

Intramuscular lipoma
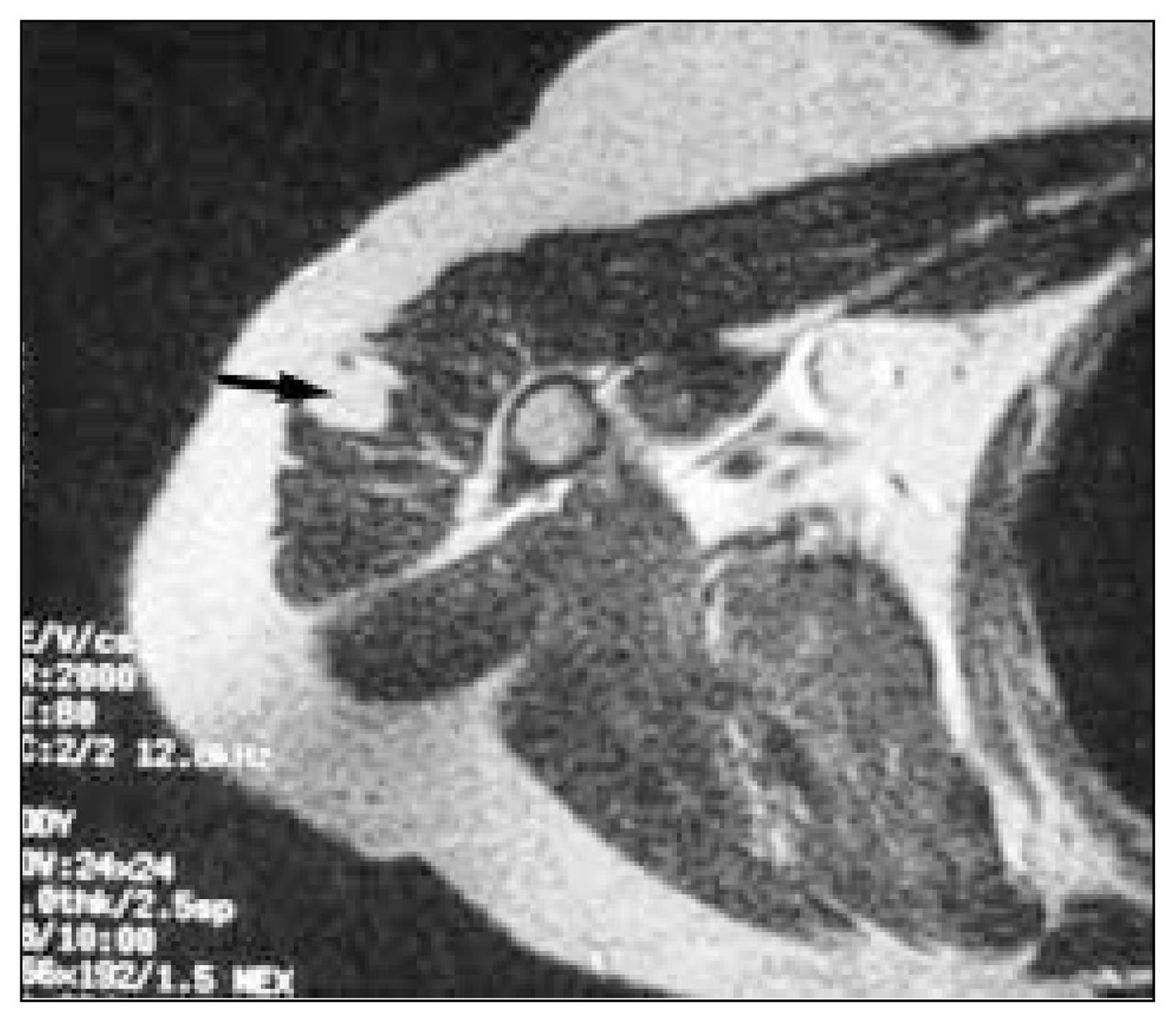
The axial computed tomography scan (Fig. 1) revealed a hypodense, well-defined lesion (arrow) within the deltoid muscle at the level of the humeral neck. The lesion was similar in attenuation to adjacent subcutaneous fat.

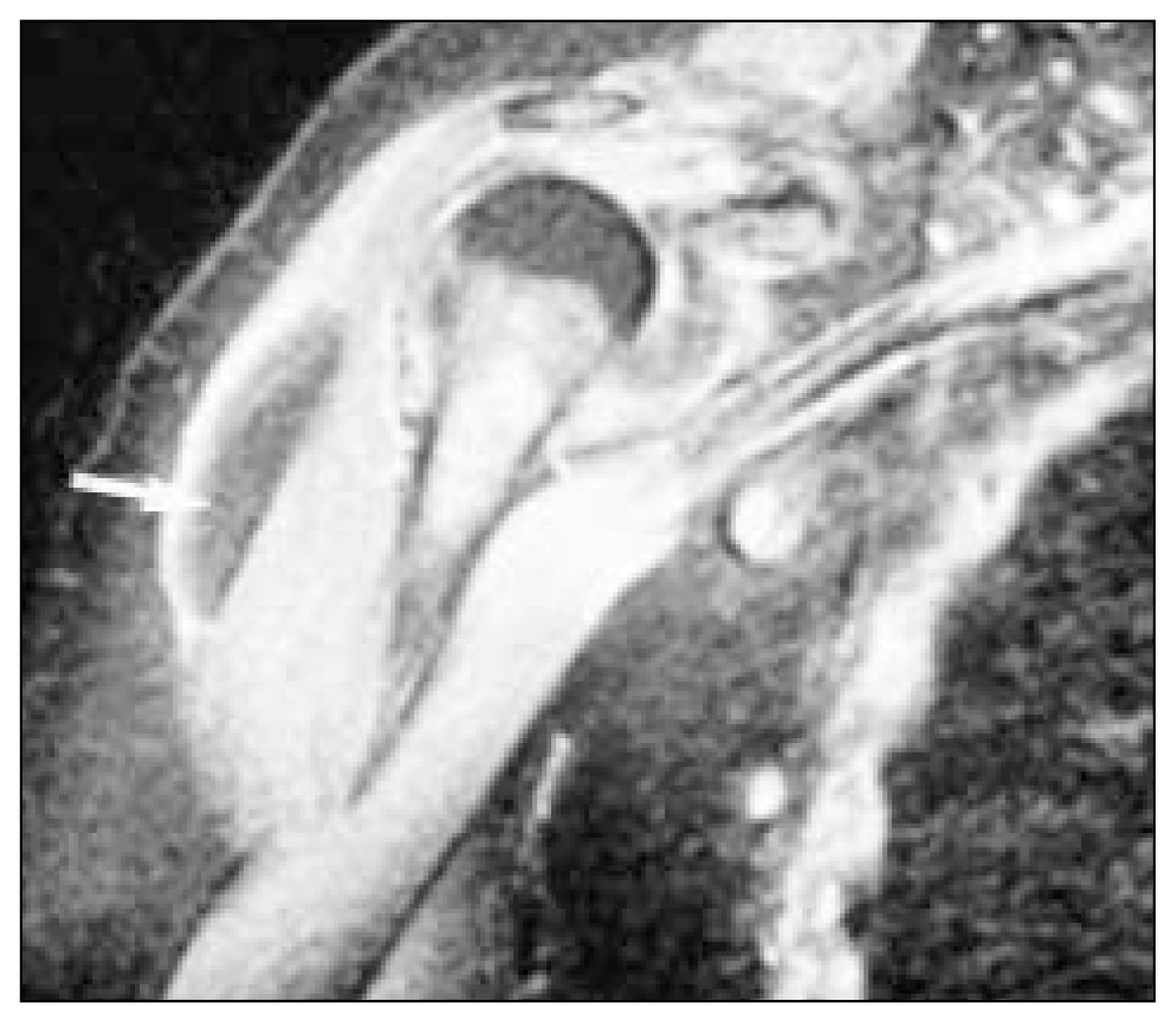
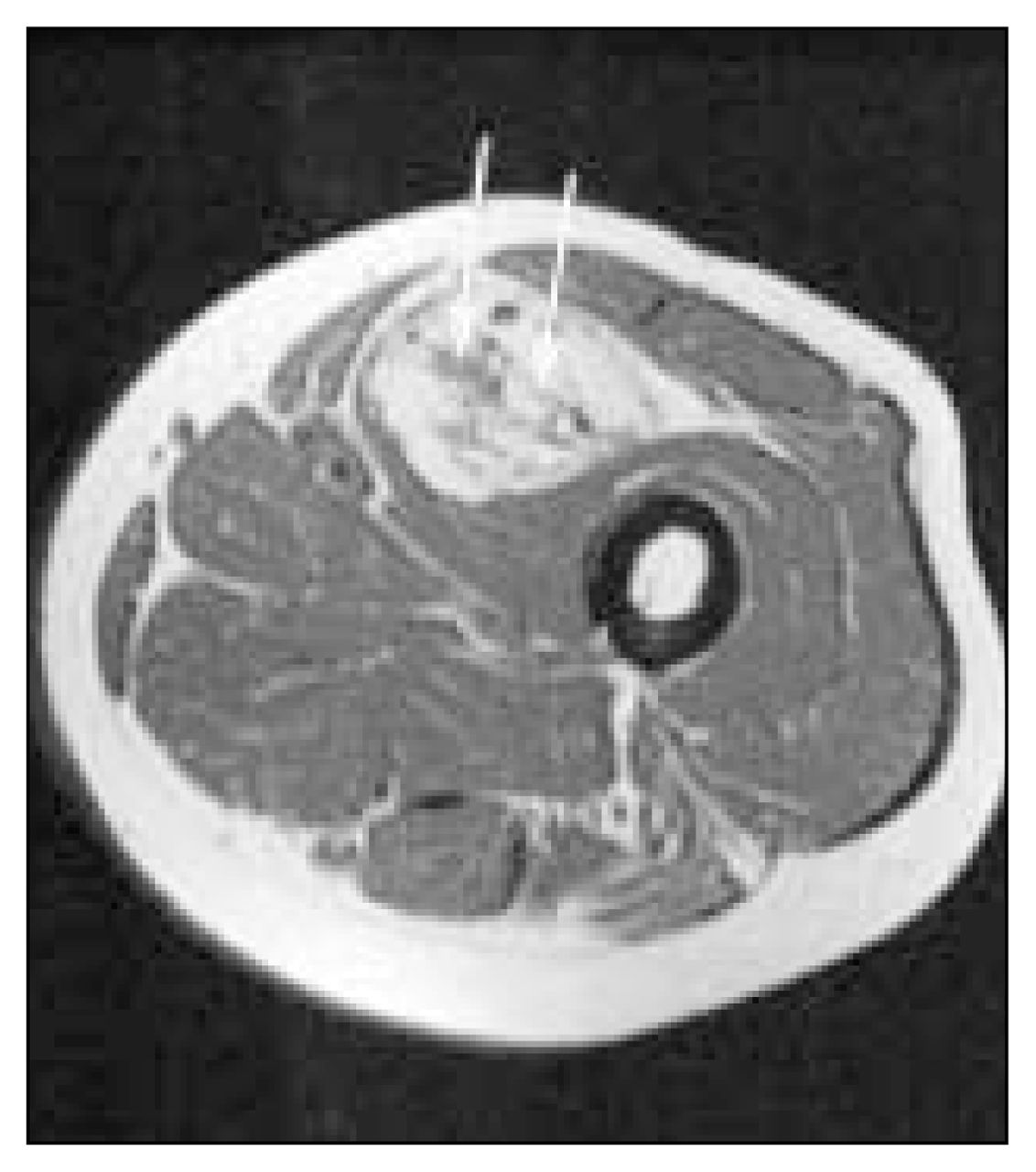
The T1-weighted coronal oblique magnetic resonance image of the area (Fig. 2), obtained for further assessment of the lump, demonstrated a well-defined hyperintense area (arrow) within the deltoid muscle, of similar signal intensity to adjacent fat. The hyperintense nodule (arrowhead) on the skin is a vitamin E capsule used to mark the area of interest. A fat-soluble vitamin, it has the same signal characteristics as fat within the body. On axial T2-weighted (Fig. 3) and proton density-weighted (not shown) images, the lesion (arrow) again had similar signal characteristics to fat. A fat-suppressed coronal oblique scan demonstrated suppression of the signal from the abnormality (Fig. 4, arrow).


Lipomas, the most common benign soft-tissue neoplasms, can occur in any soft tissue that contains fat, including subcutaneous tissue, muscle, nerve and synovium, or adjacent to bone in the periosteum.1,2 People of any age group can be affected, although lipomas are more common in adults, with a slight male preponderance.3 Lipomas in muscle may be intermuscular or intramuscular and may not be recognized clinically unless they are large or symptomatic. Dysfunction of the muscle or pain (lipoma dolorosa) is rare.
If the lipoma is large enough, plain radiographs may reveal a relatively radiolucent lesion within the muscle, but computed tomography and magnetic resonance imaging scans better demonstrate the lesion. Lipomas should approximate to fat on all imaging sequences. In general they appear as homogeneous, sharply defined fatty masses.1,3 Septations, which may be thin fibrous bands or thicker muscle bundles, are not uncommon in intramuscular lipomas but may make it impossible to rule out well-differentiated liposarcoma on the basis of imaging alone.4 Fig. 5 is a T1-weighted MR image of a different patient with a biopsy-proven, moderately well-differentiated liposarcoma. Note that the lesion’s signal is predominantly of fat, but it has areas of banding and thick septations within.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intramuscular myxoma and peripheral nerve sheath tumours may present as low-density masses on CT and simulate intramuscular lipoma.3 The measured CT attenuation values are usually not quite as low as those of subcutaneous fat (< –80 Hounsfield units). MR imaging can readily distinguish these lesions from lipoma. If doubt persists on imaging, surgical excision is required.