


Venous aneurysms are extremely rare, and most are incidental findings that have no major clinical significance. Popliteal venous aneurysms are an exception to this rule. Their presence is strongly associated with recurrent pulmonary embolism. To the best of our knowledge a popliteal venous aneurysm has never been reported as a cause of iliofemoral deep venous thrombosis. We report a case of iliac vein stenosis, which we hypothesize prevented the passage of an embolism from a popliteal venous aneurysm to the pulmonary circulation.
Case report
A 42-year-old woman presented to a rural hospital complaining of acute swelling of the left lower extremity starting the previous day. Ultrasonography revealed decreased flow velocities in the deep veins of the left lower extremity. A diagnosis of a presumed deep venous thrombosis was made, and the patient was discharged home on a therapeutic dose of low-molecular-weight heparin.
She returned to hospital 2 days later with worsening of the lower extremity swelling and cyanosis of her left foot.
Upon transfer to our institution, the patient denied any risk factors for deep venous thrombosis. Her medical history was unremarkable. She was on no medications, including oral contraceptives, and had no drug allergies.
A therapeutic dosage of unfractionated heparin was started, and CT of the lower extremity with venous delay was performed. CT revealed thrombus occluding the left common, external and internal iliac veins as well as the common and superficial femoral veins. In addition, a saccular venous aneurysm measuring 3.7 cm × 3.4 cm was present in the popliteal vein just above the knee. This aneurysm contained a nonoccluding clot (Fig. 1A).
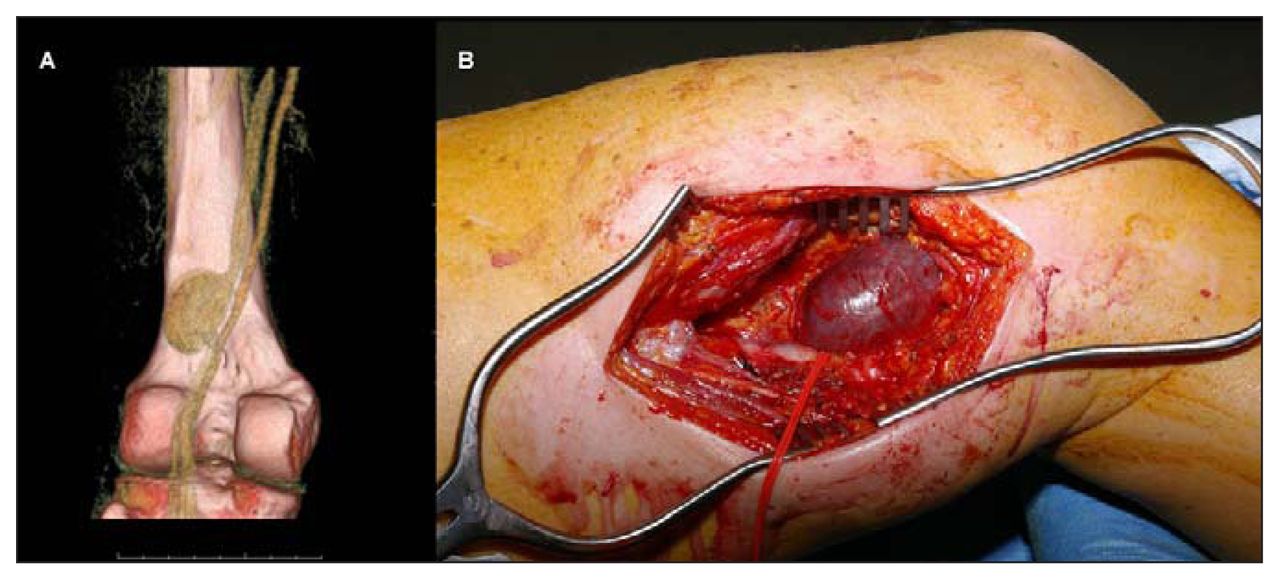
Politeal venous aneurysm located off the proximal aspect of the left popliteal vein. A: Volume-rendered image from a venous-phase CT scan. B: Intraoperative view shows the saccular venous aneurysm just above the knee.
After in-depth discussion with the patient and her family regarding the risks and benefits of conservative versus operative management, the patient consented to undergo operative resection of the venous aneurysm.
Under general anesthesia the popliteal fossa was explored, revealing a large saccular aneurysm off the popliteal artery just above the knee (Fig. 1B). A tangential aneurysmectomy with lateral venorrhaphy was performed. Open thrombectomy of the femoral and iliac veins was then performed through the left groin under fluoroscopic guidance. Completion venography revealed the unexpected finding of common iliac vein stenosis at the proximal end of the thrombus (Fig. 2), which was treated by angioplasty. Finally, a left femoral–femoral arteriovenous fistula was fashioned in an attempt to maintain venous patency.

Intraoperative venogram showing the site of stenosis of the left iliac vein (arrow).
The patient was maintained on unfractionated heparin throughout the procedure and postoperatively. Her postoperative course was uncomplicated, and she was discharged home on postoperative day 3 on low-molecular-weight heparin. Our plans were for her to remain on long-term oral anticoagulation and to return in the future for closure of the fistula.
Discussion
Compared with the arterial circulation, aneurysms of the venous system are rare.1 As of 2000, there were 117 reported cases of venous aneurysms in the world literature, 45% of which were associated with pulmonary embolism.2 These aneurysms are usually asymptomatic or present as soft masses that become more prominent when in a dependent position. However, popliteal venous aneurysms, which are extremely rare, seem to be an exception to this rule. They are associated with a significant incidence of recurrent pulmonary embolism, often despite adequate anticoagulation.3 Although the thromboembolic complications of popliteal venous aneurysms have been well described, iliofemoral thrombosis has not been reported in association with popliteal venous aneurysms.
First reported in 1957 by May and Thurner,4 compression of the left iliac vein by the overlying right iliac artery is now a well-documented cause of partial venous obstruction.
In our case, the patient had an iliac vein stenosis. Although considered to be a cause of iliofemoral thrombosis, iliac vein stenoses can also represent incidental, asymptomatic findings.5
We hypothesize that in our case the popliteal venous aneurysm was the source of a venovenous embolization. The iliac stenosis was protective, acting as a filter, which prevented the clot from progressing upstream and reaching the pulmonary circulation.
Footnotes
Competing interests: None declared.
- Accepted November 8, 2006.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.