


Abstract
Background: The purpose of this study was to assess the functional outcome and causes of persistent disability in patients with isolated femoral shaft fractures treated at an academic level-1 trauma centre.
Methods: We prospectively enrolled 40 consecutive skeletally mature patients with isolated, nonpathologic diaphyseal femur fractures. All patients underwent fracture reduction and fixation using an antegrade locked intramedullary nail. We measured functional outcome using the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index and the Short Musculoskeletal Functional Assessment (SMFA). We obtained visual analog scores for pain in the groin, buttock, thigh and knee 6 months after the injury.
Results: Joint-related and musculoskeletal outcome scores improved gradually from the baseline assessment to the 6-month review. Mean scores (and standard deviations [SDs]) on the WOMAC index improved gradually from 57 (23) to 24 (22) for pain, from 57 (25) to 30 (20) for stiffness and from 70 (21) to 21 (23) for function (p < 0.001). The mean SMFA score (and SD) improved from 64 (13) to 25 (20) (p = 0.024). We noted no further improvements in functional outcome measures from the 6-month to the 12-month assessment (p > 0.21). Patients reported more pain in the knee than in other anatomic locations; the mean pain scores (and SDs) were 3.7 (3.1) in the knee, 2.5 (2.7) in the thigh, 1.7 (2.7) in the buttock and 1.0 (1.7) in the groin (p = 0.003). We noted correlations between knee pain and WOMAC pain (ρ = 0.748, p < 0.001), function (ρ = 0.701, p < 0.001) and SMFA (ρ = 0.733, p < 0.001). We noted weaker correlations between thigh, groin and buttock pain and functional outcomes, with ρ scores ranging from 0.2 to 0.55.
Conclusion: Recovery from femur fractures occurs most rapidly in the first 6 months after injury. Residual deficits in functional outcome were still measurable 12 months after injury. Knee pain was the most common and most severe source of patient discomfort 12 months after isolated femur fractures, and demonstrated moderate to good correlation with general and joint-specific functional outcome measures.
Disability following a fracture of the femoral shaft is prolonged, even when bone union occurs without complication. Treatment with an antegrade locked intramedullary nail is generally considered to be successful when union occurs predictably and malalignment is avoided. In fact, union rates exceeding 95% and malalignment rates below 5% are expected after intramedullary nailing of midshaft fractures.1–8 Nonetheless, patients report disability long after femoral fracture, even when surgery is accomplished with technical success and union is achieved.
What are the causes of prolonged disability? The time course of recovery is poorly understood, and the sources of disability are similarly unclear. There is general agreement that knee pain is a substantial functional problem following fracture of the femoral shaft. Ricci and colleagues9 reported knee pain in up to 36% of patients with fractures of the femoral shaft, but the severity and clinical importance of this knee pain remains unknown. Causes of knee pain are generally poorly understood. Various theories propose that intra-articular pathology, intraosseous hypertension, prominent hardware and muscle deconditioning may be the primary sources of knee pain following fracture of the femoral shaft.10–16 Hip pain is also reported after intramedullary nailing. About 10% of patients report hip pain.9 Sources of hip pain include damage to the abductor musculature related to nail insertion.17,18
There are various reasons for the lack of knowledge on disability following fracture of the femur. First, fractures of the femoral shaft often occur in a young, mobile population, thus long-term follow-up can be difficult. Second, these fractures are commonly associated with other injuries, thus ascribing disability to the fracture of the femoral shaft alone may be misleading. Third, issues such as muscle deconditioning are vague, generally nonsurgical issues. There are many other reasons for the lack of knowledge on disability following femoral fracture. Further study is certainly required.
The purpose of our study was to assess functional outcomes and sources of disability following fractures of the femoral shaft in patients with isolated injuries. We sought to assess patient-related functional outcomes and determine the relative importance of knee pain. We hypothesized that knee pain was associated with adverse functional outcome following isolated fractures of the femoral shaft treated with an antegrade intramedullary nail.
Methods
We enrolled 40 patients with isolated diaphyseal fractures of the femur treated with a locked antegrade intramedullary nail in our prospective cohort study, which took place from July 2001 to August 2003. We enrolled only patients who satisfied the inclusion and exclusion criteria outlined in Box 1. We employed very strict exclusion criteria to ensure that only patients with isolated diaphyseal femoral fractures were included. The London Health Sciences Centre institutional review board approved our study (IRB 8394E).
Study inclusion and exclusion criteria
| Inclusion criteria |
|
|
|
|
|
|
|
| Exclusion criteria |
|
|
|
|
|
|
|
|
|
|
|
The mechanisms of injury were motor vehicle collisions in 29 patients (including 3 snowmobile and 3 motocross injuries), recreational or sports injuries in 4 patients and falls in 7 patients. Of the 40 patients, 39 had surgery within 24 hours after injury. Reduction was accomplished by closed manual traction in 27 patients, by fracture table in 9 patients and using an open reduction technique in 4 patients. One of 7 operating surgeons, all of whom were experienced in intramedullary nailing techniques, performed or directly supervised the surgeries. Two orthopedic trauma surgeons (D.W.S., M.M.) performed 26 of the procedures.
The surgeons used a standard surgical technique. Under image intensifier control, they inserted a 3-mm guide pin percutaneously into the piriformis fossa. They confirmed the accuracy of their guide wire placement fluoroscopically. Next, they made a 2- to 4-cm incision adjacent to the guide wire for placement of a cannulated entry reamer. Subsequently, they inserted a ball-tipped guide wire through the piriformis fossa, across the fracture site and centrally positioned in the distal femur. They treated all fractures with a reamed femoral nail. They performed the reaming using incremental sized reamers until they noted slight cortical chatter at the level of the isthmus. At that point, they selected a femoral nail about 1 mm smaller than the final reaming size and inserted it through the percutaneous incision. They used TRIGEN (Smith & Nephew) titanium femoral antegrade nails in 37 of 40 patients. In 3 patients, the surgeons envisioned difficulty achieving a piriformis fossa start point, so they used a TRIGEN trochanteric antegrade nail through a percutaneous trochanteric starting point. They routinely examined patients for a fracture of the femoral neck (using internal and external rotation fluoroscopic views) and for knee pathology (using physical examination while under anesthesia).
In-hospital care followed a standard protocol. After study enrolment, patients completed a baseline medical questionnaire and 2 functional outcome questionnaires: the Western Ontario and McMaster Universities Arthritis (WOMAC) index and the Short Musculoskeletal Functional Assessment (SMFA). The WOMAC is a validated joint-specific functional outcome measure used to determine pain, stiffness and dysfunction related to arthritis of the knee. The SMFA is a validated general functional outcome measure used in a variety of acute and chronic conditions.
We followed patients for a minimum of 12 months. The primary outcomes were based on functional outcomes at 6 months. We measured functional outcomes at baseline and after 2 weeks, 6 weeks, 3 months, 6 months and 12 months. The total completion rate of functional outcome questionnaires was 87.1% during the 12 months. One of 2 fellowship-trained orthopedic trauma surgeons (D.W.S. or M.M.) conducted the follow-up visits and assessments. At each visit, the surgeon obtained anteroposterior and lateral radiographs, reviewed the patient’s history and performed a physical examination. Patients completed 2 questionnaires (WOMAC and SMFA). One of 3 research assistants (J.L., A.D., C.T.) contacted all patients before each appointment to ensure completion of the appropriate functional outcomes questionnaire and to encourage clinic attendance. The research assistant met each patient at the follow-up visits to collect the completed questionnaires and to distribute a new set of questionnaires. The study procedures for the next visit were explained at each follow-up visit. At 6 months, all patients completed a detailed questionnaire to determine their satisfaction with the surgery, employment status and degree of disability. They also determined a score related to pain in the buttock, groin, thigh and knee using a visual analog scale. To complete the visual analog score, the examiner confirmed with the patient that they understood the description of the various sites by pointing to the anatomic region of interest.
We assessed all patients with imaging of the ipsilateral knee 6 weeks after the injury. We obtained computed tomography scans of rotational alignment and long leg standing radiographs for overall limb alignment after 6 months. We considered alignment to be abnormal if there was more than 1 cm of shortening, 5° of varus or valgus, more than 5° of internal rotation or more than 15° of external rotation.
Statistical analysis
We compared the results of functional outcome scoring using analysis of variance (ANOVA). We used the Spearman correlation test to correlate functional outcomes with visual analog scores for pain in the buttock, groin, thigh and knee. We considered results of both statistical tests to be significant at p < 0.05.
Results
A total of 368 patients had a femoral fracture treated with intramedullary nailing during the study period. We excluded 72 patients because their fractures extended beyond the femoral diaphysis; 26 patients because they had a known or suspected pathologic fracture; 97 patients because of age (28 were younger than 17 and 69 were older than 65); 37 patients because of associated polytrauma; 68 patients owing to the presence of other fractures, medical conditions or the need for additional procedures; and 24 patients for other nonmedical reasons (e.g., language, distance of their primary residence from the hospital) resulting in presumed difficulties with follow-up or study compliance. Of the 44 eligible patients, 3 patients refused to participate and 1 patient enrolled but withdrew less than 2 weeks later. This left 40 patients (34 men and 6 women) with a mean age of 29 (range 17–65) years for inclusion in our study. All 40 patients had complete follow-up.
After surgery, we considered alignment to be acceptable in 35 of 40 patients; 3 patients had external rotation between 15° and 25°, and 2 patients had shortening between 1 and 2 cm. No patients had significant varus or valgus deformity, and none of the 5 patients with unacceptable alignment wished to have a secondary procedure to correct the alignment. Most of the patients (38 of 40, 95%) achieved union without additional surgery requirements. Two patients required additional surgery to treat a delayed union. In both these patients, union was achieved following exchange intramedullary nailing. One of these patients had the highest pain score in the thigh, whereas the other had equal pain scores in the thigh and knee.
Results of the visual analog scale scores for pain in the buttock, thigh, groin and knee are shown in Figure 1. The overall mean pain scores (and standard deviations [SDs]) were 3.8 (2.9) for the knee, 2.3, (2.5) for the thigh, 2.2 (2.6) for the buttock and 1.0 (1.5) for the groin. Pain scores were significantly higher for the knee than for the other sites (p < 0.001).

Visual analog pain scores 6 months after injury, by anatomic location of pain.
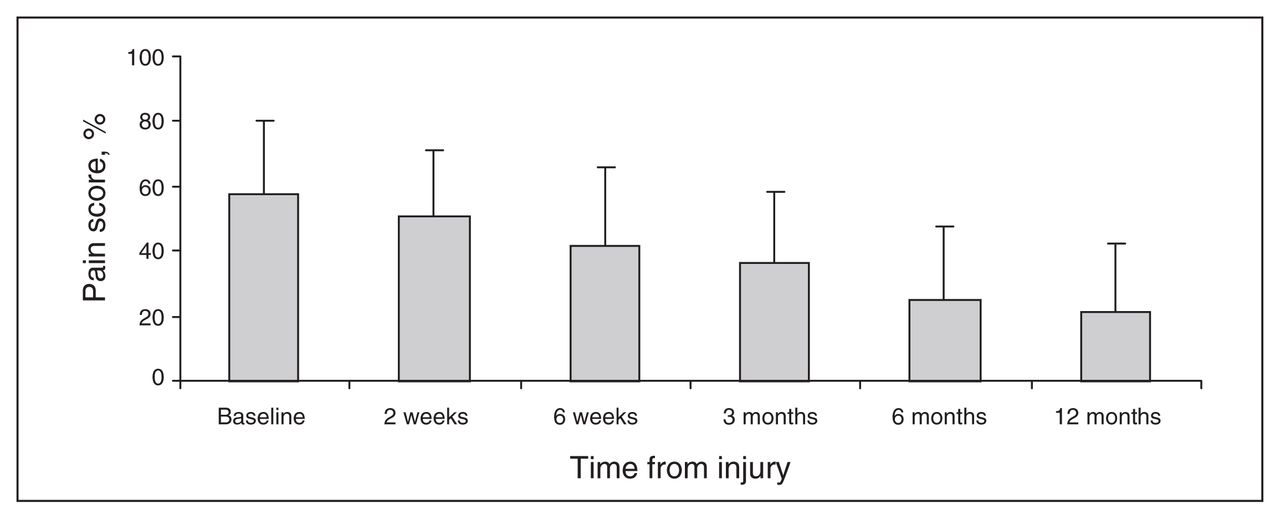
We compared scores on the visual analog scale for the various sites. Overall, 22 patients reported maximum pain in the knee, 8 patients reported maximum pain in the thigh, 3 patients reported maximum pain in the buttock and 3 patients reported maximum pain in the groin (p < 0.001); the remaining 4 patients reported no pain (Fig. 2). We compared pain in the groin, buttock, thigh and knee with the results of functional outcome assessment at the 6-month follow-up visit. We used data from the 6-month visit because these data were collected at the same time as the pain data and because the functional outcome scores had essentially reached a plateau by the 6-month assessment for the WOMAC pain, stiffness and function scores and for the SMFA disability score. Figure 3 shows a sample of the change in functional outcomes over time for the WOMAC score. Results for 6 and 12 months reflected lower pain scores compared with all other intervals (p < 0.001), but results comparing 6 and 12 months did not differ (p = 0.621).

Number of patients reporting maximum pain at various anatomic locations.

Western Ontario and McMaster University Osteoarthritis index (WOMAC) pain scores, by time from injury.
We compared pain and functional outcome scores to determine whether there was an association between knee pain and functional outcome scores. We plotted pain and functional outcomes on scatter graphs and assessed correlations using the Spearman correlation test. We noted the strongest correlations between knee pain and WOMAC pain (ρ = 0.748, p < 0.001), function (ρ = 0.701, p < 0.001) and SMFA (ρ = 0.733, p < 0.001). We noted weaker correlations between thigh, groin and buttock pain and functional outcomes, with scores ranging from ρ = 0.2 to ρ = 0.55.
Discussion
Fractures of the femur involve major trauma. The femur is the second most commonly fractured long bone, with about 325 000 fractures per year in the United States.1 Fractures of the femur are associated with a high prevalence of serious injuries elsewhere, such as the head, chest and abdomen, and they generally heal well. The femur has a rich vascular supply, and most recent reports describe union rates between 90% and 99% when treatment with an antegrade locked intramedullary nail is performed.1–7 Nonetheless, fractures of the femur remain a source of major disability for patients. In many cases, disability is secondary to injuries to other body systems. In other instances, lower extremity disability relates to residual fracture malalignment. Recently, attention has been directed to the high incidence of knee pain in the presence of femoral fractures that seems to occur commonly despite successful treatment.
The etiology of knee pain following fractures of the femoral shaft is essentially unknown. It is thought that the mechanism of injury may provide further insight into knee pain following femoral fractures. Epidemiologic studies have shown correlation between the mechanism of injury and the types of injuries associated with femoral fractures. 10 Other studies have investigated the pathology in the so-called “dashboard knee.”11 The position of the knee at the time of impact and the direction of force applied may allow a prediction of the type and severity of knee injuries associated with femoral fractures. After vehicular trauma, the most common cause of fractures of the femoral shaft, it is often difficult to determine the exact mechanism of injury. Unrestrained patients may have multiple potential mechanisms and, with associated injuries, recollection of the traumatic event can be extremely difficult. In some cases, major ligamentous injuries occur in the knee in association with femoral fractures.12,19,20 These can often be missed, thus it is essential to maintain a high index of suspicion for knee pathology after fractures of the femoral shaft.
Recently, osteochondral injuries have been identified as potential sources of pain and disability following injuries to the knee. Osteochondral injuries are impaction fractures of the bone and cartilage that are not seen on plain radiographs but can be identified easily using magnetic resonance imaging. Osteochondral injuries are frequently seen in conjunction with ligamentous tears and other knee injuries and may act as a source of long-term pain and disability.21,22 The role of osteochondral injuries to the knee in femoral fractures has not been studied.
Limitations
Our study had several weaknesses. Our intention was to include only isolated fractures of the femoral shaft to avoid confounding variables that may also have been related to knee pain. In addition, we followed strict inclusion criteria to ensure that only midshaft fractures were included. Because of the strict inclusion criteria, we were obliged to exclude many patients treated with an intramedullary nail.
However, our follow-up was nearly complete, with all 40 patients completing the functional outcome portion of the study. The use of 2 validated outcome measures to assess outcome previously had not been applied to this population, and limited data were available regarding the standard timing of functional improvement after a femoral fracture.
We did not seek to explain the origin of knee pain following femoral fractures. Various sources of knee pain might be assumed, including prominent hardware, quadriceps dysfunction, intraosseous hypertension and intra-articular derangements. The use of magnetic resonance imaging may be useful in future studies to determine the relation, if one exists, between intra-articular pathology and functional outcome. The incidence of knee pain was analagous to other reports; however, a recent study by Ricci and colleagues9 noted that hip pain was commonly reported after antegrade intramedullary nailing. Knee pain was more common and severe compared with buttock or groin pain in our study, which may be explained by the use of a percutaneous entry portal in contrast to the open portal used by Ricci and colleagues.9
Specific to the surgical implant used in our study is the design of the locking screws. For the majority of the study, we used a self-drilling, self-tapping screw. These screws have a sharp tip and a hexagonal head. Four patients subsequently required hardware removal owing to screw irritation proximal to the knee. More recently, the manufacturer has converted to a non–self-tapping screw and, since July 2003, the locking screws have had a rounded design. We do not have sufficient data at this time to determine whether knee pain has been improved with the use of the rounded locking screw design.
In conclusion, we noted knee pain to be an important source of disability after a fracture of the femoral shaft. In addition, knee pain was correlated with both general and joint-specific functional outcome measures. We believe that a systematic investigation into the causes and treatment of knee pain after fractures of the femoral shaft merits further investigation.
Acknowledgement
We received funding from the Lawson Health Research Institute in support of this study.
Footnotes
Competing interests: None declared.
Contributors: Drs. Sanders and MacLeod designed the study. Drs. Sanders and MacLeod and Mses. Lydestad, Domonkos and Tieszer acquired the data, which Dr. Sanders and Mses. Charyk-Stewart, Lydestad, Domonkos and Tieszer analyzed. Dr. Sanders and Ms. Charyk-Stewart wrote the article, which all authors reviewed. All authors gave final approval for publication.
- Accepted March 14, 2006.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools





