


Abstract
Background: Trauma centres continue to evolve with respect to clinical care and their impact on public health. Despite improvements in patient outcomes, operative volumes, and therefore maintenance of surgical skills, has become a challenging issue. We sought to determine whether injury demographics and treatments at a high- volume centre changed over time.
Methods: We used the Alberta Trauma Registry to analyze all severely injured (injury severity score [ISS] ≥ 12) patient admissions over a 16-year period (1995–2011).
Results: Of the 12 879 severely injured patients requiring admission, there was a 1.5-fold increase in the annual admission rate despite population normalization (p = 0.001). Over the 16-year interval, patients were older with a subsequent lower mortality (p = 0.001) and length of hospital stay (p = 0.007). In patients with the most severe ISS (≥ 48), there was no change in mortality (27%, p = 0.26). In 2011, falls were the most common mechanism compared with motor vehicle crashes (41% v. 23%; p < 0.001); this was a complete reversal compared with 1995 (25% v. 41%). Motorized recreational vehicle and motorcycle injuries also increased (p < 0.001). The mean number of operations performed by trauma surgeons decreased (laparotomies: 67 [17%] in 1995 v. 47 [5%] in 2011, p < 0.001). Thoracotomies and tracheostomies remained unchanged (p = 0.19).
Conclusion: Clinical care has improved despite an increasing overall volume of severely injured patient admissions. The number of operative interventions performed by trauma surgeons continues to decrease concurrent to a change in injury mechanisms. Despite these improvements, maintenance of technical skills among trauma surgeons has become an important issue.
Over the past 16 years, important advances in the care of injured patients have occurred. These include, but are not limited to, the development of regionalized trauma referral centres,1,2 recruitment of trauma fellowship–trained surgeons (trauma team leaders [TTLs]), integration of trauma nurse specialists, improvements in the fidelity of diagnostic imaging,3–5 evolution of hybrid/RAPTOR treatment suites6 and numerous clinical advances, such as percutaneous techniques for arresting ongoing hemorrhage and repairing vascular structures,7 damage control resuscitation,8 nonoperative therapies for solid organ injuries and improved methodologies for achieving same-hospital-stay abdominal fascial closure. This list does not even begin to reflect additional updates in the field of surgical critical care.
Despite a perceived reduction in operative caseloads over time, clinicians at many high-volume centres believe they are receiving an ever increasing total volume of referrals with a subsequent improved survival rate for patients in the most severely injured subgroup. The development of acute care surgery (ACS) in the United States,9 and therefore the acquisition of additional nontrauma operative cases, has been a reflection of both this overall reduction in operative case volumes for faculty and trainees alike and of the challenge to recruit the best residents to the field of trauma surgery itself. Although most ACS services in Canada do not currently incorporate the care of injured patients (i.e., limited to all nontrauma surgical emergencies),10 the issues of faculty operative/technical skill maintenance and resident trainee career choices remain very relevant. Similarly, public health ventures, such as prevention programs, require reflection upon changing injury mechanisms, clinical care and overall volumes.
The aim of our study was to determine how injury demographics and treatment spectrum at a high-volume centre have evolved over time (i.e., volume, severity, length of stay, therapies).
Methods
Study population and data sources
We analyzed aggregated population-level data from the Alberta Trauma Registry over a 16-year period (1995–2011). This registry has been previously validated for accuracy.11 The study population consisted of all adults (age ≥ 16 yr) admitted to the Foothills Medical Centre (FMC) after major trauma (injury severity score [ISS] ≥ 12) during the study period. The FMC is a university-affiliated, level 1 trauma centre that provides tertiary care services to all of southern Alberta, southeast British Columbia and southwest Saskatchewan.
Statistical analysis
Using the Alberta Trauma Registry, standard trauma admission (FMC) and treatment epidemiology as well as outcomes data were collected and evaluated. Count data were summarized as frequencies or proportions. A combination of descriptive statistics with linear regression adjusted per year were used to analyze the data. We considered 2-sided p values < 0.05 to represent statistical significance for all evaluations. Two-way scatter plots with overlayed least squares regression fit linear lines were used to illustrate the temporal changes over time. All statistical testing was performed using Stata/IC version 12.0 (Stata Corp.).
Results
Patient, injury and transport demographics
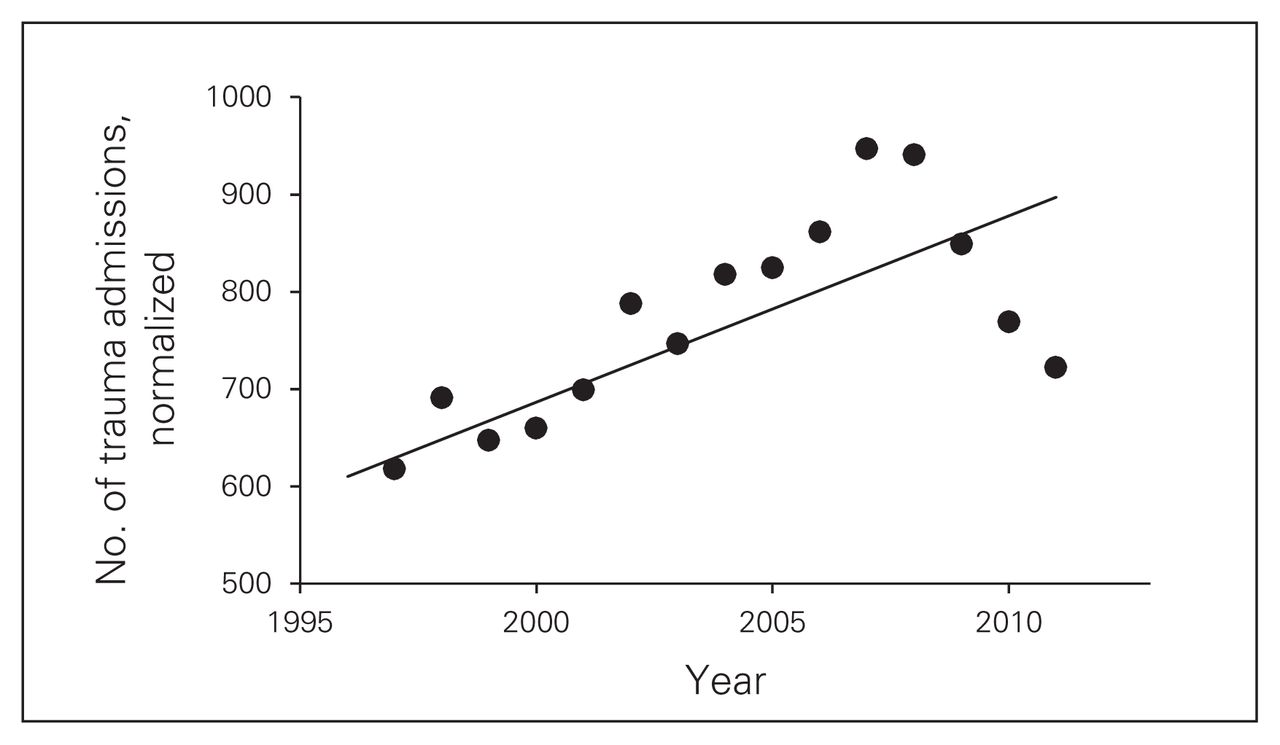
Over the 16-year study period, among a mean population of 1.1 million people residing in the City of Calgary (2.4 million in the FMC catchment area), 12 879 patients with severe injuries were admitted to the FMC (median 827 patients/yr). When normalized by regional population increases, FMC trauma admissions were observed to have increased 1.5-fold over these 16 years. In comparison to 402 admissions in 1995, the trauma service peaked at 1118 admissions in 2008 (p = 0.001; Fig. 1).
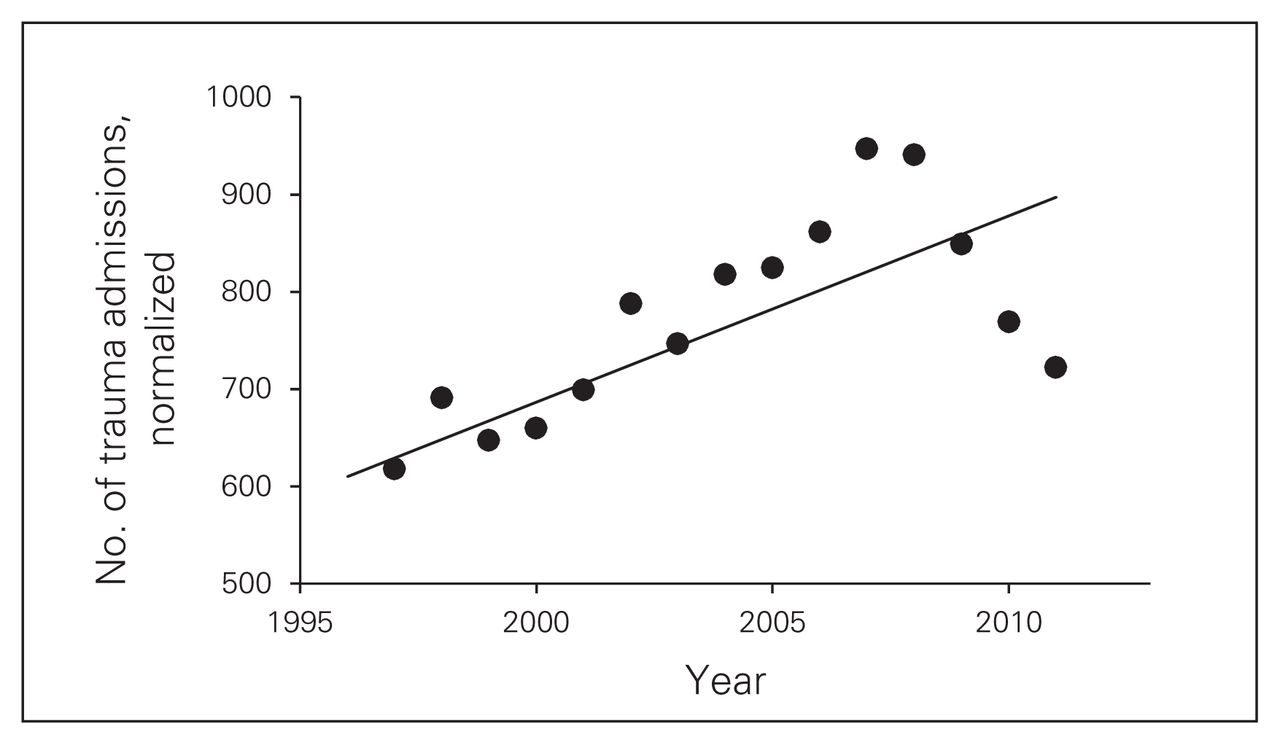
Linear regression model for trauma admissions (injury severity score ≥ 12) to the Foothills Medical Centre over 16 years, normalized for increases in the Calgary regional population.
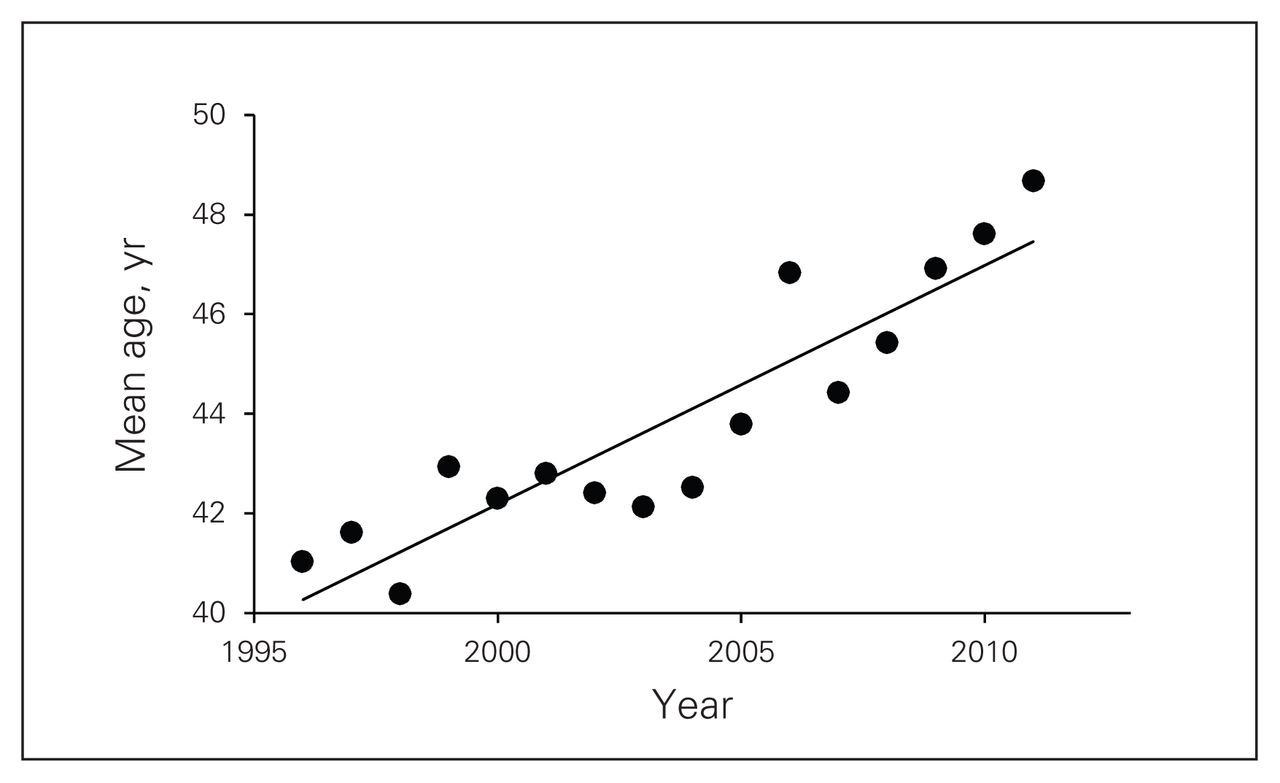
Patients were on average older (mean 44 yr) at the end of the 16-year interval (41 yr in 1995 v. 49 yr in 2011, p < 0.001; Fig. 2). The average ISS remained unchanged (mean 25, p = 0.84) except in patients undergoing a laparotomy (28 in 1995 v. 35 in 2011, p = 0.011). Similarly, the percentage of patients presenting to the FMC with hypotension (systolic blood pressure ≤ 90 mm Hg) remained constant over the study interval (mean 6.1%, p = 0.44). The time of admission to the FMC was also unchanged (03:23, p = 0.53). The mode of transport remained consistent (74% via ground ambulance, 16% via helicopter, 5% via fixed wing, 5% via walk-in/private vehicle; p = 0.39). The number of patients presenting with injuries that occurred at the workplace was also stable (5%/yr, p = 0.59). The specific type of injuries did not change over the study interval (p = 0.44).
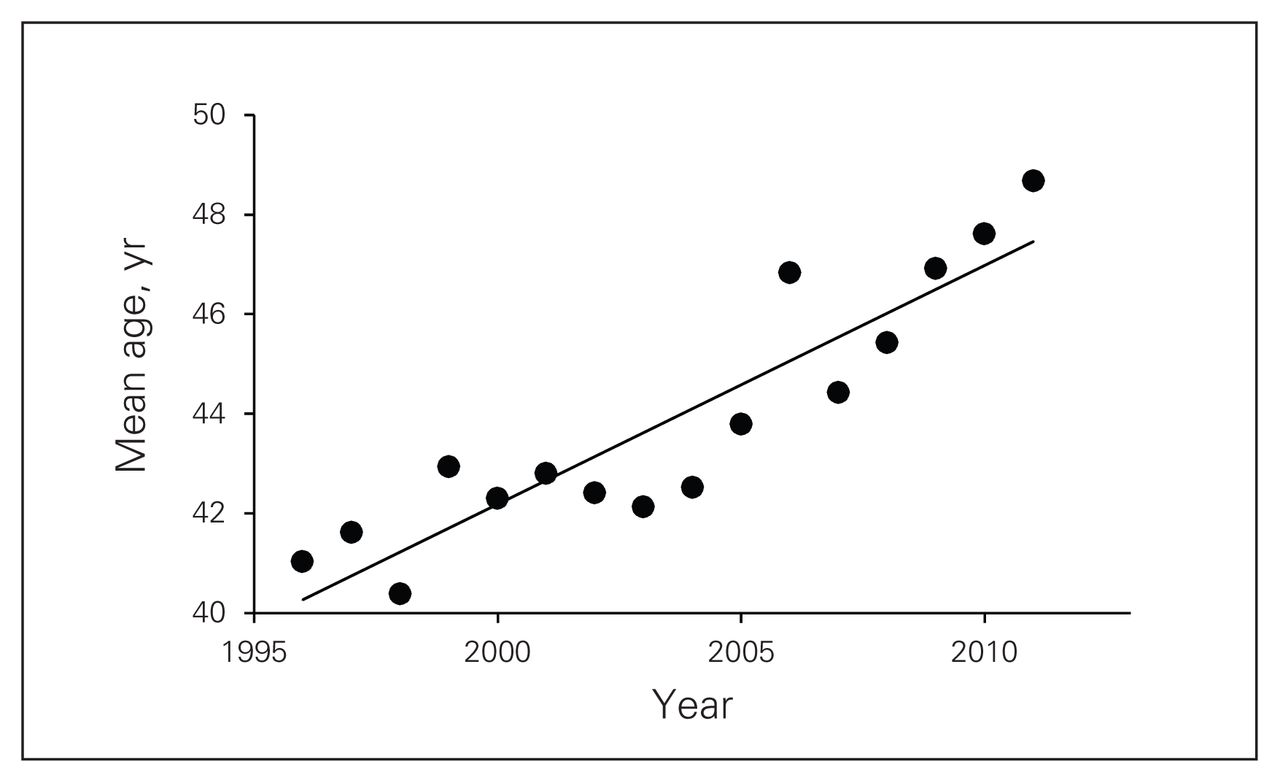
Linear regression model for mean patient age of trauma admissions (injury severity score ≥ 12) to the Foothills Medical Centre over 16 years.
Mechanism of injury
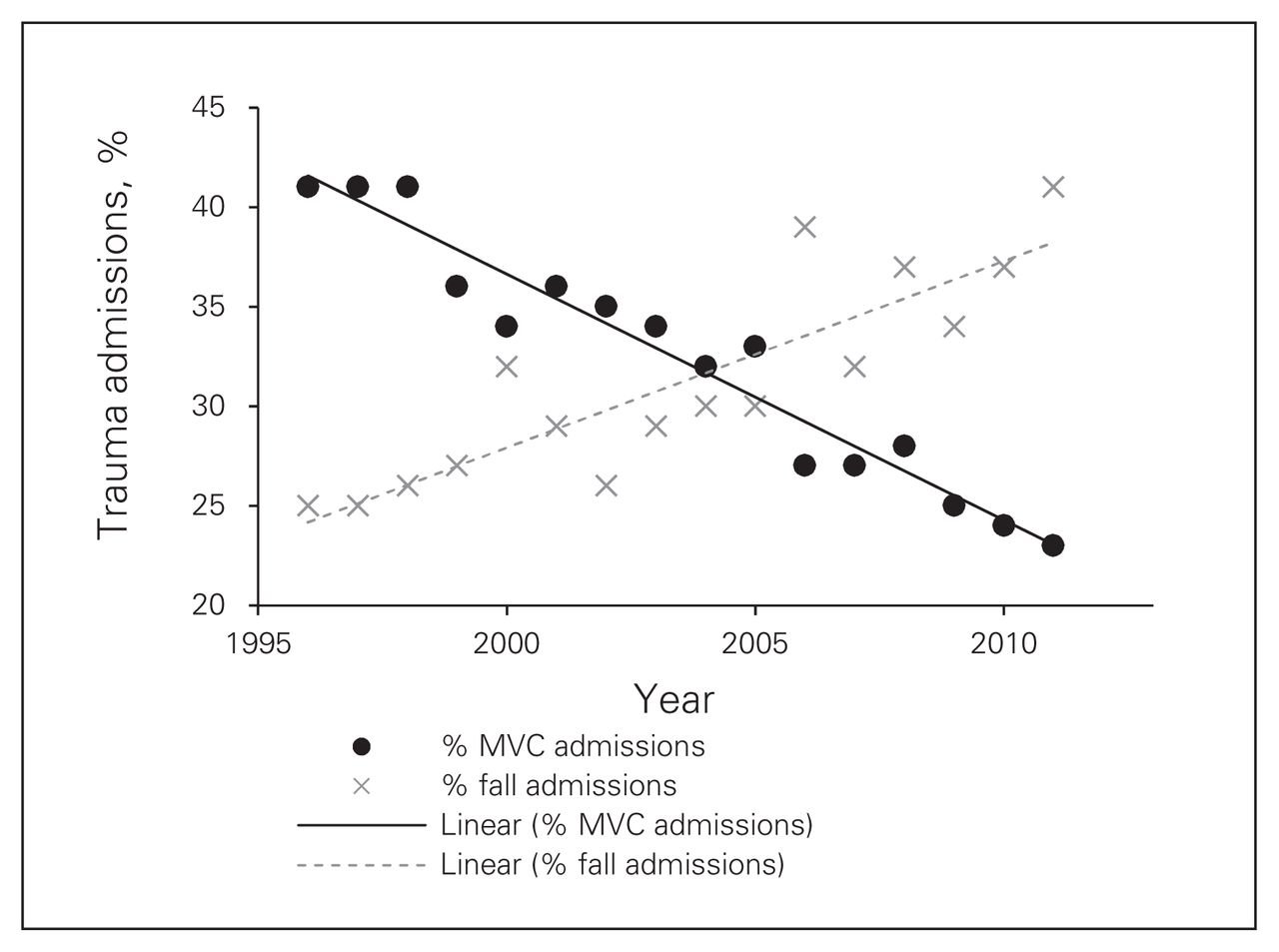
The mechanism of severe injury changed dramatically over the study period. While motor vehicle crashes (MVCs) were the most common cause in 1995 (41%), this decreased by almost half by 2011 (23%, p < 0.001; Fig. 3). Conversely, falls nearly doubled in frequency (25% in 1995 v. 41% in 2011) to become the most common mechanism of injury (p < 0.001; Fig. 3). Motorized recreational vehicle (e.g., all-terrain vehicles [ATVs], dirt bikes, snowmobiles) injuries (1% in 1995 v. 4% in 2011, p < 0.001) and motorcycle injuries (3% in 1995 v. 8% in 2011, p < 0.001) increased significantly. The frequency of penetrating (e.g., gunshots, stab wounds) injuries remained stable (mean 4%/yr, p = 0.24).

Linear regression model comparing motor vehicle collisions (MVCs) and fall trauma admissions to the Foothills Medical Centre over 16 years.
Operative interventions
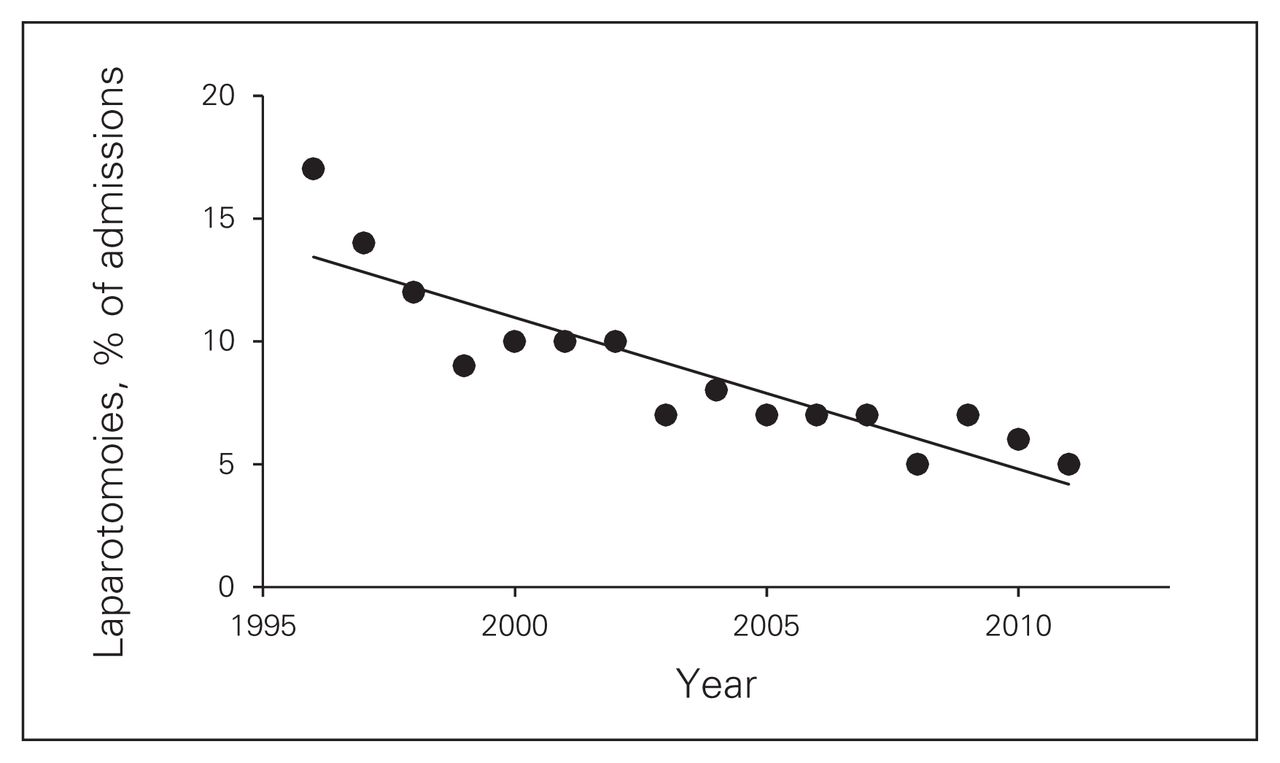
The mean number of operative interventions for the trauma service decreased significantly over the study interval. The rate of laparotomies decreased from 67 (17%) in 1995 to 47 (5%) in 2011 (p < 0.001; Fig. 4). Thoracotomy and tracheostomy procedures remained unchanged (12/yr and 67/yr, respectively; p = 0.19).
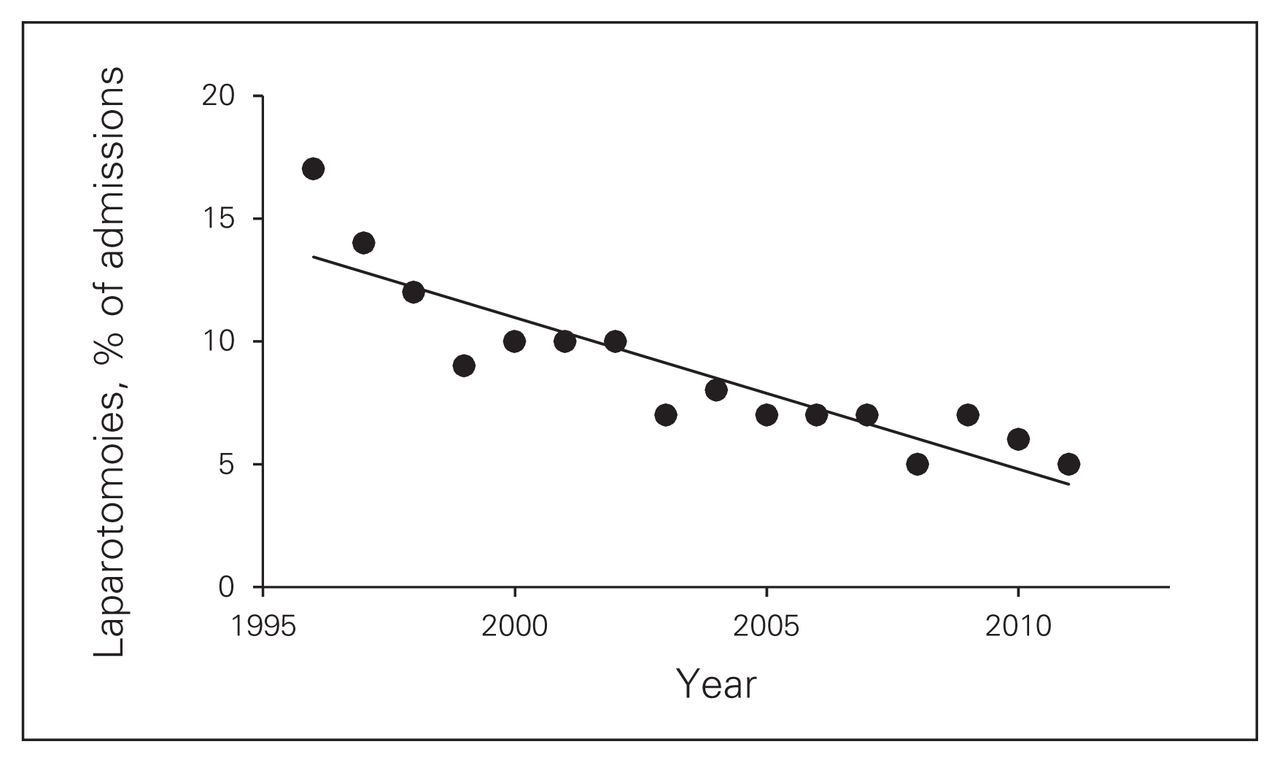
Linear regression model for number of laparotomies performed as a percentage of incoming trauma admissions (injury severity score ≥ 12) to the Foothills Medical Centre over 16 years.
Outcome measures
The mean length of stay in hospital decreased significantly over the study interval (17 d in 1995 v. 13 d in 2011, p = 0.007); however, length of stay in the intensive care unit (ICU) remained unchanged (3 d in 1995 v. 2 d in 2011, p = 0.14). Among all injured patients, the majority (mean 67%/yr) were discharged home. Most of the remaining patients were transferred to a rehabilitation (14%) or acute care (13%) facility. This ratio remained unchanged over the study interval (p = 0.49). Mortality among the study population decreased (15% in 1995 v. 11% in 2011, p = 0.001). In patients with a high ISS (≥ 48), there was no change in mortality over the study interval (mean 27%, p = 0.26). The specific rate varied by surgeon. Mortality among patients undergoing a laparotomy also increased over time (17% in 1995 v. 21% in 2011, p = 0.024).
Discussion
From 1995 to 2011, 12 879 severely injured patients were admitted to the trauma service at the FMC. The year- specific volumes increased in nearly a linear manner to a peak admission total observed in 2008. Although this increase in volume is partially reflective of an absolute increase in the local population, when normalized for regional population changes, the observed 1.5-fold increase remains indicative of concurrent influences. Given the lack of any additional level 1 trauma centres in the region, in addition to a policy of absolute acceptance of all injured patients (regardless of inpatient bed status or service patient volume), we believe that this increase in volume is most reflective of a more complete catchment of injured patients in a large heterogeneous geographic region.
In addition to an increase in overall volume, patients were also significantly older. With a mean age approaching 50 years, patients now present with more comorbidities and a diminished physiologic reserve in scenarios of critical illness.12–14 Although our registry has been historically poor at documenting preinjury health issues, anecdotal experience clearly indicates that we are caring for an older, sicker populace of severely injured patients.13,14 This observation, in addition to the challenges of caring for this population, have been documented in numerous publications throughout North America.12,15
The advancing patient age is also likely reflected in the massive increase in the number of severely injured patients admitted after falls. This single mechanism is now the most common etiology for admission by a substantial volume. Conversely, the proportion of MVC-related admissions has decreased substantially over the past 16 years. This evolution most likely reflects the population-based public health benefits from improvements in both motor vehicle and civil engineering as well as from injury prevention legislation. Interestingly, a notable increase in motorized recreational vehicle (ATVs, motorcycles) trauma was also identified. As previously outlined, we believe this is likely a reflection of increased disposable income in an area of economic affluence.16 Active public health program measures for both fall prevention and recreational vehicle safety are now underway at our centre (media and legislation).
Despite the increasing age of injured patients, both the overall length of stay in hospital and mortality decreased significantly over the study interval. When taking into account the stability in the proportion of patients presenting with hypotension and in their associated ISS, prehospital transport and discharge destination, the noted improvement in mortality is likely secondary to improved volume outcomes within the trauma centre itself. This includes, but is not limited to, increased frequency of nonoperative therapies, increased expertise in trauma-specialized nursing and critical care as well as in rehabilitation therapy and system processes. It was interesting to note that there appeared to be no improvement in mortality among the most critically ill patients (ISS ≥ 48). This score represents the most severely injured subgroup in any trauma system and is arguably a measure of trauma surgeon/TTL performance at the most sensitive and critical time points.
Although trauma surgeons cared for more injured patients per year, the overall number of operative interventions decreased dramatically over the study period. More specifically, the number of laparotomies showed a relative reduction of 70% to approximately 5% of all trauma admissions. This observation represents a significant improvement in patient care and follows evidence-based guidelines consistent with the proliferation of nonoperative therapies. While other types of operative cases (e.g., thoracotomy, tracheostomy) remained stable, this significant decrease in operative experience among trauma surgeons represents a sensitive skill maintenance issue. More specifically, trauma surgeons are required to perform potentially complex operative therapies in physiologically challenged patients on an increasingly occasional basis. Although clinicians may practise preoperative decision-making via simulators and triage scenarios, actual operative technique and rapid intraoperative decision-making relies on limited preceding exposure and maintenance of advanced technical skills (i.e., elective practices).17,18 This issue is also highlighted by the observation that both the mean ISS and mortality of patients who required a laparotomy increased over time. The issue of limited ongoing experience is also apparent to trainees who have increasingly deflected away from making career choices to become trauma surgeons.19 These 2 dominant issues (operative case load and skill maintenance) have been significant factors in the development of ACS services in the United States.8,18–20 In Canada, one can make a similar argument that in centres where ACS is not directly integrated with the trauma service owing to volume concerns (most centres), maintenance of skills must be maintained by active involvement in a critical threshold of ACS service weeks and complex cases. The exception to this principle may potentially occur when an atypical trauma surgeon of note has a large, complex intra-abdominal elective practice.
Limitations
Our study has important limitations. First, as a result of the aggregated or ecological nature of the data, our results can only be interpreted as associations on a population level and, therefore, not causative at the individual level. Second, although we observed a decrease in mortality, specific assertions as to causal relationships cannot be reliably confirmed. Third, we cannot accurately comment on the impact of alcohol consumption over the study interval. In a recent study21 only 63% of our patients were tested. Of these, 30% had a blood alcohol level above the legal limit. It is unclear if this rate has changed over time. Finally, although the data trends support anecdotal concerns for recruitment and operative skill maintenance, there is no direct evidence available at the present time to confirm these possibilities. A national manpower analysis is currently underway by our group to better understand these issues.
Conclusion:
Despite an increasing overall volume of severely injured patient admissions, the number of operative interventions performed by trauma surgeons has decreased substantially. This represents a potential issue with regard to both the maintenance of technical skills and to the recruitment of high-quality residents to the field itself. With the continued advancement of percutaneous and nonoperative therapies, these issues may become even more problematic. A strong association between trauma and ACS services (regardless of whether their actual delivery is distinct or combined) will offer benefits with regard to both of these challenges. From an overall trauma system point of view, however, the quality of patient care has improved within the setting of increased patient volumes and age as well as comorbidities and changes in mechanism of injury. Future public health prevention strategies should reflect the increased prevalence of costly falls and recreational vehicle injuries.
Footnotes
This manuscript was presented at the Trauma Association of Canada (TAC) scientific conference on Apr. 12, 2013, in Whistler, BC.
Competing interests: None declared.
Contributors: C. Ball, D. Das and D. Roberts designed the study. C. Ball, D. Das and C. Vis acquired the data, which C. Ball, D. Das. D. Roberts, A. Kirkpatrick and J. Kortbeek analyzed. C. Ball, D. Das and D. Roberts wrote the article, which all authors reviewed and approved for publication.
- Accepted June 18, 2014.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.