

Abstract
Background: Sentinel lymph node biopsy (SLNB) for melanoma plays a central role in determining prognosis and guiding treatment and surveillance strategies. Despite widely published guidelines for SLNB, variation exists in its use. We aimed to determine the frequency of and predictive factors for SLNB in patients with clinically node-negative melanoma in British Columbia.
Methods: A retrospective review was performed of patients with clinically node-negative melanoma diagnosed between January 2015 and December 2017. Patients included had a Breslow depth greater than 0.75 mm or a Breslow depth less than or equal to 0.75 mm with ulceration, or a mitotic rate greater than or equal to 1/mm2. SLNB was considered to be indicated for clinical stages IB to IIC (American Joint Committee on Cancer’s AJCC Cancer Staging Manual, seventh edition).
Results: A total of 759 patients were included. SLNB was performed in 54.8% (363/662) of patients when indicated. SLNB was more likely to be performed for tumours with a Breslow depth greater than 1.0 mm or a mitotic rate greater than or equal to 1/mm2. SLNB was less likely to be performed in patients older than 75 years and with a nonextremity tumour location. Compliance with SLNB guidelines decreased distant recurrence but did not significantly affect regional recurrence, nor did it have a significant impact on overall survival among patients aged 75 years and younger.
Conclusion: SLNB is being underutilized in British Columbia. These results are concerning and highly relevant given the rapidly evolving field of adjuvant systemic therapy for high-risk patients and the increased proportion of patients who should be considered for SLNB on the basis of the eighth edition of the AJCC Cancer Staging Manual and current guidelines. Efforts should be made to increase the use of SLNB in appropriate patients.
In Canada, cutaneous malignant melanoma accounts for approximately 3% of all new cancer diagnoses and 80% of skin cancer–related deaths.1,2 The lifetime risk of developing melanoma is 1 in 59 for women and 1 in 73 for men, respectively, with mortality rates ranging between 1 in 240 to 1 in 395.1,2 Worldwide, the incidence of melanoma continues to rise.3
The majority of patients with melanoma present with early, clinically node-negative disease.4,5 Staging with sentinel lymph node biopsy (SLNB) is indicated for most patients with clinically node-negative disease. This allows identification of occult nodal metastases, which has important prognostic implications and helps guide management.6–9 The importance of SLNB in cutaneous melanoma has been well established.10
The MSLT-I trial established SLNB as an accurate prognostic tool and laid the foundation for determining the impact of regional lymphadenectomy on survival, which was investigated in follow-up analyses.10,11 After MSLT-I, the benefit of completion lymph node dissection (CLND) after a positive SLNB was challenged by 2 landmark trials. The DeCOG-SLT trial (published in 2016) and the MSLT-II trial (published in 2017) both failed to show a survival benefit with CLND.12,13 As a result, a positive SLNB is no longer an absolute indication for a CLND.14 Despite this, accurate staging of the regional nodal basins remains imperative. SLNB provides important prognostic information that is used to identify patients who may benefit from enhanced surveillance, adjuvant systemic therapy or enrolment in clinical trials.9,15
There is a growing body of high-level evidence in support of adjuvant systemic therapy for stage III (pT1–4N1) melanoma.16–19 Adjuvant immunotherapy and targeted therapy have demonstrated substantially improved outcomes including improved recurrence-free survival (RFS), distant metastasis–free survival (DFMS) and overall survival (OS) in resected stage III melanoma.16–18,20,21 Although these studies required that patients undergo a CLND, it is recognized that routine CLND is no longer standard of care.22 Taken together, these data indicate that complete and accurate staging remains relevant in the post-MSLT-II era.
SLNB indications are well established and have been widely published (Table 1). The National Comprehensive Cancer Network (NCCN) recommends that SLNB be considered in patients with stage IB (0.8–1.0 mm without ulceration or ≤ 1.0 mm with ulceration) melanoma, and it should be offered to patients with stage IB (T2a) or stage II melanoma.6 Similarly, the clinical practice guidelines of the American Society of Clinical Oncology and Society of Surgical Oncology recommend that SLNB should be offered to patients with intermediate-thickness (T2 and T3) melanoma and considered for those with thin (T1b) and thick melanoma (T4).23 The European Society for Medical Oncology recommends that SLNB be performed for patients with T1b or greater melanoma.24 Finally, a Canadian clinical practice guideline recommends that SLNB be performed in patients with T2 and T3 melanoma and be discussed with patients with T1 melanoma in the presence of high-risk features.14 Despite the existence of clear guidelines and the strong rationale for performing SLNB, variation exists in the use of SLNB, and it is often underutilized.25–28
Society SLNB recommendations
The use of SLNB in the province of British Columbia has not previously been evaluated, to our knowledge. The primary objective of this study was to determine the frequency with which SLNB is performed for patients with clinically node-negative disease in BC and predictive factors for undergoing SLNB. Secondary objectives were to determine if noncompliance with SLNB guidelines affects regional or distant recurrence, or OS.
Methods
A retrospective study was performed of patients treated at tertiary, regional and community centres in BC with clinically node-negative cutaneous malignant melanoma diagnosed between Jan. 1, 2015, and Dec. 31, 2017. Patients were identified using the Sunset pathology database.
Patients were included who had cutaneous malignant melanoma with a Breslow depth greater than 0.75 mm, or a Breslow depth less than or equal to 0.75 mm with ulceration or a mitotic rate of at least 1/mm2. Patients noted to have regional or distant metastases before undergoing definitive surgical treatment were excluded.
Data collected for each patient included demographic information (sex, age at diagnosis), tumour characteristics (location of the primary tumour, Breslow depth, ulceration, mitotic rate, lymphovascular invasion and sentinel node status) and treatment characteristics (type of surgery, date of last follow-up). Rates of regional and distant recurrence and survival at the time of last follow-up were recorded.
The primary objectives were to determine the frequency with which SLNB was performed and predictive factors for undergoing SLNB. Secondary objectives were to determine if noncompliance with SLNB guidelines affected regional or distant recurrence, or OS. The study was conducted after approval was obtained from the University of British Columbia Cancer Research Ethics Board.
Statistical analysis
Demographic, tumour and treatment characteristics were collected and summarized using descriptive statistics. Stage was determined on the basis of both the seventh and eighth editions of the American Joint Committee on Cancer’s AJCC Cancer Staging Manual, but stage based on the seventh edition was used to determine if SLNB was indicated. SLNB was considered to be indicated in any patient with clinical stage IB or II melanoma.
Predictive factors for undergoing SLNB were analyzed using logistic regression models. The factors that were included were age, location of the primary tumour, Breslow depth, ulceration, mitotic rate and lymphovascular invasion. Patients with incomplete data were excluded from the analysis. Multivariable analyses selected covariates using stepwise backward selection on the basis of the Akaike information criterion (AIC), starting from an initial model including SLNB compliance and all 6 factors described above. A subset analysis was performed to identify predictive factors for undergoing SLNB in patients 75 years of age and younger.
The impact of noncompliance with SLNB guidelines on regional (nodal or in-transit or both) and distant recurrence was assessed by logistic regression analysis for the entire population and for patients 75 years of age and younger. A Kaplan–Meier analysis was performed to determine if non-compliance with SLNB recommendations affected OS. Statistical significance was set at p < 0.05. Statistical analysis was performed using R (version 4.0.3).
Results
Study population
A total of 759 patients were included. Patient and tumour characteristics are summarized in Table 2. The mean age at diagnosis was 66 years (standard deviation 16.3 yr, range 19–104 yr). Tumours were located most commonly on the extremity (43.9%) followed by the trunk (33.6%). Although nearly all (94.6%) patients underwent wide local excision (WLE) of the primary tumour, 41 patients (5.4%) underwent only a skin biopsy with no record that they went on to have a formal WLE.
Characteristics of study population
Rate of SLNB
SLNB was indicated in 662 patients and performed in 363 patients (54.8%). The rate of SLNB was lowest for those with clinical stage IIC (35.2%) and highest for those with stage IIA (64.1%). SLNB was indicated in 451 of 529 patients aged 75 years or younger and performed in 298 of these patients (66.1%). Among patients older than 75 years of age, SLNB was indicated in 212 of 230 patients and performed in 65 patients (30.7%). By primary tumour site, the SLNB rate was lowest for tumours on the head and neck (32.6%) and highest for tumours on the extremity (65.9%) (Figure 1). The SLNB result was positive in 11.8% of patients (43 of 363). When the same indications for SLNB were applied to patients staged according to the eighth edition of the AJCC Cancer Staging Manual, SLNB would have been indicated in 750 of 759 patients (98.8%).
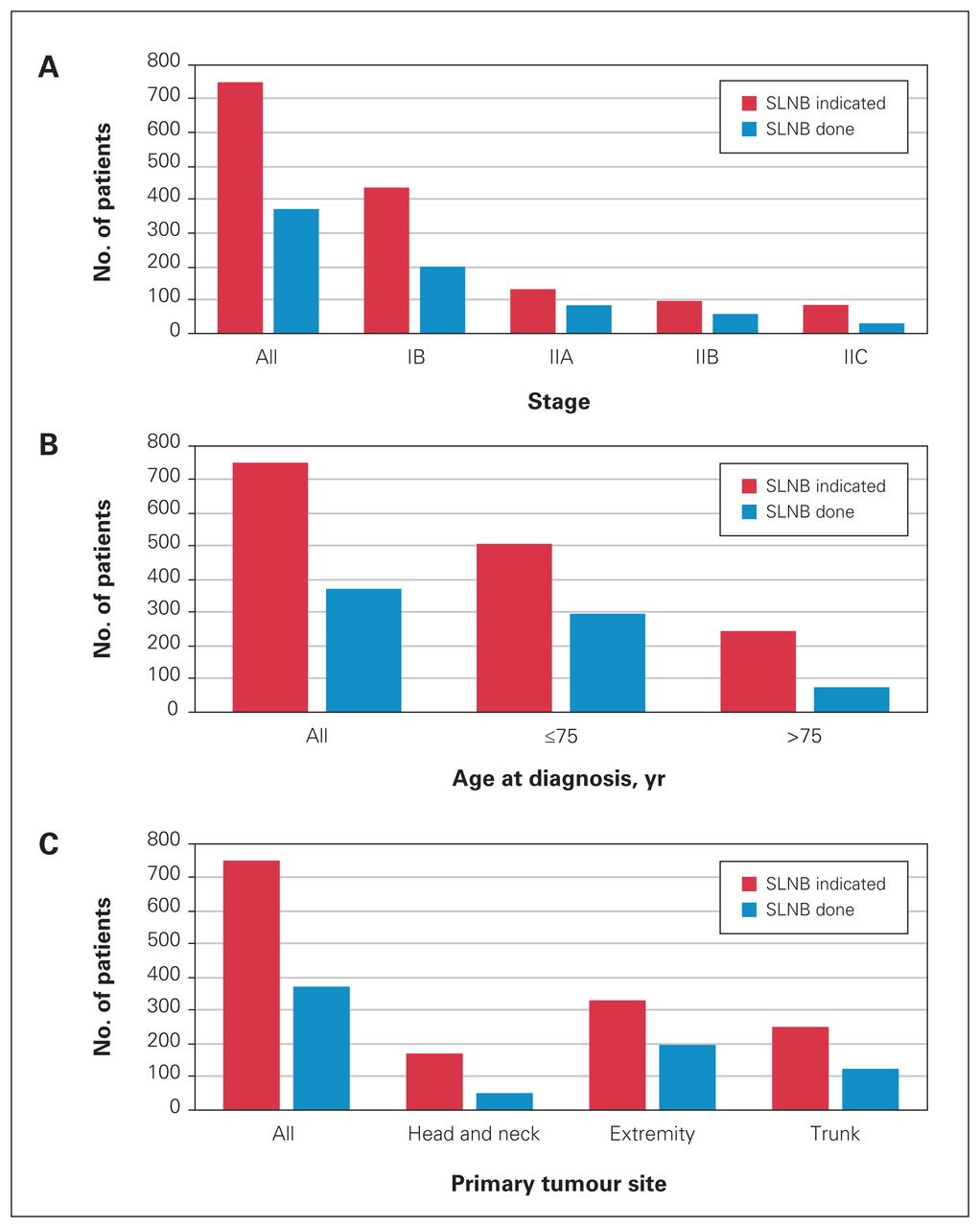
(A) SLNB indication and completion by the eighth edition of the AJCC Cancer Staging Manual, (B) age at diagnosis and (C) primary tumour site. SLNB = sentinel lymph node biopsy.
Predictive factors for undergoing SLNB
All patients
Significant predictive factors on univariable analysis were patient age, primary tumour location, Breslow depth and mitotic rate. On subsequent multivariable analysis, patients older than 75 years (odds ratio [OR] 0.15, 95% confidence interval [CI] 0.09–0.26, p < 0.001) or with a primary tumour on the trunk (OR 0.50, 95% CI 0.33–0.76, p = 0.001) or head and neck (OR 0.23, 95% CI 0.14–0.36, p < 0.001) were less likely to undergo SLNB (Table 3). Patients were more likely to undergo SLNB if they had a Breslow depth of 1.01–4.0 mm (OR 17.0, 95% CI 10.3–29.3, p < 0.001) or greater than 4.0 mm (OR 6.8, 95% CI 3.6–13.0, p < 0.001), a mitotic rate of 1/mm2 or greater (OR 1.8, 95% CI 1.1–2.9, p = 0.040) or lymphovascular invasion (OR 3.3, 95% CI 1.1–11.2, p = 0.041).
Multivariable analysis: all patients
Patients aged 75 years and younger
When patients older than 75 years were excluded, significant predictive factors on univariable analysis were primary tumour location, ulceration, Breslow depth and mitotic rate. On subsequent multivariable analysis SLNB was less likely to be performed with a primary tumour located on the trunk (OR 0.33, 95% CI 0.19–0.57, p < 0.001) or head and neck (OR 0.17, 95% CI 0.09–0.32, p < 0.001) (Table 4). SLNB was more likely to be performed in the presence of ulceration (OR 2.11, 95% CI 1.10–4.14, p = 0.028) and in tumours with a Breslow depth of 1.01–4.0 mm (OR 27.6, 95% CI 14.9–54.1, p < 0.001) or greater than 4.0 mm (OR 17.8, 95% CI 7.6–43.7, p < 0.001) or a mitotic rate of 1/mm2 or greater (OR 1.90, 95% CI 1.00–3.33, p = 0.040).
Multivariable analysis: patients aged 75 years and younger
Impact on regional and distant recurrence
The median follow-up was 27.5 (range 14–52) months, during which 72 patients (9.5%) developed regional recurrence and 66 patients (8.7%) developed distant recurrence in the entire study population. Recurrence rates for the entire study population by Breslow depth are shown in Table 5. Among patients who underwent SLNB, recurrence occurred more commonly in those with pathologic stage III disease than those with stage II disease. This held true for both regional (6.8% v. 32.6%) and distant recurrence (5.5% v. 14.0%). Noncompliance with SLNB guidelines had no significant impact on regional recurrence overall (OR 1.27, 95% CI 0.78–2.06, p = 0.17) or when stratified by clinical stage (stage I: OR 1.02, 95% CI 0.34–2.79, p = 0.49; stage II: OR 1.10, 95% CI 0.61–1.98, p = 0.37). Noncompliance with SLNB guidelines was significantly associated with increased distant recurrence (OR 1.86, 95% CI 1.12–3.10, p = 0.008). On stratified analysis, noncompliance significantly affected distant recurrence for patients with stage I disease (OR 4.33, 95% CI 0.92–30.46, p = 0.041), while statistical significance was not achieved for patients with stage II disease (OR 1.38, 95% CI 0.78–2.45, p = 0.14).
Regional and distant recurrence: all patients
Impact on survival
All patients
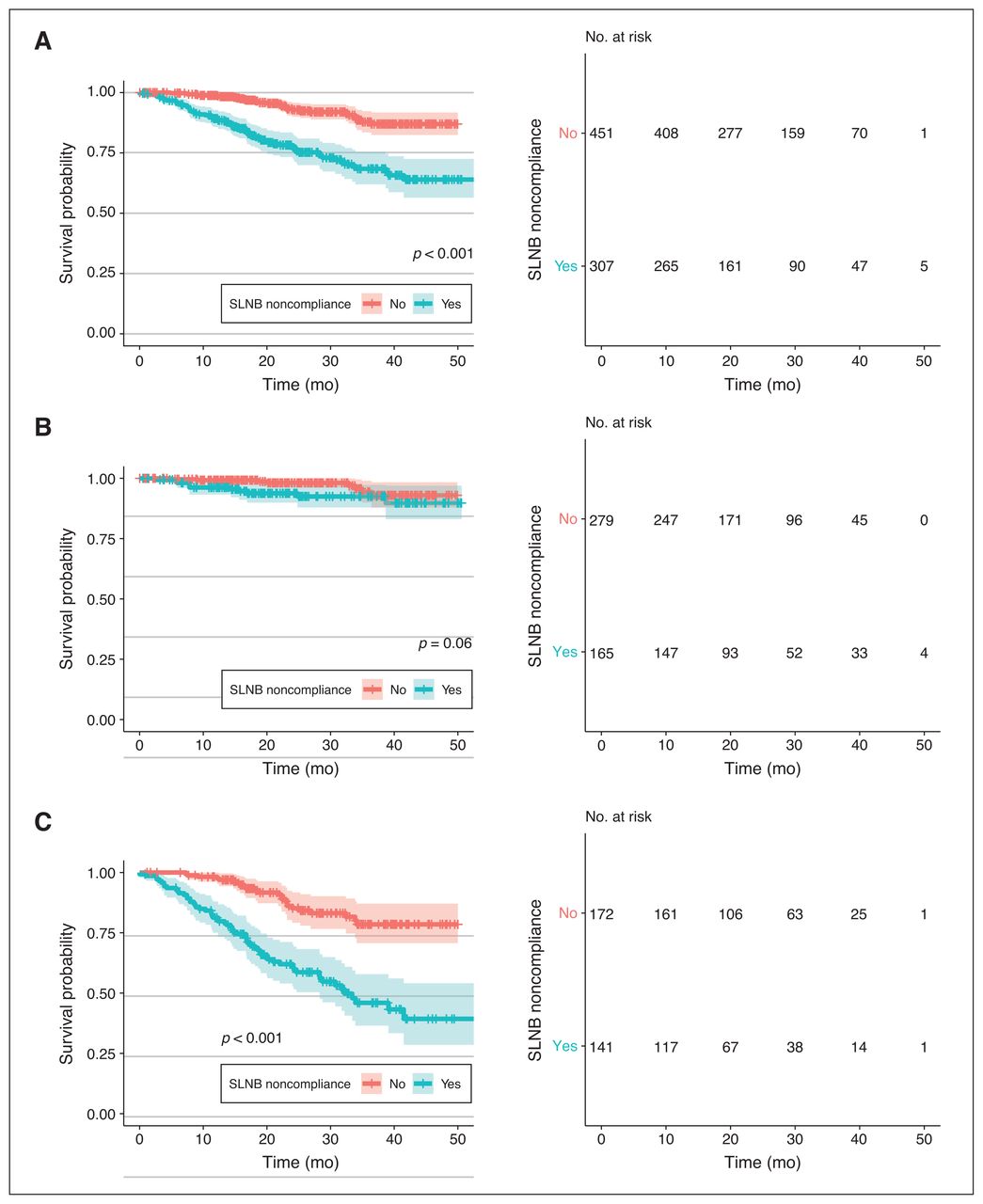
At last follow-up, 106 of 759 patients (14.0%) had died. Median survival was not reached at the time of analysis. Noncompliance with SLNB guidelines was associated with a significantly increased hazard for mortality (hazard ratio [HR] 3.742, 95% CI 2.471–5.666, p < 0.001) (Figure 2). This risk persisted when clinical stage I (HR 2.347, 95% CI 0.944–5.835, p = 0.033) and stage II (HR 3.818, 95% CI 2.381–6.120, p < 0.001) were separately analyzed.

Kaplan–Meier analysis for all patients based on noncompliance with SLNB guidelines. Analyses were performed for patients with melanoma at both stages I and II (A), stage I only (B) and stage II only (C). SLNB = sentinel lymph node biopsy.
Patients aged 75 years and younger
Excluding patients older than 75 years of age, at the time of last follow-up, 33 of 529 (6.2%) patients had died. Of those who died, 39.4% (13/33) did not undergo SLNB. Median survival was not reached at the time of analysis. Noncompliance with SLNB guidelines had no significant impact on survival in this group overall (HR 1.396, 95% CI 0.683–2.856, p = 0.18) nor when stratified by clinical stage (stage I HR 1.976, 95% CI 0.278–14.030, p = 0.25; stage II HR 1.611, 95% CI 0.724–3.588, p = 0.122) (Figure 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis for patients aged 75 years and younger based on noncompliance with SLNB guidelines. Analyses were performed for patients with melanoma at both stages I and II (A), stage I only (B) and stage II only (C). SLNB = sentinel lymph node biopsy.
Discussion
Nearly half of patients in this study did not undergo SLNB when it would be indicated on the basis of published international guidelines. This is concerning given the firmly established role of SLNB in the management of melanoma, including its implications for therapeutic decisions and the prognostic information it provides.9,10,25 Our findings are in keeping with those of previous studies that have shown that SLNB is underutilized.25,26
Our results demonstrate that certain groups are at especially high risk for noncompliance with SLNB recommendations and we identified both clinical and pathologic factors that predict the likelihood of undergoing SLNB. Patients with tumours on the head and neck were significantly less likely to undergo SLNB and only 33% of eligible patients with tumours in this region underwent SLNB. This is in keeping with the findings of previous studies and may suggest that a lack of familiarity with operating in the head and neck region may contribute to poor rates of SLNB.25,26,29 Patients with high-risk pathologic factors, including a mitotic rate of 1/mm2 or greater and an increased Breslow depth, were more likely to undergo SLNB. Previous studies have also found that adverse pathologic features affect the likelihood of undergoing SLNB.27,29 The increased likelihood of undergoing SLNB with Breslow depth greater than 1.0 mm may reflect the fact that performing SLNB in patients with clinical stage IB (T1b) melanoma is not clearly standard of care. The NCCN guidelines recommend that SLNB be considered for T1b melanoma, whereas SLNB is recommended for T2 melanoma.6 The rate of SLNB improved to 75% when patients with T1b melanoma were excluded. However, this still indicates that one-quarter of patients with higher-risk melanoma are being inadequately staged. Furthermore, only 35% of patients with clinical stage IIC underwent SLNB. This is particularly concerning given this is a high-risk group of patients with an estimated 30%–50% risk of nodal metastases.30 Given the important prognostic information and the implications for adjuvant systemic therapy for melanoma of clinical stage IB or greater, the underutilization of SLNB is problematic.9,10,23,31
Older patients have consistently been shown to be less likely to undergo SLNB.25–27,29,32 Our results further add to this evidence, with patients older than 75 years having an OR of 0.15 for undergoing SLNB. This may reflect a tendency toward less invasive procedures with advancing age and increased patient comorbidities, which was not captured in our study. Interestingly, 90% of this population still underwent a definitive WLE. While we recognize that SLNB is more invasive than a simple WLE, the decision to omit SLNB in this group to avoid the potential associated surgical complications must be balanced against the risk of nodal metastases, particularly if patients would be candidates for adjuvant systemic therapy. Finally, the rate of SLNB for patients aged 75 years and younger remains low (66.1%) and similar predictive factors for undergoing SLNB were identified on a subset analysis excluding patients older than 75 years. This suggests that advanced age alone does not explain lack of compliance with SLNB recommendations.
While this study did not demonstrate a difference in regional recurrence–based compliance with SLNB recommendations, there was a significantly higher risk of distant recurrence with noncompliance with SLNB recommendations. This highlights the importance SLNB plays in the early detection of clinically occult regional disease and the implications this may have for the prevention or early treatment of distant metastatic disease. The lack of impact of noncompliance on regional recurrence may be partially due to a relatively short duration of follow-up and the fact that regional recurrence can be difficult to capture. Noncompliance with SLNB recommendations appeared to increase the risk for mortality for the overall population, but this impact was not maintained when patients older than age 75 were excluded. This may suggest that noncompliance with SLNB has a greater impact on older patients, but it more likely reflects underlying comorbidities in this age group. The lack of impact on survival of younger patients may be partially explained by the fact that adjuvant immunotherapy and targeted therapy were not routinely being used in BC during the study period. The lack of survival benefit among patients aged 75 years and younger is in keeping with MSLT-1, which failed to show an impact of SLNB on OS.10 Even without a survival benefit, the importance of accurate nodal staging is highlighted by the substantially higher rates of both regional and distant recurrence among those with a positive SLNB.
The shift away from routine CLND in the setting of a positive SLNB coupled with a lack of survival benefit overall may cause some to argue that SLNB is not essential.10,13 However, the evolving role of systemic therapy provides renewed relevance to SLNB, and current guidelines emphasize the importance of SLNB in identifying patients who may benefit from adjuvant systemic therapy or enrolment in clinical trials.6,9,14,23 There are now several studies that provide strong evidence for improved outcomes with adjuvant systemic therapy for stage III melanoma. For example, at a median follow-up of 5.3 years the use of adjuvant ipilimumab compared with placebo in stage III melanoma resulted in improved RFS (40.8% v. 30.3%), DFMS (48.3% v. 38.9%) and OS (65.4% v. 54.4%).16 Patients treated with adjuvant pembrolizumab had improved RFS compared with those who received placebo at 12 months (75% v. 61%) and 18 months (71% v. 53%).17 Patients with BRAFV600-mutated resected stage III melanoma who were treated with adjuvant dabrafenib and trametinib had improved RFS compared with those who received placebo at 3 years (59% v. 40%) and 4 years (54% v. 38%). The BRIM8 trial showed that the use of adjuvant vemurafenib in select patients with resected stage IIC and III melanoma resulted in improved DFS in comparison with placebo.33 These studies provide a strong rationale for performing SLNB, as patients must be accurately staged to benefit from systemic therapy. As the treatment of melanoma continues to evolve, accurate staging is also imperative to identify opportunities for enrolment in clinical trials.9,14
Limitations
This study is limited by its retrospective nature and the possibility of patient exclusion or missing data. Information on patient comorbidities was not collected, which influences the clinical decision for SLNB. However, this is balanced by a large sample size and a comprehensive review of patients.
Conclusion
SLNB is being underutilized in BC. These results are highly relevant given the rapidly expanding role of adjuvant systemic therapy for high-risk patients in addition to the increased proportion of patients who should be considered for SLNB on the basis of the eighth edition of the AJCC Cancer Staging Manual and current guidelines. Efforts should be made to increase the use of SLNB in appropriate patients through physician and patient education and awareness.
Footnotes
Presented in part at the Canadian Surgery Forum, Sept. 5–7, 2019, Montréal, Que., and at the Canadian Society of Surgical Oncology Annual Meeting, May 3, 2019, Toronto, Ont.
Competing interests: None declared.
Contributors: S. Ollek, K. Taqi, L. Chen, N. Davis, T. Hamilton and H. Stuart conceived the study. S. Ollek, S. Minkova and M. Martinka acquired the data, which S. Ollek, S. Minkova, L. Chen, T. Hamilton and H. Stuart analyzed. S. Ollek, K. Taqi, L. Chen, T. Hamilton and H. Stuart wrote the article, which S. Minkova, L. Chen, M. Martinka, N. Davis, T. Hamilton and H. Stuart critically revised. All authors agreed to be accountable for all aspects of the work.
- Accepted April 7, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/