


Abstract
Background: It is generally accepted that surgical training is associated with increased surgical duration. The purpose of this study was to determine the magnitude of this increase for common surgical procedures by comparing surgery duration in teaching and nonteaching hospitals.
Methods: This retrospective population-based cohort study included all adult residents of Ontario, Canada, who underwent 1 of 14 surgical procedures between 2002 and 2012. We used several linked administrative databases to identify the study cohort in addition to patient-, surgeon- and procedure-related variables. We determined surgery duration using anesthesiology billing records. Negative binomial regression was used to model the association between teaching versus nonteaching hospital status and surgery duration.
Results: Of the 713 573 surgical cases included in this study, 20.8% were performed in a teaching hospital. For each procedure, the mean surgery duration was significantly longer for teaching hospitals, with differences ranging from 5 to 62 minutes across individual procedures in unadjusted analyses (all p < 0.001). In regression analysis, procedures performed in teaching hospitals were associated with an overall 22% (95% confidence interval 20%–24%) increase in surgery duration, adjusting for patient-, surgeon- and procedure-related variables as well as the clustering of patients within surgeons and hospitals.
Conclusion: Our results show that a wide range of surgical procedures require significantly more time to perform in teaching than nonteaching hospitals. Given the magnitude of this difference, the impact of surgical training on health care costs and clinical outcomes should be a priority for future studies.
Training the next generation of surgeons is an integral part of a sustainable health care system. Surgical training is associated with decreased operative efficiency owing to the time required for instruction in addition to the slower operative speed of trainees compared with senior surgeons.1–8 Given the long duration of surgical residency, surgical training can result in substantial cumulative inefficiency, which impacts cost as well as access to limited surgical resources. Previous research has also demonstrated a consistent association between prolonged surgery duration and adverse patient outcomes across a wide range of procedures.9–20
Although previous research has shown that trainee involvement is associated with prolonged surgical duration,1–8 the magnitude of this increase has not been estimated at a population level, nor has previous research adjusted for patient- and surgeon-related factors, such as experience of the attending surgeon. Administrative data from the province of Ontario are ideal to address this research question because surgical training in Ontario is concentrated within a limited number of teaching hospitals, such that the impact of training on surgery duration can be estimated by comparing teaching and nonteaching hospitals.
The objective of this study was to establish robust, population-based estimates of the time premium associated with operative training for a variety of common surgical procedures, adjusting for patient-, surgeon- and procedure-related variables. Results from this study can be used by administrators, policy-makers and legislators to make informed decisions about sustainable funding for surgical education and will provide a benchmark for surgical educators as they balance operative efficiency and trainee participation with the potential for adverse time-dependent surgical outcomes.
Methods
Study setting and design
Residents of the province of Ontario, Canada, (population 13.4 million in 2012)21 have universal access to hospital care and physician services. Private delivery of such services is prohibited, meaning that all eligible procedures performed in the province are recorded in administrative databases. Relevant data sets were linked using unique, encoded identifiers and analyzed at ICES Western, a satellite site for the Institute for Clinical Evaluative Sciences (ICES) in Toronto, Ont.
In Ontario, surgical and anesthesiology training is concentrated in hospitals associated with 6 medical schools. Nonteaching services in teaching hospitals are rare, and in most programs residents outnumber staff, meaning that it is reasonable to assume that a resident will be present at almost all procedures performed in a teaching hospital. Residents rotate through community hospitals for a small proportion of their overall training. When present in a community hospital, residents would typically replace a surgical assistant.
In this retrospective, multicentre, population-based cohort study, all adult residents of Ontario who underwent any of the index procedures (see the section on procedures and data sources) between Apr. 1, 2002, and Mar. 31, 2012, were included. Cases were excluded if the patient was younger than 18 years, if the procedure was performed emergently or during out-of-office hours (evening, weekend, or holiday; not for appendectomy or hip fracture), if the surgery was for a recurrent condition, if the attending surgeons’ main specialty was atypical for the procedure, or if the surgery was performed without an anesthesiologist (involvement of anesthesiology was required to calculate the outcome). Elective procedures (except tonsillectomy, which is rarely performed with an assistant) performed in nonteaching hospitals were excluded if an assistant did not submit a valid payment claim for the surgery because it was thought that such surgeries may be more likely to include resident assistants. Finally, 2 geographic areas encompassing less than 1.5% of the Ontario population were excluded owing to concerns regarding procedure coding accuracy in those areas. The number of cases excluded at each step is presented in Appendix 1, Table S1 (available at canjsurg.ca).
Procedures and data sources
A panel of experts selected procedures from various surgical specialties that represent common procedures that are often managed in both teaching and community settings, but rarely require referral to tertiary care centres. Procedures included laparoscopic cholecystectomy, right hemicolectomy, appendectomy, unilateral inguinal hernia repair, hysterectomy, hip hemiarthroplasty, open reduction and internal fixation (ORIF) for hip fracture, hip and knee arthroplasty, and tonsillectomy (see Appendix 1, Table S2 for coding information); where applicable, open and laparoscopic procedures were considered separately.
Surgeon and patient characteristics were ascertained from 5 linked health care administrative databases: the Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD) and Same Day Surgery (SDS) databases (includes diagnostic, procedural and clinical patient data), the Ontario Health Insurance Plan (OHIP) database (contains health claims), the Registered Persons Database (vital statistics for all residents of Ontario) and the ICES Physician Database (information for all physicians practising in Ontario).
We created exposure groups based on the type of hospital (teaching v. nonteaching) in which the index procedure was performed. Hospital type was determined using a list of academic hospitals published by Health Force Ontario,22 all of which have surgical training programs. The number of hospitals in each group fluctuated slightly over time owing to openings, closures and mergers. In the final year (2012) we identified 19 teaching hospitals and 159 nonteaching hospitals. Although 1 medical school (Northern Ontario School of Medicine) began providing postgraduate training during the study period, the 2 hospitals associated with this program were classified as nonteaching because of the very small number of residents enrolled during the timeframe of this study. The impact of this decision should be minimized by the exclusion of procedures performed at nonteaching hospitals without an assistant. There are no known surgical training programs at any other nonteaching hospitals included in the study.
Variable definitions
Duration of surgery was determined on the basis of anesthesiology billing records, using the methodology validated by Redelmeier and colleagues.23 In Ontario, anesthesiologists submit fee-for-service billings through OHIP, with fees calculated according to a standardized algorithm based on service units. Service units related to surgery duration represent the entire time that the anesthesiologist is in attendance with the patient and are recorded in 15-minute intervals; therefore, times calculated based on these units should include all physician teaching activities that occur during the encounter.
We determined patient complexity using the Johns Hopkins ACG (adjusted clinical group; ACG software version 10) methodology.24 This method of case-mix grouping captures all morbidities for which a patient receives care during a defined period — in this case, 3 years before the procedure date. The ACGs can be collapsed into 6 resource utilization bands (RUBs) on the basis of expected use of health care resources. In the present study, we used the CIHI-DAD, CIHI-SDS, CIHI–National Ambulatory Care Reporting System (NACRS) and OHIP databases to calculate RUBs, which were summarized as a 3-point ordinal variable: 1 = low (RUB = 0–3), 2 = moderate (RUB = 4) and 3 = high (RUB = 5).
Statistical analysis
We conducted all analyses using SAS software version 9.3 (SAS Institute). Differences in baseline variables between teaching and nonteaching hospitals were assessed using standardized differences, with an effect size threshold of > 0.2 used to identify meaningful differences. We assessed differences in mean surgery duration using t tests. As surgery duration is a non-negative integer, it is appropriate to model it using a count data model, such as Poisson or negative binomial regression. In this case, where overdispersion was present, we used negative binomial regression to assess the association between surgery duration and teaching hospital status, controlling for patient age, sex, obesity (body mass index [BMI] > 40), complexity (RUB), anesthetic technique, procedure year and procedure type (only for analyses involving multiple procedures). We additionally controlled for surgeon-related variables, including age, sex and annual procedure-specific volume (determined using the OHIP database). To account for the clustering effect of patients within surgeons and hospitals, we used the generalized estimating equations approach.
We conducted 3 additional sensitivity analyses to assess the presence of referral bias, whereby more difficult, potentially longer-duration cases are referred to teaching hospitals. Two of these analyses used the Ontario Multispecialty Network (OMN) database25 to identify each patient’s expected admitting hospital. The OMN assigns Ontario residents to an expected admitting hospital using a 2-step process: individuals are linked to a “usual provider of care,” and providers are linked to hospitals. The OMN also aggregates select hospitals into hospital networks, such that the expected place of admission can be 1 of several individual hospitals within the network (i.e., the patient’s expected admitting hospital network). In the first sensitivity analysis, the cohort was limited to procedures performed at the patient’s expected admitting hospital, whereas the second was limited to procedures performed within the patient’s expected admitting hospital network. In the final sensitivity analysis, the cohort was limited to patients defined as having a low level of complexity (RUB = 1). All 3 sensitivity analyses involved the same statistical approach used for the primary analyses.
Results
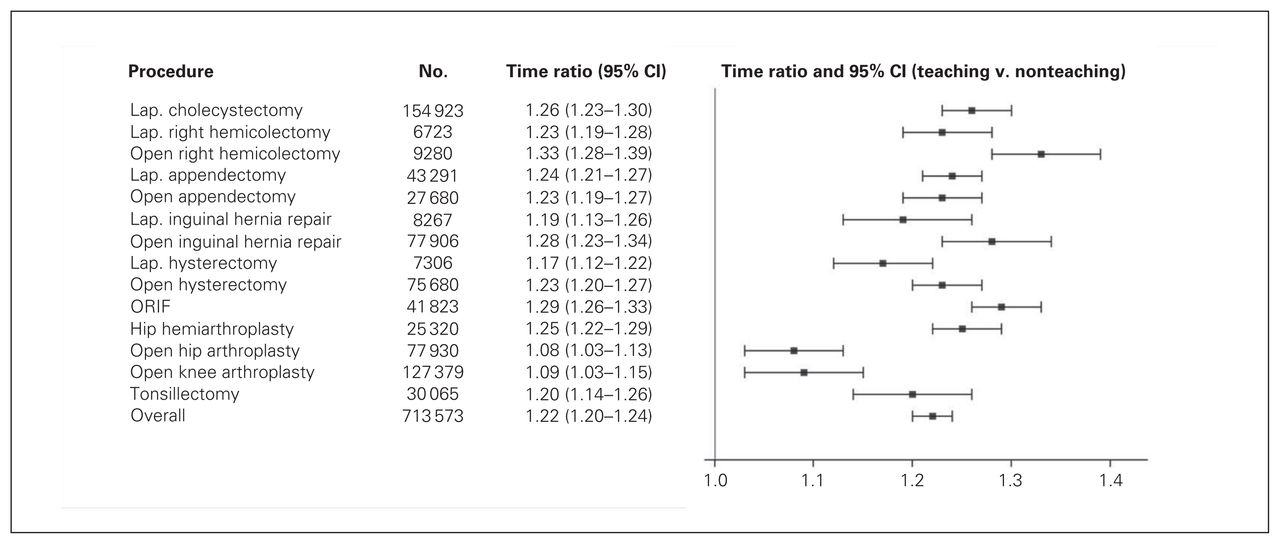
Of the 713 573 surgical procedures included in this study, 148 538 (20.8%) were performed in a teaching hospital, representing 11.7%–39.8% across the individual procedures. Across all procedures, the mean duration of surgery was significantly longer for procedures performed in teaching than nonteaching hospitals, with mean differences ranging from 5 to 62 minutes across the individual procedures and all comparisons significant at p < 0.001 (Table 1). In negative binominal regression analyses adjusting for patient-, surgeon- and procedure-related variables, teaching hospitals were associated with significantly longer surgery durations than nonteaching hospitals for all of the procedures studied (Fig. 1). Across the 14 procedures, teaching hospitals were associated with an overall 22% (95% confidence interval [CI] 20%–24%) increase in surgery duration, ranging from 8% for hip arthroplasty to 33% for open right colectomy.

Operative time ratio comparing surgery duration in teaching and nonteaching hospitals, adjusted for patient-, surgeon- and procedure-related variables (see the Statistical analysis section for a complete description of covariate adjustment). CI = confidence interval; Lap = laparoscopic; ORIF = open reduction and internal fixation.
Mean duration of surgery by hospital type and unadjusted difference in surgery duration comparing teaching to nonteaching hospitals (in minutes)
Patients treated in teaching and nonteaching hospitals were similar in regards to baseline characteristics (Appendix 1, Table S3a–c). While a slightly higher proportion of complex patients (as ascertained by the RUBs) were treated in teaching hospitals than nonteaching hospitals (26.0% v. 21.5%), most of the baseline differences identified were not clinically significant. Similarly, surgeons operating in teaching and nonteaching hospitals did not meaningfully differ, with the exception that surgeons operating in teaching hospitals tended to perform a greater number of the index procedures per year (mean total of 51.8 ± 43.6 v. 43.3 ± 41.3 procedures).
An increase in surgical duration was evident over the study period in both teaching and nonteaching hospitals for all procedures except elective hip and knee arthroplasty. Overall mean duration increased from 114 minutes in 2002 to 125 minutes in 2011 across the 14 procedures. Post hoc analysis of this unexpected finding suggests that this increase is largely explained by the transition from open to laparoscopic techniques over the study period for several of the included procedures (data not shown).
We conducted 3 sensitivity analyses to investigate the potential impact of referral bias using the same analytic methods used for the main analysis and adjusting for the same covariates. Exclusion of patients who were not admitted to their expected hospital and/or hospital network (on the basis of OMA hospital assignment) did not change our findings, with teaching hospitals remaining significantly associated with increased duration for each procedure type. Again, we obtained similar findings when the cohort was restricted to patients with a low level of complexity. Results for the sensitivity analyses are presented in Appendix 1, Figs. S1–S3.
Discussion
This robust analysis of more than 700 000 cases demonstrates that surgery duration is prolonged in teaching compared with nonteaching hospitals over a wide range of commonly performed procedures. On average, procedures performed in teaching hospitals take 22% longer to complete, with an even greater increase for more complex procedures. The magnitude of this difference suggests a negative impact on both patient outcomes and clinical efficiency. There are many differences between teaching and nonteaching hospitals, with teaching hospitals tending to have larger volume, higher acuity and a greater focus on research. Beyond the impact of these disparities, we propose that factors associated with surgical training likely account for the vast majority of the observed increase in surgery duration.
Prolonged surgery duration has been linked previously to surgical training,1–8 yet few studies have controlled for patient or surgeon factors. Our study confirms these findings by accounting for a wide range of patient and surgeon factors and by generating a robust estimate of the time premium associated with surgical training. This study also differs from previous literature in that we looked at total duration of surgery, defined as the duration of involvement by anesthesiologists, rather than the time from incision to skin closure. Our definition includes all aspects of the operative intervention, including positioning, prepping, draping and insertion of monitoring catheters and lines within the operating suite. Moreover, this definition accounts for all teaching activities that occur within the operating suite, including training of surgical and anesthesiology residents. This metric is potentially more useful from the perspective of both patients and policy-makers, as it encompasses the entire case and all associated resources.
The difference in surgery duration between teaching and nonteaching hospitals was much lower for elective hip and knee arthroplasty than for other procedures, with increases of 8% and 9% in adjusted analyses, respectively. We speculate that specialization within dedicated arthroplasty teams may partly explain this finding. Within Ontario teaching centres, arthroplasty procedures are predominantly performed by surgeons who specialize in arthroplasty and work with dedicated teams, whereas community-based arthroplasty is typically performed by general orthopedic surgeons in nondedicated units. This contrasts with the other procedures we studied, which are often performed by generalists and, although common, rarely dominate a surgeon’s practice in either teaching or nonteaching settings. Whether such efficiencies can be achieved by adopting specialized units for other common procedures is an obvious question posed by this research.
Although investigation of surgical outcomes was beyond the scope of the present study, previous research has demonstrated a consistent association between surgery duration and adverse surgical outcomes.9–20 This association likely reflects multiple confounding factors, including the observation that complex and challenging cases take longer and are associated with higher complication rates. Disentangling the impact of teaching time from other factors that increase surgical duration will be a considerable challenge for future research to address. Quantifying the added operative time that is an inherent component of surgical training represents an important contribution to the debate regarding the effect of trainees on patient outcomes. Future research should aim to identify thresholds that are indicative of excess risk of complications across various surgical procedures.
Limitations
As a large, population-based study, the present study allows for precise estimates and wide generalizability. However, because this study was limited to the data available within administrative databases, it was not possible to adjust for some of the variables known to contribute to surgery duration, such as procedure complexity (e.g., size of hernia). Similarly, no information was available regarding the resident’s experience level or extent of participation, nor was it possible to confirm resident involvement in individual cases. Although this study encompassed the entire training period of several annual cohorts of residents, we were also unable to assess the impact of trainee seniority. Another potential weakness is that we estimated surgery duration on the basis of billing data rather than direct measurement; however, it is unlikely that any bias introduced using this method would have a differential impact on estimates for teaching and nonteaching hospitals.
Conclusion
This population-based study of more than 700 000 cases suggests that trainee involvement significantly increases surgery duration. The magnitude of this increase is large enough to potentially affect direct and indirect costs, institution and surgeon efficiency, and possibly impact surgical outcomes. Our findings with respect to arthroplasty further suggest that the impact of teaching may be reduced when surgical training is delivered in the context of procedure-specific teams. These data provide a benchmark for surgical educators as they strive to meet the needs of their trainees without compromising efficiency or safety. Finally, our study provides robust population-level data allowing policy-makers to include the time costs of surgical training into funding models.
Acknowledgements
The authors thank Drs. Amit Garg, David Urbach and Salimah Shariff for their support and input throughout the study process and Kathryn Barber for providing input regarding hospital coding procedures. This study was funded in part by the Academic Medical Organization of Southwestern Ontario (AMOSO) AHSC AFP Innovation Fund and the London Health Sciences Centre Department of Surgery. This study was supported by the ICES Western site. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Core funding for ICES Western is provided by AMOSO, the Schulich School of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES, AMOSO, SSMD, LHRI, or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions, opinions and statements expressed herein are those of the author, and not necessarily those of CIHI.
Footnotes
Submitted on behalf of the Surgical Investigators Group at ICES Western: Sumit Dave, Eric Frechette, Sarah Jones, Sarah Knowles, Danielle MacNeil, Dave Nagpal, Stephen E. Pautler, Kelly Vogt.
Competing interests: None declared.
Contributors: All authors designed the study and interpreted the results. J. Winick-Ng was responsible for data extraction and analysis. C. Vinden wrote the article, which all authors reviewed and approved for publication.
- Accepted December 23, 2015.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.