


Abstract
Background: The Advanced Trauma Operative Management (ATOM) course was first introduced into Canada in 2003 at the University of Toronto, with senior general surgery residents being the primary focus. We present an assessment of the course in this Canadian general surgery residency program.
Methods: We compared trainees’ pre- and postcourse self-efficacy scores and multiple choice question (MCQ) examination results, using paired t tests and resident (n = 24) and faculty (n = 7) course ratings made according to a 10-item, 5-point Likert scale. Faculty were previously trained as ATOM instructors.
Results: Mean pre- and postcourse self-efficacy scores were 68.9 (standard deviation [SD] 24.0) and 101.4 (SD 14.8), respectively (p < 0.001). Mean pre- and post-MCQ scores were 16.4 (SD 3.2) and 18.8 (SD 2.7), respectively (p = 0.006). On the Likert scale (1 = strongly disagree, 5 = strongly agree), all faculty and residents rated the following items as 4–5: objectives were met; knowledge, skills, clinical training, judgment and confidence improved; the live animal is a useful representation of clinical trauma; and the course should be continued but would be more appropriate for the fourth rather than the fifth year of residency. Residents rated as 1–2 the item that the human cadaver would be preferable for learning the surgical skills. Of 24 residents, 20 rated as 3 or less the item stating that the course prepares them for trauma management more adequately than their regular training program.
Conclusion: Self-efficacy, trauma knowledge and skills improved significantly with ATOM training. Preference was expressed for the live animal versus cadaver model, for ATOM training in the fourth rather than fifth year of residency and for the view that it complements general surgery trauma training. The data suggest that including ATOM training in Canadian general surgical residency should be considered.
Present trends in the management of torso trauma have resulted in decreasing opportunities for surgical trainees to gain operative experience. 1–4 Factors responsible for this include technological developments that have improved diagnostic accuracy; the ability to stabilize patients, enabling investigations before operative intervention; and studies showing positive outcomes after nonoperative approaches to intra-abdominal injuries. 1 Surgical educators have approached this challenge by focusing on the development of surgical skills centres that use mechanical and live models.5–9 However, many of these approaches lack the realism of an intact, live, bleeding model. Programs such as the Definitive Surgical Trauma Care (DSTC) course introduced in 1996 in Sydney, Australia, as well as the Advanced Trauma Operative Management (ATOM) course developed at the University of Connecticut in Hartford, seek to fill this void by allowing trainees the opportunities to practise operative repair in conditions mimicking the real human situation.10 This report describes the experience with the ATOM course in a Canadian general surgical residency.
The course consists of a precourse preparation package that includes a CD-ROM outlining objectives and demonstrating surgical repair. Participants review exposures dealing with penetrating injuries, with commentary by experts in the field of penetrating trauma management. In addition, participants complete a precourse multiple choice question (MCQ) examination and a self-efficacy test. As well, they are provided with a manual outlining the injuries and a critique of injury approaches with appropriate references, together with a textbook on managing specific injuries derived from writings by experts in the field of trauma. This textbook describes clinical trauma scenarios with the experts’ preferred surgical techniques for managing these injuries, complete with full illustrations.11 On the day of the course, the sessions begin with 6 lectures on the program’s development; trauma laporotomy; liver injuries; injuries to the stomach, duodenum and pancreas; splenic injuries; genitourinary trauma; and cardiac and vascular injuries.
After the lecture sessions, the participants gown and glove and are introduced into an operating room that is fully equipped as a general trauma operating room with full anesthesia, monitoring, nurse assistant and instruments, including the retractors, staples, sutures and so forth that are common in the management of critically injured patients. Standardized injuries created by trained instructors in a porcine model (weight 50 kg) constitute the operating room model where a single participant is taught, evaluated and monitored by a single trained ATOM instructor who is a surgeon knowledgeable in the management of penetrating injuries. The individual participants are introduced into the operating room after being given clinical scenarios and are then tested according to standardized criteria for their ability to identify the injury, develop a correct treatment plan and perform the necessary repair. The injuries include wounds to the bladder, small bowel, kidney, ureter, duodenum, stomach, liver, diaphragm, spleen, pancreas, heart and inferior vena cava.
The faculty and trainees then evaluate the course, using appropriate questionnaires; the faculty also evaluate the trainees.
To date, practising surgeons and trainees in the United States have been the main focus of training. The course has been evaluated extensively by Jacobs and colleagues.10,12
In 2003, the course was introduced into Canada at the University of Toronto, as a first site outside the United States. The main focus at the University of Toronto has been training senior general surgery residents. The aim of the present project was to evaluate this program in the context of a Canadian general surgery residency to determine whether the ATOM course should be established as part of our postgraduate general surgery curriculum.
Method
We present data from 24 senior general surgery residents and 7 ATOM-trained faculty at the University of Toronto. The trained faculty evaluated the residents, taught the course and completed the questionnaire (described below). Information from the faculty was considered important because of their expertise in trauma surgery, which allowed them to evaluate both the course and the trainees.
The residents all completed a pre- and postcourse MCQ examination as well as a self-efficacy questionnaire. The self-efficacy score is based on established social cognitive theory13,14 and asks the participants to judge their own skill level. In the ATOM course, a high self-efficacy score is associated with a high likelihood of success in performing the task, whereas a low self-efficacy score is associated with behaviours such as task avoidance or low level of performance. 15 In the ATOM course, the self-efficacy score is equivalent to a measure of self-confidence in regard to performing procedures in the course. The self-efficacy scale ranges from a low of 1 (very little confidence) to a high of 5 (high level of confidence). This score is assigned for each of 27 life-saving surgical manoeuvres for a maximum total self-efficacy score of 135. Box 1 demonstrates the scale for the self-efficacy scoring of item 11: control of renal artery and vein for renal laceration.
Sample item from self-efficacy measure
Following each item below, please fill in the number that represents the level of confidence you have in performing the following procedures.
11. Control of renal artery and vein for renal laceration
| Example | 1 | 2 |
 | 4 | 5 |
| Very little confidence | Quite a lot of confidence | ||||
A scale of 1–3 was used to evaluate the performance of the participant for each injury. A score of 1 was assigned when the participant was unable after 3 prompts to perform the required manoeuvre (injury identification, developing a correct treatment plan or performing the repair). A score of 2 was assigned when the participant was able to identify the injury, develop a correct treatment plan and perform the repair after 2 prompts or less from the instructor, and a score of 3 was assigned when the participant was able to independently (with no prompts) complete the required tasks. Possible scores in this part of the course therefore ranged from a minimum of 27 to a maximum of 81.
Using a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree), both faculty and residents evaluated the course according to the following items:
Objectives were met.
Surgical skills were improved.
Trauma knowledge was improved.
Clinical judgment in trauma management was improved.
Confidence in approaching trauma was improved.
The live laboratory model was a realistic representation of injury in humans.
A human cadaver model would be preferable to the live laboratory model.
The course more adequately prepares the trainee for dealing with penetrating trauma than regular general surgery training.
The course is more appropriately directed to fourth year than to fifth year.
This course should be continued in the general surgery residency program.
Because the faculty were the teachers and did not take the course, it may not have been entirely appropriate to have them complete the same evaluation form as the residents. However, this information did provide us with an opportunity to assess the faculty’s view of the course through their interaction with the residents during its conduct.
Results
Scores
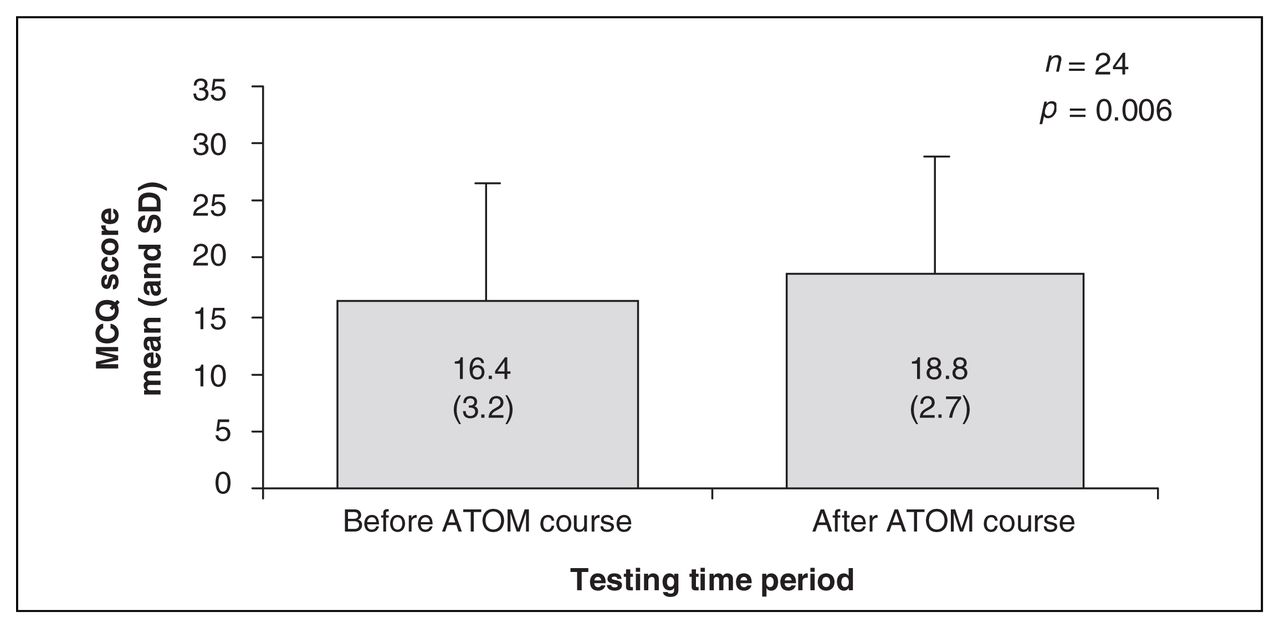
We report the results as means (and standard deviations [SDs]) for the MCQ and self-efficacy scores. With regard to the MCQ, out of a maximum score of 25, the mean precourse score was 16.4 (SD 3.2), compared with a postcourse score of 18.8 (SD 2.7) (p = 0.006, n = 24) (Fig. 1).

MCQ scores: there was a statistically significant improvement in multiple choice performance after the ATOM course. ATOM = Advanced Trauma Operative Management course; MCQ = multiple choice questionnaire; SD = standard deviation.
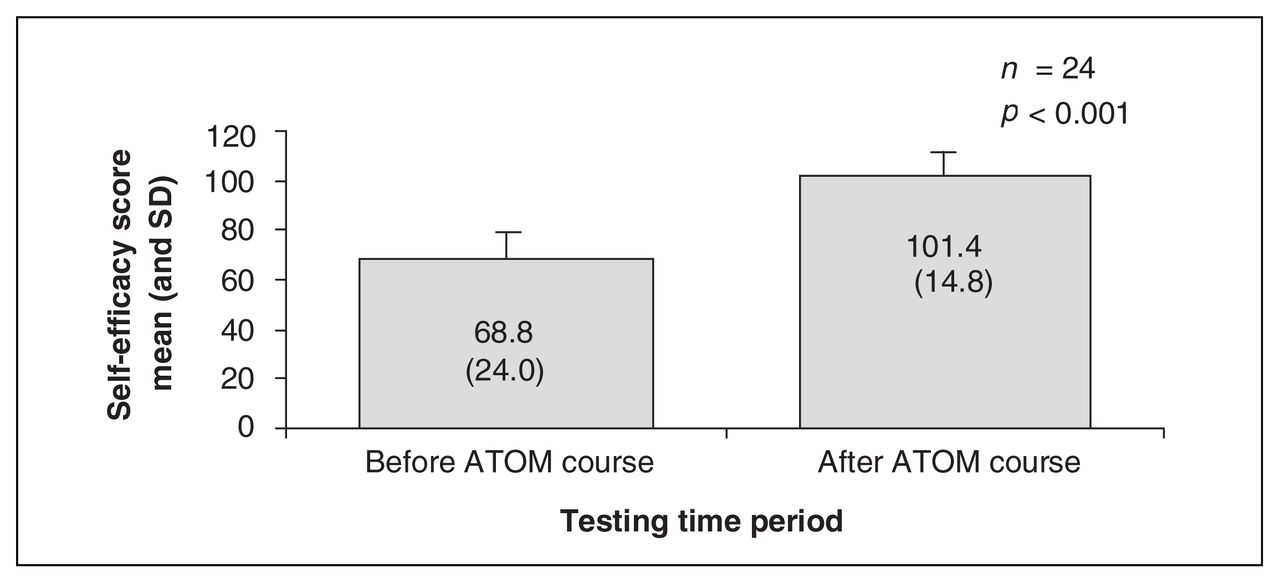
The self-efficacy scores were out of a total minimum of 27 and maximum of 135. The precourse self-efficacy mean score was 68.9 (SD 24.0), and the postcourse mean score was 101.4 (SD 14.8). The pre–post mean difference was 31.7 (SD 16.9) (p < 0.001, n = 24) (Fig. 2).
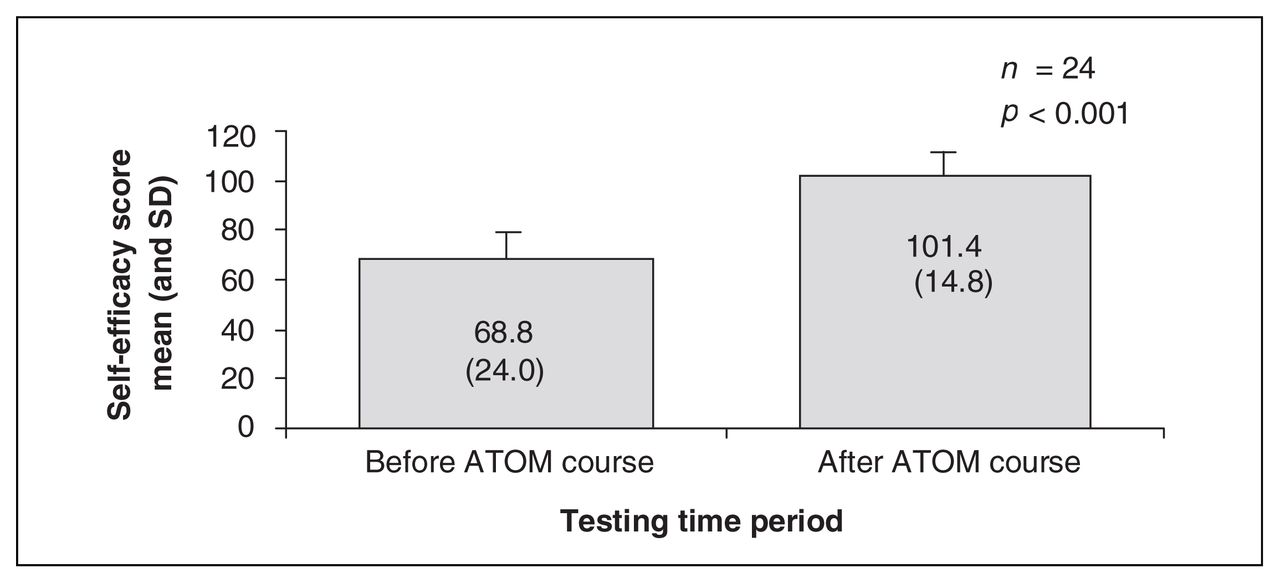
Self-efficacy result. There was a statistically significant improvement in self-efficacy scores after the ATOM course, with the mean pre- and postcourse difference being 31.7 (SD 16.9). ATOM = Advanced Trauma Operative Management; SD = standard deviation.
Evaluation by residents and faculty
Residents assigned a Likert score of 4–5 (agree to strongly agree) to the following items: objectives were met, knowledge was improved, skills were improved, clinical training was improved, clinical judgment was improved, confidence in dealing with trauma was improved, the live model was a realistic representation of these injuries in human and the course should be continued in the fourth rather than the fifth year. All 24 residents assigned scores of 1–2 (highly disagree to disagree) to the statement that the human cadaver was preferable for teaching surgical skills, and 20 of 24 residents assigned a score of 1–3 (strongly disagree to neutral) to the statement that the ATOM course more adequately prepared them for dealing with penetrating trauma than their regular general surgery training.
With regard to overall course evaluation, faculty assigned a score of 4–5 to the following items: objectives were met, surgical skills were improved, trauma knowledge improved, clinical judgment improved, confidence in managing penetrating trauma improved, the laboratory model was a true representation of human trauma, the course added significantly to surgical training and the course should be continued in residency. Six of the 7 faculty graded as 4–5 the statement that the course would be more appropriately directed to fourth year. Six of the 7 faculty graded as 1–2 (strongly disagree to disagree) the statement that the human cadaver is a preferred model for teaching the surgical skills.
With regard to faculty evaluation of students, the mean total score for all participants was 73.9 (SD 6.4), with individual scores ranging from 65 to 81. Of the participants, 34% achieved the maximum score of 81. No resident was assigned a score of 1 for any of the injuries in the category of injury identification, developing a correct treatment plan and performing the surgical repair.
Discussion
Traditionally, the operating room has been the venue for teaching basic surgical skills to residents. Current fiscal constraints in health care demand that less time be spent in the operating room, which decreases training time for residents. It has also been suggested that resident-performed operations may cost more.16 Further, serious and complex surgical problems require the immediate skills of expert surgeons, which again decreases residents’ opportunities for “hands-on” skills training in lifesaving procedures.7 There are also ethical concerns about teaching and learning surgical skills on patients.17 Quite apart from these factors, the present trend in nonoperative management of torso trauma decreases the opportunites for training in operative management.
The ATOM course was developed as one of the many strategies in our surgical residency to address the lack of opportunities for developing operative repair techniques for major penetrating injuries. The Advanced Trauma Operative Management course was introduced in Hartford, Connecticut, in 2000 and since then 14 sites in the U.S.A, Canada and Africa have been developed with over 465 students and over 100 instructors being trained.18
This program has been extensively evaluated by Jacobs and colleagues10,12 in the US context, and the results have been very gratifying. In this study, we analyzed the same program in the context of a Canadian general surgery residency program. All residents agreed or strongly agreed that the objectives were met and that trauma knowledge and skills, clinical training and judgment and confidence in dealing with trauma improved. Although subjective, these results demonstrate strong support for continuing the ATOM program in our general surgical residency. We demonstrated very high self-efficacy scores (increasing from mean 68.9, SD 24.0, to mean 101.4, SD 14.8, after ATOM), reflecting increasing confidence in performing corrective surgical manoeuvres in trauma management. As well, there was a statistically significant improvement in trauma knowledge as indicated by the MCQ scores (mean 16.4, SD 3.2, increasing to mean 18.8, SD 2.7, out of a maximum score of 25). We had anticipated a greater increase in the MCQ scores after ATOM, and the smaller-than-anticipated difference may be due to the program’s major emphasis on technical skills as opposed to trauma knowledge skills.
The DSTC course is one of the other initiatives aimed at providing similar exposure to trainees and surgeons in the field of trauma. This course has also been strongly endorsed by the International Association for the Surgery of Trauma and Surgical Intensive Care. Major differences between the 2 courses are the length of the course (1 day for the ATOM course v. a minimum of 2 days for the DSTC course) and the 1-to-1 ratio of student to faculty in the live-animal model of the ATOM course, compared with the lower ratio of faculty to students in the DSTC course. Undoubtedly, both of these courses play a significant role in filling the void created by the lack of operative opportunities for dealing with trauma. In our course, the residents preferred the live-animal experience as opposed to cadaver dissection (which was not conducted in the course). Their opinion was therefore based on exposure to cadaver models in our surgical skills centre.
We have demonstrated that the ATOM course can be conducted in a reasonable time frame (1 day) and that it has a very high acceptance rate among our surgical residents. There was also very strong support for continuing this program in our general surgical residency, but the trainees and the faculty both were strongly in favour of having this program introduced in the penultimate year rather than final year of the general surgical residency, with the hope that in their final year of residency the trainees would have an opportunity to further reinforce the training provided through the ATOM program.
After our experience at the University of Toronto, another Canadian course was developed in March 2006 at the Calgary Foothills Hospital, where 8 general surgical residents were trained and additional faculty prepared for the establishment of ATOM training in their general surgical residency. In 2007, ATOM courses were introduced into the general surgery residency programs in Calgary and Edmonton. Other trauma directors have informally expressed interest in starting their own ATOM program or participating in the already-established programs in Eastern and Western Canada. We anticipate that this program will eventually be adopted by most of our general surgical residency training programs throughout Canada.
Acknowledgements
This study was supported in part by the University of Toronto Dean’s Excellence Fund.
Footnotes
Presented at the joint meeting of the Trauma Association of Canada and the PanAmerican Trauma Society, Banff, Alta., March 23–25, 2006.
Competing interests: None declared.
Contributors: All authors designed the study, reviewed the article once written, and gave final consent for publication. Drs. Ali, Ahmed and Jacobs acquired and analyzed the data. Drs. Ali and Ahmed wrote the article.
- Accepted April 4, 2007.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.