


Abstract
Background: A novel symmetric posterior condylar design and option of a femoral component with an outer zirconium oxide layer were introduced to a successful asymmetric condylar total knee arthroplasty system in 2005. Given the paucity of information on this modified design, we performed a study to determine its early to midterm survivorship and performance.
Methods: Patients who received the Genesis II Symmetric Posterior Condyle or Legion Primary total knee (cobalt–chromium [CoCr] or oxidized zirconium–niobium [OxZr]) (Smith & Nephew) implanted at the study centre between March 2007 and December 2013 were enrolled into a prospective database. We retrospectively reviewed the database and performed survival analysis using Kaplan–Meier techniques.
Results: There were 2178 patients (1359 women [62.4%]; mean age 64.6 yr; mean body mass index 35.0) with 2815 knee replacements available for analysis. Survival rates were 98.2% (95% confidence interval [CI] 97.6%–98.7%) for failure for any reason at 2 years and 96.8% (95% CI 96.0%–97.7%) at 5 years. Age (hazard ratio [HR] 0.97, 95% CI 0.94–0.997) and female sex (HR 0.45, 95% CI 0.27–0.75) were protective, whereas body mass index (HR 1.02, 95% CI 0.99–1.05) and OxZr implant (HR 1.11, 95% CI 0.57–2.18) did not influence survivorship. Oxford Knee Score values improved from a mean of 40.2 to 21.8 by 2 years (p < 0.001), with no difference between the CoCr and OxZr groups.
Conclusion: The symmetric posterior condylar posterior-stabilized knee offers excellent midterm survivorship. Implant bearing surface did not have an influence on survivorship to 5 years, and, thus, use of OxZr implants may not be justified.
The Genesis II (Smith & Nephew) total knee implant system was released to the general market in 1996 and since its release has experienced good overall performance. Case series from the design surgeons1,2 as well as registry data3,4 have shown excellent survivorship and functional results in patients undergoing primary total knee replacement with this system.5 The original system uses built-in external rotation of the femoral component in an attempt to optimize patellofemoral tracking, minimize the risk of femoral notching and prevent tibiofemoral shear forces in extension and flexion.1 Design variations were introduced into the system in 2005 to accommodate a condylar-constrained polyethylene insert requiring a symmetric posterior condyle design. This variant was initially branded as the Symmetric Posterior Condyle and later as the Legion Primary. In an effort to reduce wear, the components were made available in both standard cobalt–chromium (CoCr) bearing as well as an oxidized zirconium–niobium (OxZr) gradient ceramic bearing surface. The OxZr implants are predominantly zirconium–niobium metal with a 4- to 6-mm gradient layer of zirconium oxide on the articulating surface.6 Proposed benefits of the more expensive oxidized zirconium surface are increased wettability,7 decreased peak roughness, 8 decreased adhesive and abrasive wear,7 and its applicability in patients with known metal sensitivities given the absence of nickel in the base alloy.9–11 The tibial component of this device is a titanium–aluminum–vanadium alloy that does not have the issue of nickel as seen in CoCr alloy femoral components.
There have been reports of seemingly minor changes in implant design having effects on overall survivorship and revision rates in both hip and knee arthroplasty.12,13 These occurrences show the need to critically evaluate the effect of minor design changes on implant function and survivorship.
Given the paucity of information regarding the survivorship of this iteration of these modifications to a successful design, we performed a study to determine the early to midterm survivorship of the Symmetric Posterior Condyle total knee arthroplasty components at a single institution. Additional goals were to assess for differences in revision risk between the OxZr and CoCr implants and to evaluate the impact of age, sex and body mass index on revision risk and assess the functional scores in patients in whom the prosthesis has been used.
Methods
The institution’s ethics review board approved the study. All patients received the Genesis II Symmetric Posterior Condyle or Legion Primary total knee implanted at the study centre between March 2007 and December 2013. All implants in the study were cemented and used a posterior stabilized design. Selection of OxZr versus CoCr was left to surgeon preference in discussion with the patient; however, selection of OxZr was restricted to patients aged less than 60 years with expected higher activity levels and a history of metal sensitivity, based on regional guidelines. Preoperatively, patients provided informed consent and were enrolled into a prospective research database. The database documents patient demographic characteristics, diagnosis, procedure details and outcome scores.
All procedures performed by the 4 participating fellowship-trained arthroplasty surgeons were eligible for inclusion in the study. Patients were followed at 6 weeks, 6 months, 1 year, 2 years and every 2 years thereafter for routine monitoring and surveillance. Follow-up data were captured from March 2007 until August 2014. Age at time of surgery, height and weight were documented, and body mass index was calculated. The bearing surface of the femoral component was also documented. In addition, we analyzed the preoperative, 1-year postoperative and 2-year postoperative Oxford Knee Score values (best possible score 12, worst possible score 60). This instrument has proven to be reliable, valid and responsive to clinical change.14–16
Statistical analysis
We performed survival analysis using Kaplan–Meier techniques for the entire population and then separately for the CoCr and OxZr implants. We compared survivorship of the CoCr and OxZr version using the Cox proportional hazards method to control for the possible confounding effects of age,17,18 sex17–19 and body mass index19,20 on revision risk. We compared demographic characteristics and functional score using t tests for continuous data and the χ2 test for dichotomous data.
Results
A total of 2178 patients with 2815 primary total knee replacements were identified in the database. The demographic data can be found in Table 1. The mean age of the patients at the time of surgery was 64.7 (standard deviation [SD] 10.7) years, and the patients were predominantly female (1359 [62.4%]). The average body mass index of all eligible patients from the database was 35.0 (SD 8.5).
Patient demographic and clinical characteristics
There were 2286 CoCr components and 529 OxZr components implanted. Patients who received the OxZr implants were younger than those who received the CoCr implants and were predominantly male (Table 2). There was no difference in body mass index between the 2 implant groups.
Patient demographic characteristics by femoral component material
Survivorship
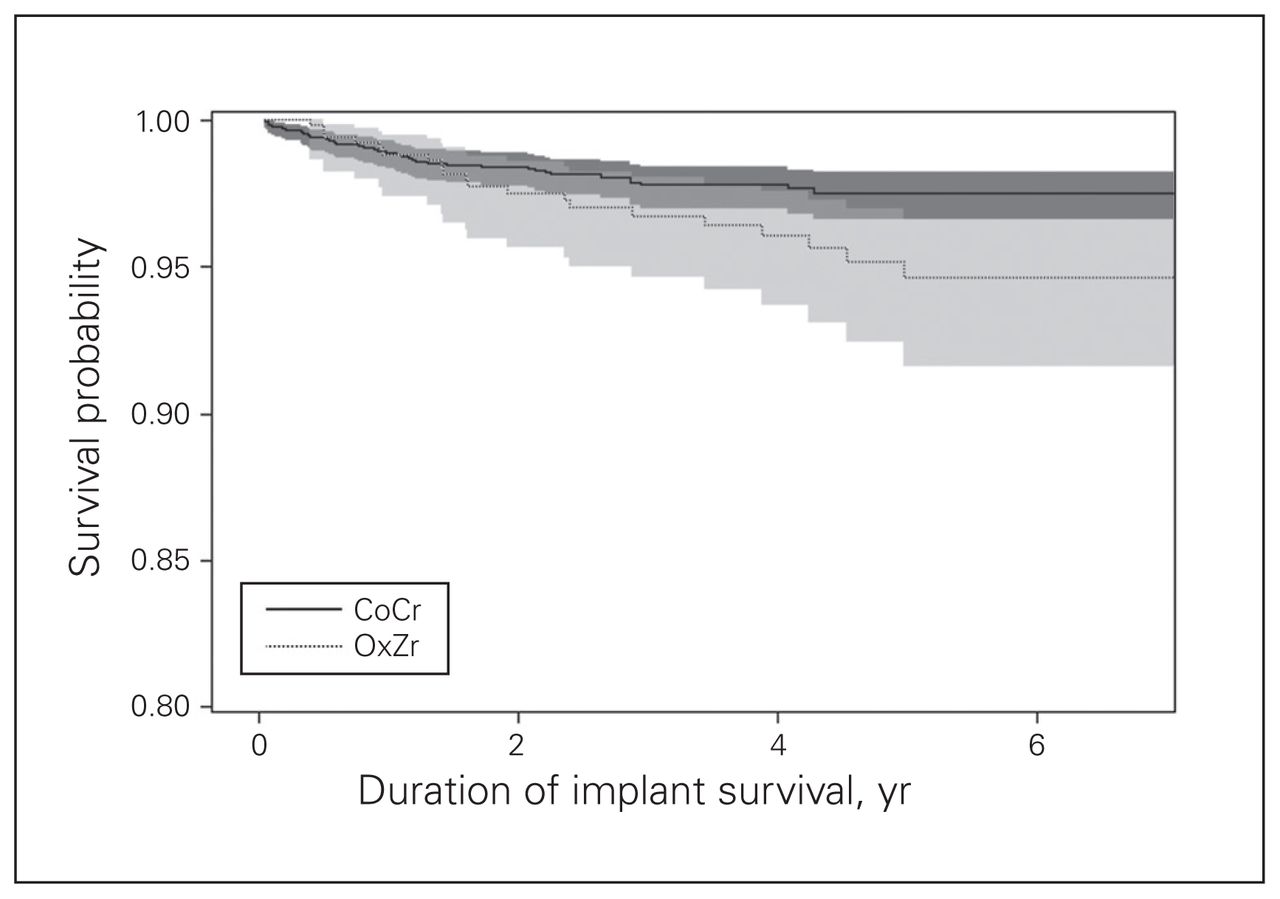
Kaplan–Meier analysis of the pooled implants showed a 2-year survival rate of 98.2% (95% CI 97.6%–98.7%) for failure for any reason and a 5-year survival rate of 96.8% (95% CI 96.0%–97.7%) (Fig. 1). There were 63 cases that required revision, with infection being the most common reason (Table 3). Cox proportional hazards analysis showed that both female sex and increased age lowered revision risk and that there was a trend toward increased revision risk with increased body mass index, but this did not reach statistical significance (Table 4). The individual CoCr and OxZr Kaplan–Meier survival curves are presented in Figure 2. After adjustment for age, sex and body mass index, we could not detect any difference in survival between the 2 materials.

Pooled Kaplan–Meier product-limit survival estimate of the Genesis II Symmetric Posterior Condyle/Legion Primary total knee implant (Smith & Nephew). Grey shading represents 95% confidence intervals.

Kaplan–Meier product-limit survival estimates for cobalt–chromium (CoCr) and oxidized zirconium (OxZr) femoral implants. Grey shading represents 95% confidence intervals.
Reasons for revision
Risk of revision by age, sex, body mass index and femoral implant material
Outcome scores
There were 1851 total knee replacements with preoperative Oxford Knee Score values available for analysis. The mean preoperative score was 40.2 (SD 8.3). The mean score improved to 22.6 (SD 8.6) at 1 year postoperatively and 21.8 (SD 8.9) at 2 years. The improvement in the score at 1 year was statistically significant (95% CI 17.06–18.09), as was the improvement at 2 years (95% CI 17.06–18.09). No differences were found between patients who received OxZr implants and those who received CoCr implants.
Discussion
We found that the overall (combined CoCr and OxZr) revision rate of the Legion Primary knee system was 1.8% at 2 years and 3.2% at 5 years. The Australian National Joint Replacement Registry shows a cumulative revision rate at 3 years of 1.8% for the posterior-stabilized CoCr bearing models and 3.2% for the posterior-stabilized OxZr models.3 Although this may reflect a difference in the performance of these two materials, it may also result from selection bias from the OxZr products’ being used in patients at increased risk for failure, such as those less than age 55. At 5 years, the registry shows cumulative revision rates of 2.1% for CoCr models and 4.1% for OxZr models with posterior-stabilized designs.3 The findings in the current study are consistent with the results from the Australian registry.
Our results also suggest that both age at time of surgery and sex have an influence on overall survivorship. Increased age at time of surgery decreased the revision rate, with a hazard ratio of 0.968, which is in keeping with registry data. Data from the National Joint Registry of England, Wales and Northern Ireland and the Isle of Man demonstrate decreasing cumulative revision rates at each incremental increase in age of 5 years.4 Similarly, the New Zealand Joint Registry illustrates a statistically significant decrease in revision rate with each successive incremental increase in age of 10 years.21 In our series, female sex had a positive influence on implant survivorship. Again, this is in keeping with reports from several national joint registries. 3,4,21 The 2016 report from National Joint Registry of England, Wales and Northern Ireland and the Isle of Man indicates that males are more likely to undergo revision than females of comparable age if they were less than 75 years old at the time of primary surgery.4 Given that the predominant indication for revision in our study was infection, this may be related to the finding of Rasouli and colleagues22 that male sex was associated with an increased risk of surgical site infection, with an odds ratio of 1.79.
Femoral bearing surface did not have a statistically significant influence on overall survivorship of the Legion Primary implant in our series, even when we controlled for the possible confounding effects of age, sex and body mass index. The OxZr implant is a premium implant with an associated increase in cost. The differential varies between centres based on regional contracting; however, the cost of the OxZr femoral component may be as much as 4 times that of the otherwise identical CoCr component. Tribological studies have suggested superior characteristics of OxZr femoral implants in comparison to the standard CoCr femoral implants.7,23–25 Interestingly, these superior characteristics have not resulted in consistent published reports of improvement in in vivo wear or superior clinical results in knee arthroplasty. This is in contrast to total hip arthroplasty, where data from the Australian joint registry suggest superiority of this bearing surface in terms of survival. 3 Matched comparison retrieval studies have shown a decrease in femoral component damage in OxZr components8,26,27 and a corresponding decrease in polyethylene damage.26 Synovial fluid analysis in patients with bilateral total knee replacement failed to show differences in polyethylene particle number, weight, size and shape between the CoCr knee and the OxZr knee,28 and no clinical differences were found between groups.29 A small randomized controlled trial evaluating OxZr and CoCr implants in patients undergoing simultaneous total knee arthroplasty procedures failed to show significant differences in clinical, subjective and radiographic outcomes at 5 years.30 Vertullo and colleagues31 reviewed 17 577 cases from the Australian joint registry involving a cruciate-retaining asymmetric-flexion knee and found no difference in implant survival in patients less than 75 years of age, with poorer survival of OxZr implants at or beyond this age. Our study supports these findings in a posterior-stabilized symmetric flexion knee by the same single manufacturer.
Conclusion
Although there are theoretical advantages to using the OxZr implant bearing surface, we did not detect an improvement in early to midterm implant survivorship. With no apparent survival benefit to the OxZr surface in knees, the use of these more expensive implants may not be warranted to extend implant longevity until longer-term evidence of superiority is presented. The symmetric posterior condylar posterior-stabilized design as a whole offers excellent early to midterm survivorship, with a cumulative revision rate of 1.8% at 2 years and 3.2% at 5 years in the current study. The findings support the continued use of this design iteration, which is based on a previous implant with an excellent record. Both increased age and female sex had a positive influence on implant survivorship; however, we could not detect any effect of body mass index on survivorship.
Acknowledgements
This study was supported by funds granted from the Thorlakson Chair at the Department of Surgery, University of Manitoba.
Footnotes
Competing interests: A.R. Demcoe has no conflicts to declare. E.R. Bohm, D.R. Hedden, C.D. Burnell and T.R. Turgeon all declare institutional research support (unrelated to this project) from DePuy Synthes, Hip Innovation Technology, Smith & Nephew and Zimmer, and institutional fellowship educational funding from DePuy Synthes and Smith & Nephew. E.R. Bohm declares speakers bureau/paid presentations for Zimmer, DePuy Synthes and Stryker and unpaid consultancy for Smith & Nephew. D.R. Hedden declares a paid consultancy for Smith & Nephew. T.R. Turgeon declares speakers bureau/paid presentations for DePuy Synthes and unpaid consultancy for Smith & Nephew.
Contributors: A.R. Demcoe, E.R. Bohm and T.R. Turgeon designed the study. D.R. Hedden and C.D. Burnell acquired the data, which A.R. Demcoe, E.R. Bohm and T.R. Turgeon analyzed. A.R. Demcoe and T.R. Turgeon wrote the article, which all authors reviewed. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
- Accepted July 10, 2018.
References

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.