate Check-Off subscriptions.7
Technically, only a miner's spouse and children were considered to be dependents, but in reality parents or extended family living in the same household were often covered under the miner's subscription.4,8 The coverage depended on at least one person in the family working in the mine, as did the use of company houses. Miners who were forced to stop working for any period of time were replaced by able-bodied sons, who might be as young as 13.2 If a miner died without a son to replace him, the family would lose their company-owned accommodations and their medical services and would be dispersed among extended family in the area. These women and children would either be covered for medical services as dependents in their new residence or would be treated as charitable cases.
Young men, especially those married with children, were attracted to mine work because the Check-Off system provided their family with health security. A miner's average annual income in the 1940s was just over $1000 and did not vary much over the years.7 Doctor fees were $2 per office visit and $3 per house call under the fee-for-service system that existed outside of the mining communities; it would have been practically impossible for a miner to finance adequate health care for his family without a pre-paid insurance plan.
Even though miners were content to have health insurance, many were dissatisfied with the system that provided it. Miners had little control over their lives and often felt “owned” by the company.7 Since mines were often closed during the winter, miners would accrue debt during this season and often spent the rest of the year paying it off through Check-Off deductions.
The Check-Off system was a form of group practice plan whereby a “panel” of doctors entered into a contract with the coal company and the miners' union to provide medical care to subscribed families. In the 1940s, these panels covered 460 to 1190 families, so that a total of 8 doctors would be responsible for 13 000 to 14 000 patients.2 However, in the 1950s and 1960s, doctors reported that each panel included 1500 to 4000 miners9 with an average of 6000 to 7000 patients in a practice.8
With such large practices, it is not surprising that physicians felt overworked. A 1944 study2 compared the caseload of physicians working under the Check-Off system in Glace Bay with the caseload of those working in a fee-for-service system in Yarmouth, NS. Over the 1-year study period, doctors attended to an average of 10 977 cases in Glace Bay, compared with 3644 in Yarmouth: practically a 3-fold difference.2 Doctors in the Check-Off system were obliged to attend to any and all patients in their panel; on call 24 hours a day, 7 days a week, they were often overwhelmed by the pace.6 Also of note is the difference in the number of house calls performed by doctors in Glace Bay and Yarmouth: “1000 persons under [a Check-Off] insurance scheme receive 64 percent more in the way of doctors' calls — that is, office, home and night calls taken together — than a group of similar size lacking insurance protection.”2 One physician recalled performing 145 house calls on one day with a colleague during an influenza epidemic in December 1956.6 Another estimated that he made an average of 40 to 50 house calls a day.9
In the 1940s, the average family size in Glace Bay was 4.7 people; wage earners made up 27% of the patients covered by a panel.2 With a fee of 40 cents per week per miner, doctors were remunerated less on a per-patient basis than were their colleagues in the fee-for-service system. Although doctors under the Check-Off system worked comparatively harder than those in the fee-for-service system, their total incomes were comparable: fee-for-service physicians were often not paid for their services. During the Depression, a Nova Scotian physician practising outside of Halifax and the South Shore would be remunerated for about 30% of his services.8 The Check-Off system, on the other hand, provided physicians with a secure income, even if they ended up receiving less money per visit.
In the early 1900s, there were very few specialty-trained physicians in Nova Scotia. General practitioners handled all of the obstetrics, pediatrics and surgery cases. During the 1950s, when specialization was growing, specialists were attracted to Halifax and Sydney but not to Glace Bay: the Check-Off system was not organized to pay specialists. To an extent, the Check-Off did not allow for the evolution of health care; its fixed funding would not have sustained quality of care during the boom of medical technology that began in the 1960s.
Did the Check-Off system influence the development of Canadian medicare? The Hall Report mentions the Cape Breton coal miners' pre-paid insurance plan as a matter of historic rather than current interest. Tommy Douglas, the founder of Canada's first provincial health care insurance plan, is reported to have visited Glace Bay on several occasions in the 1960s as leader of the federal Cooperative Commonwealth Federation (CCF).10 However, he did not seem to be influenced by the Check-Off system in his fight for national health care insurance. Mr. M.J. Coldwell, Tommy Douglas' successor as leader of the CCF, made a speech in Glace Bay during an election year. Before taking the podium, he was approached by a group who informed him of the Check-Off system and suggested that miners might not be interested in national health care insurance, as they already had their own system. He was unaware of the Check-Off before arriving in Glace Bay and is reported to have replied, "Whether it goes well or not, if I'm elected Prime Minister of Canada, you're going to get medicare, including the Glace Bay miners." 10 Senator Allan MacEachen, who was federal minister of health when national medicare was implemented in 1968, came from the mining town of Inverness in Cape Breton and, as the son of a miner, knew the Check-Off system well. However, he considered it a stretch to imply that the Check-Off system had an impact on the evolution of Canadian health care insurance.3
When medicare replaced the Check-Off system in Cape Breton, miners no longer paid their weekly subscription to doctors. The Check-Off for uninsured health services persisted until it was replaced by a commercial insurance plan (Great West).11 Under medicare, Check-Off doctors' incomes tripled and quadrupled overnight. Doctors didn't change their work habits and continued to cover a practice of 6000– 7000 patients. As a result, Nova Scotia Medical Services Insurance (MSI), now responsible for the doctors' incomes, would frequently send down investigators, doubting that these mining-town doctors could possibly see as many patients as they claimed.
The Check-off system was the first comprehensive medical insurance program established in this country, and it provided total medical coverage to its subscribers and their families, close to 100 years before medicare. It functioned well as a small system but, at its end, struggled with modernization. It could not have coped with the rapidly increasing costs of health care in recent years. Although the model of health care delivery chosen for medicare was not that of the Check-Off system, MacEachen admitted, in the CBC Radio documentary, that “the technique maybe was not applied, but I think the attitude, or the philosophy behind it, may have had some relevance, namely that a group effort to provide services had possibilities that individual efforts could not achieve.” 3
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

