


Bullous disease of the lung and pneumothorax are both frequent conditions in thoracic surgery.1 Lung cancer may develop in patients with bullous emphysema,1,2 lung cysts3 and pneumothorax,4 which are usually treated as benign diseases; however, pulmonary carcinoma associated with bullous emphysema is unusual. We report the case of a patient who presented with right spontaneous pneumothorax that was managed surgically through tube thoracostomy followed by minithoracotomy and excision of a right apical bulla. Pathological examination revealed a poorly differentiated non–small cell lung carcinoma (NSCLC), and the patient underwent a right upper lobectomy as final treatment.
Case report
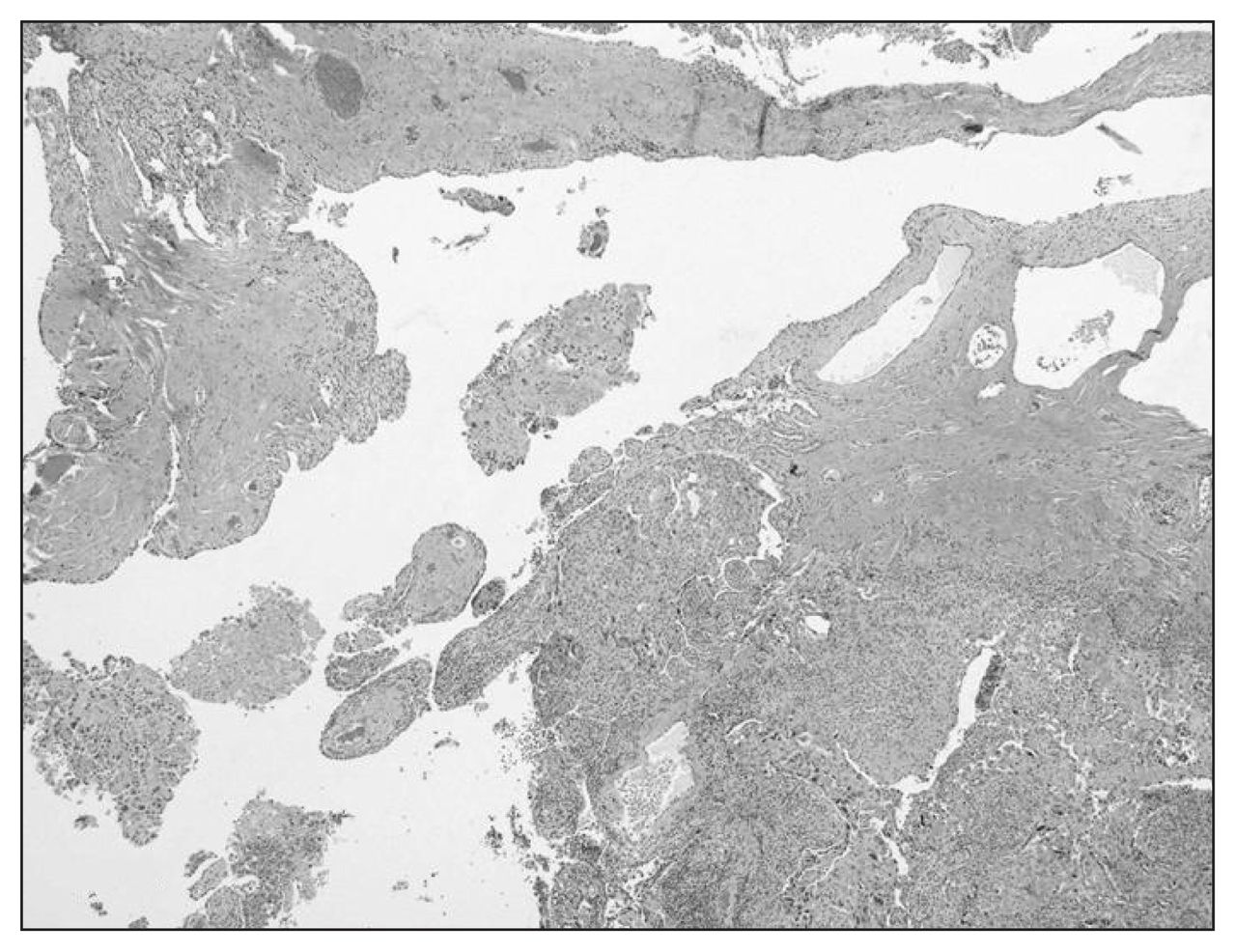
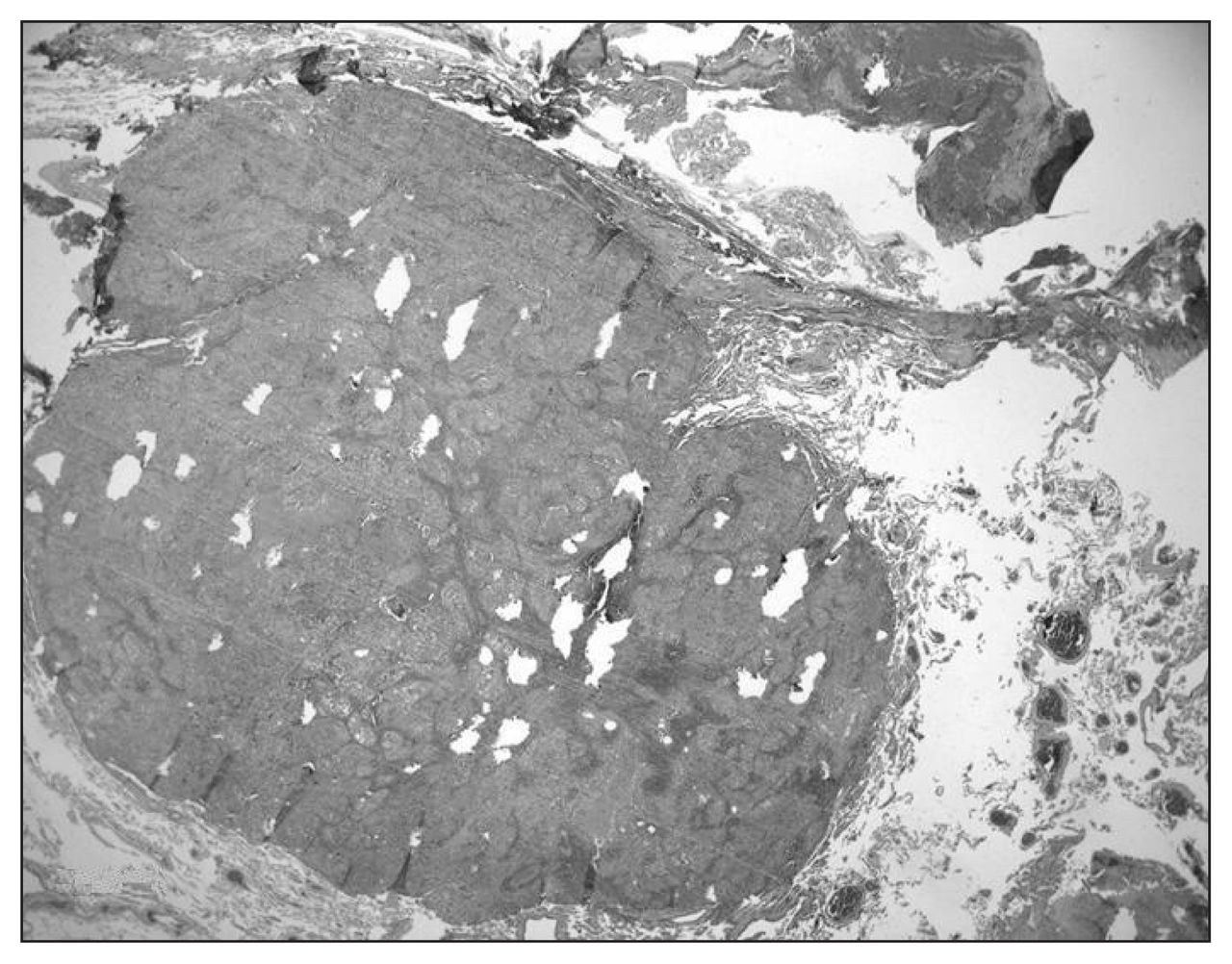
A 52-year-old male smoker presented with a right spontaneous pneumothorax where a chest tube was inserted. Chest radiographs and computed tomography scans showed a right apical lung emphysematous bulla. We planned a thoracoscopic resection. There were adhesions between the emphysematous bulla and the superior vena cava, so we completed the resection through a right minithoracotomy. Pathological examination revealed a large emphysematous bulla with a 0.5-cm poorly differentiated NSCLC focally lining the enlarged airspaces and extending to the surgical margin (Fig. 1). The patient underwent reinvestigation on CT and positron emission tomography; we found no residual lesion. We confirmed a diagnosis of poorly differentiated NSCLC after reviewing the pathology slides, and the patient underwent a right upper lobectomy. Gross examination revealed a small irregular nodule, 12 mm in size, adjacent to the previous resection line (Fig. 2). Microscopy showed a large-cell carcinoma. We detected no metastatic lymph nodes. The patient’s postoperative course was uneventful.
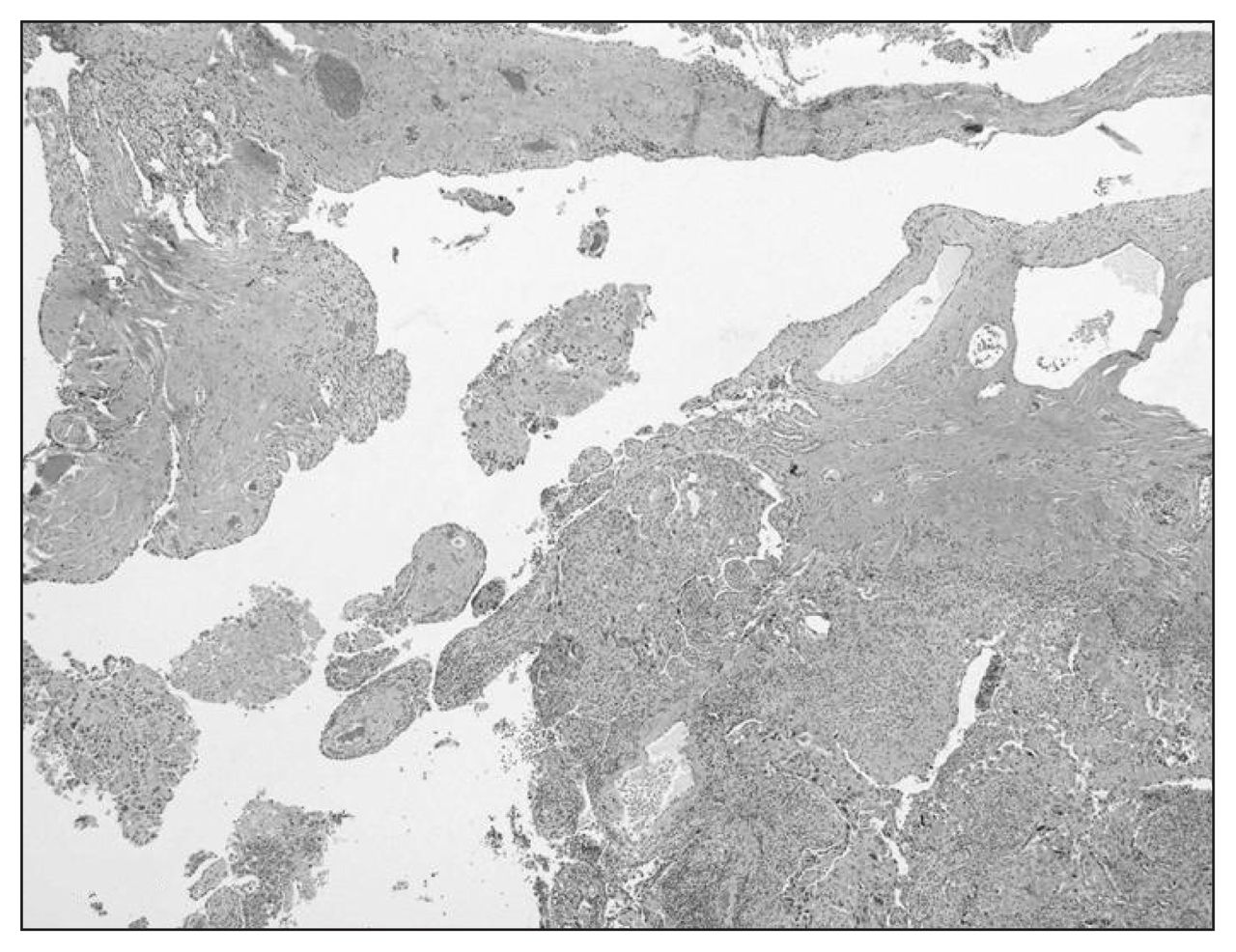
Histology shows the tumour nodule in the bottom right and the enlarged emphysematous subpleural spaces with fibrous septa (hematoxylin and eosin staining, original magnification ×12.5).
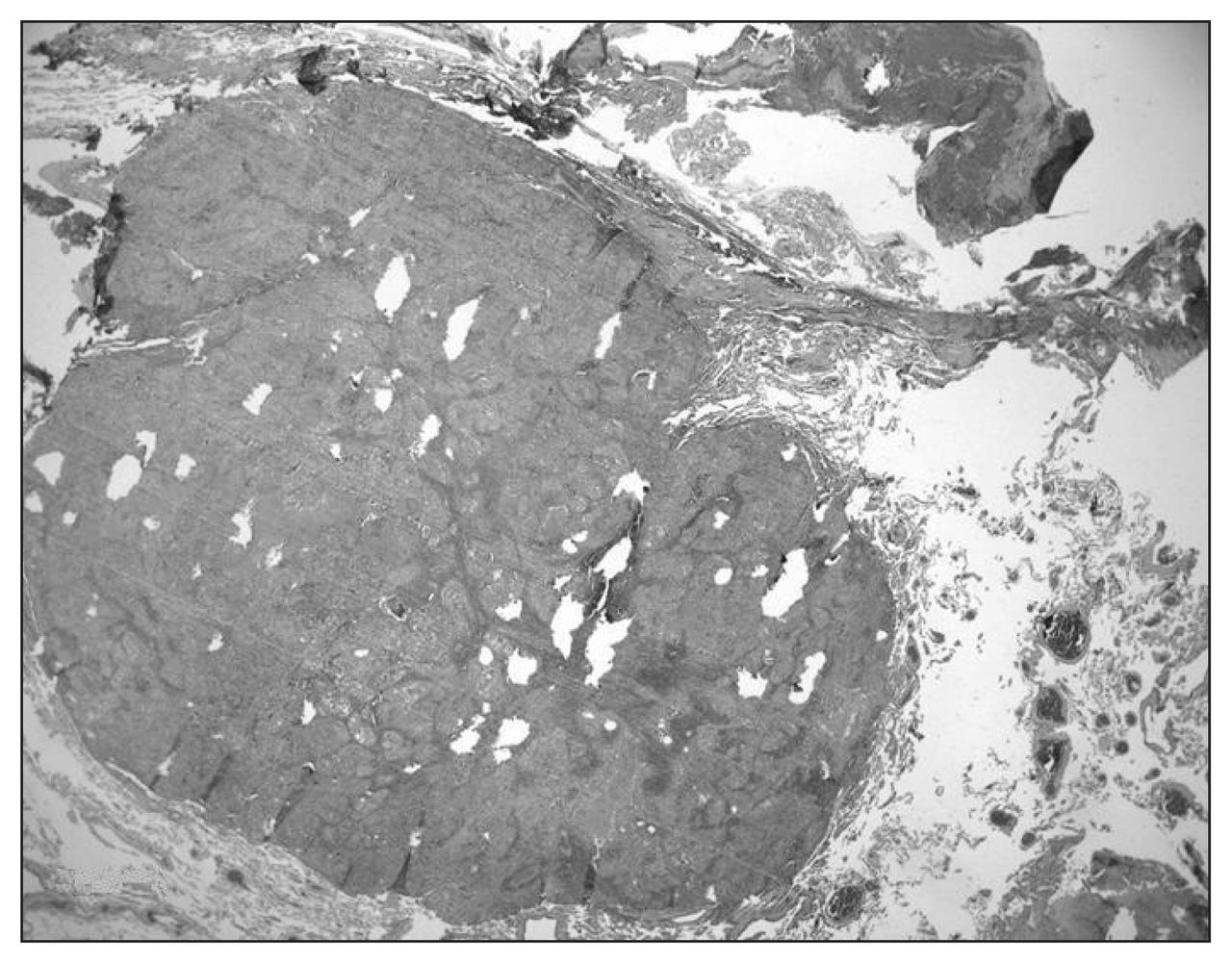
Histology shows the tumour nodule in the vicinity of the emphysematous lung and the surgical margin on the right side. Note a small satellite nodule in the lower right corner (hematoxylin and eosin staining, original magnification ×12.5).
Discussion
Cases of carcinoma arising in bullous lung disease have been reported in the last few years.2 The association of lung cancer with emphysematous bulla is infrequent, and most of these cancers were found to be NSCLCs. Radiological diagnosis of these tumours may be difficult owing to architectural remodelling and scar formation adjacent to the bulla. Hence, most of these tumours were detected on pathological examination, as in our patient’s case.1
Bronchogenic carcinomas, mostly squamous-cell carcinomas, may cavitate, leaving only a thin rim of tumour tissue, and present themselves as a pneumothorax due to the rupture of the carcinomatous bulla.5 In our patient’s case, the bullous dilatation of the airspaces was emphysematous in nature, and there was only a small nodule of carcinoma at the suture line.
We attributed the occurrence of incidental carcinoma in bullous emphysema in our patient to his cigarette smoking, a common etiologic factor of both diseases.2,5
Physicians should be aware of the potential development of lung cancer in patients with pulmonary bullae, even in asymptomatic patients. These patients may present with pneumothorax or lung cysts, and radiologic examination may not be able to detect these cancers. As a result, we recommend careful pathological examination of the specimen. Patients with incidental carcinomas in emphysematous bulla should benefit from pulmonary lobectomy, the standard care for lung carcinoma.
Footnotes
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.