


Pharyngeal perforation after blunt cervical trauma is a rare occurrence, which can cause serious morbidity and mortality if not diagnosed and treated early. Successful treatment depends on the size and location of the perforation. We found 11 reports of pharyngeal perforation after blunt trauma to the neck published after 1970.1–11 We report here the details of our experience with the 12th case of blunt pharyngeal perforation.
Case report
A 23-year-old man hit his head on the steering wheel when his car hit an electrical pole at a speed of 80 km/h.
On arrival at the Montreal General Hospital, his pulse rate was 90 beats/min, a respiratory rate of 18/min and a blood pressure of 130/70 mm Hg. His airway was intact and his Glasgow Coma Scale score was 15. He had no neurologic deficit, dyspnea or hoarseness. He complained of neck pain, odonyphagia and had evidence of a tender right submandibular hematoma. A lateral cervical spine film showed retropharyngeal emphysema (Fig. 1). The remainder of his history and physical examination was unremarkable.

Lateral cervical x-ray film showing streaks of air in the retropharyngeal region.
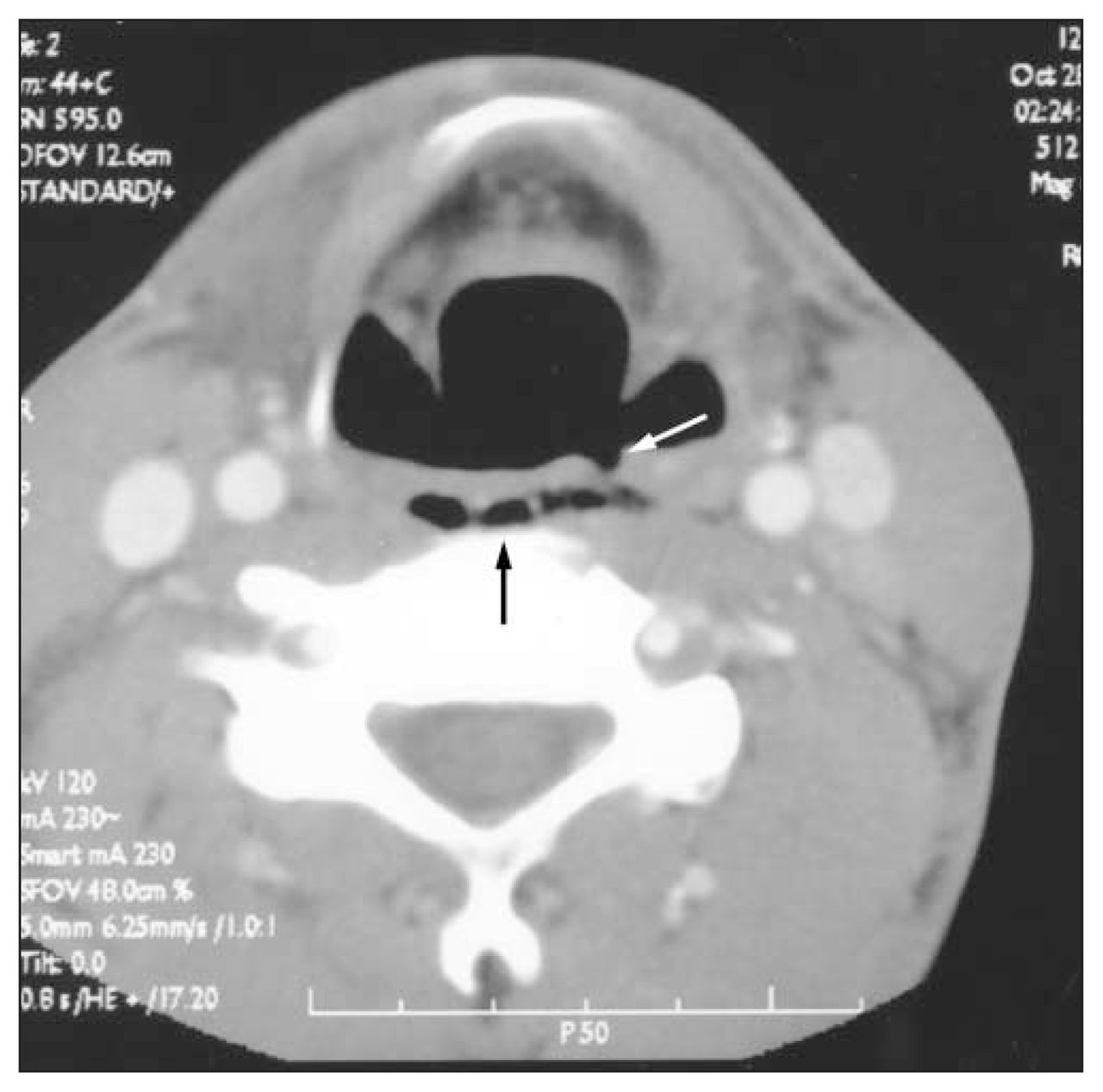
Computed tomography demonstrated retropharyngeal air starting at the level of the epiglottis. There was slight irregularity of the posterior wall of the hypopharynx extending for 2 cm. The site of perforation was clearly indicated (Fig. 2). Flexible esophagoscopy revealed a tear on the left side of the posterior pharyngeal wall at the level of the epiglottis. The esophageal mucosa distally was intact.
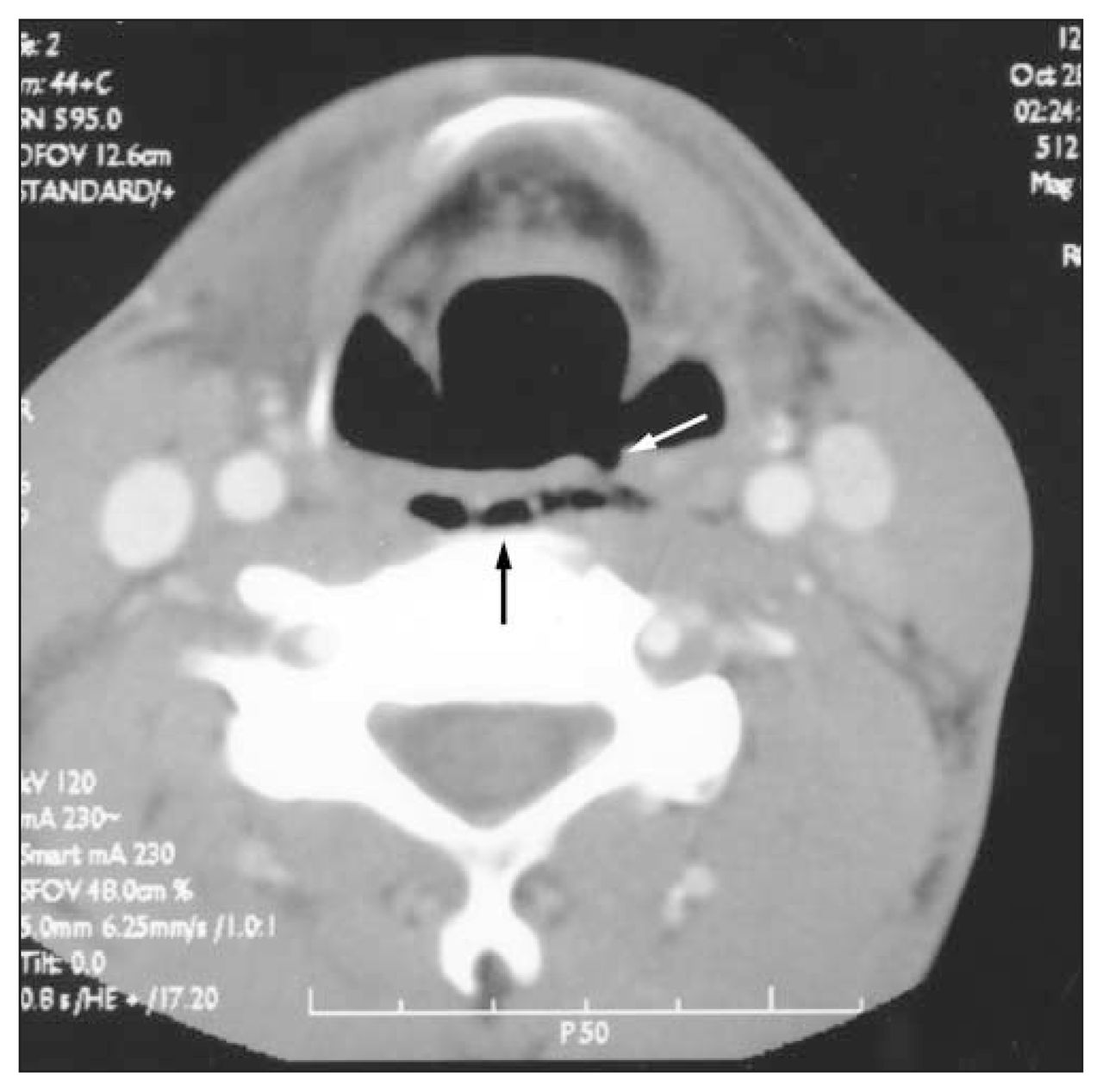
Axial cervical computed tomography scan showing retropharyngeal air (black arrow) and the pharyngeal tear (white arrow).
The patient was admitted to the intensive care unit, where he was kept in the fasting state, and cefazolin 1 g every 6 hours and metronidazole 500 mg every 6 hours were started intravenously. Because he refused insertion of a nasogastric tube, flexible fibroptic nasotracheal intubation was done in the operating room. He was found to have 2-cm posterior pharyngeal wall tear. This was repaired with interrupted 3–0 polydioxanone surgical sutures through a lateral cervical approach. The retropharyngeal space was drained.
The drain was removed on postoperative day 3. He was discharged from the hospital on postoperative day 4 on a soft diet. When seen at follow-up, after 2 weeks and 1 month, he was well with no complaints.
Discussion
The commonest cause of pharyngeal perforation is iatrogenic (i.e., occurring during instrumentation).1–3 It has a more favourable prognosis than perforation caused by blunt trauma to the neck, in which the tear is usually larger or extends to the intrathoracic esophagus. Knowledge of the size and location are critical to the management of this injury. Most authorities believe that primary closure should be performed.3
Since the introduction of seat belts, the frequency of blunt head and neck trauma has decreased. Pharyngeal perforation is rare after blunt trauma to the neck, accounting for less than 2% of all perforations in the pharyngoesophageal region.4 To date, only 11 cases had been reported in the world literature since 1970.1–11
Trauma secondary to endotracheal intubation is an uncommon occurrence and is usually due to a very difficult intubation or to the inexperience of the individual placing the tube, an emergent setting, or the use of a stylet during the procedure.5–8 Moreover, there are reports of injury to neonates in intensive care units attributed to the use of rigid suction catheters, nasogastric and endotracheal tube placement, and digital trauma by the physician during resuscitation.9–11
Niezgoda and colleagues2 reviewed the literature and divided these 11 cases into 2 categories depending on the method of management: either nonoperative or surgical. Nonoperative treatment is reserved for patients with small perforations, less than 2 cm long and limited to the pharynx. Patients are kept fasting and treated with nasogastric suction and broad-spectrum antibiotics. Four of 5 patients treated in this fashion made uncomplicated recoveries. Of the 6 patients requiring operative repair of the injury, all had perforations greater than 2 cm or complex tears involving the esophagus. All but 1 of these 6 patients recovered without complications. The sixth patient, in whom the diagnosis was delayed for longer than 12 hours, required treatment for a paraesophageal abscess.2
Whereas early outcome is reported in the literature, the long-term sequelae of pharyngeal perforation secondary to blunt trauma is unknown because follow-up of these patients is lacking.
In the present case, even though the perforation was limited to the pharynx, we opted for surgical repair because of the size of the tear and the easy accessibility for repair.
In summary, pharyngeal perforation after blunt neck trauma is rare. Early diagnosis requires an awareness of this condition in any patient who complains of severe neck pain, odynophagia, dyspnea, stridor or hoarseness or who is found to have neck crepitus or subcutaneous emphysema after blunt neck trauma. Treatment must be individualized according to the size and location of the tear and the experience of the treating team.
- Accepted September 2002.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.