


Abstract
Background: In the setting of international disaster response, an important challenge is determining when it is appropriate to withdraw deployed assets as the acute disaster response transitions to recovery and rebuilding. We describe our experience with real-time data collection during our medical response to Typhoon Haiyan as a means to guide military aid mission parameters.
Methods: The operational medical headquarters prospectively developed a database for use in this mission. Mobile medical teams (MMTs) were deployed to provide primary care, and the nurse designated to each MMT was responsible for entering and transmitting data daily to the medical headquarters. Data collected included the MMT location, basic patient demographics, the primary reason for the encounter and any treatment provided. These encounters were then classified as disaster, acute or chronic.
Results: Between Nov. 16 and Dec. 16, 2013, medical care was provided to 6596 local nationals; 238 (3.6%) had disaster-related illness or injury, 4321 (65.5%) had acute postdisaster medical conditions and 2037 (30.9%) sought medical care for chronic conditions. Of the 257 patients with traumatic injuries, 28 (11%) had disaster-related injuries and 214 (83%) had acute injuries that occurred postdisaster.
Conclusion: The data collected during the mission to the Philippines was compiled with performance metrics from the other Disaster Assistance Response Team components to help advise the Canadian government regarding mission duration. We recommended that data collection continue on all future missions and be modified to provide further information to larger disaster coordination teams, such as the United Nations Office for the Coordination of Humanitarian Affairs.
International disaster response is a complex and challenging endeavour for both governmental and nongovernmental organizations to undertake. However, an often greater challenge is determining when it is appropriate to withdraw deployed assets as the acute disaster response transitions to recovery and rebuilding. This paper describes the feasibility of real-time data collection and analysis as a means to guide military aid mission parameters and facilitate collaborations with other civilian aid agencies to achieve rapid and targeted medical assistance.
On Nov. 8, 2013, Typhoon Haiyan (also known as “Yolanda”), one of the strongest typhoons on record, struck the central region of the Philippines. In addition to devastating infrastructure, property, power and communications, this Category 5 supertyphoon resulted in substantial losses of life and injury. As of Jan. 29, 2014, more than 6000 individuals were reported dead, 29 000 injured, and approximately 1800 still missing.1
As part of the response to this overwhelming humanitarian disaster, the Government of Canada rapidly made the decision to deploy the Canadian Armed Forces (CAF) Disaster Assistance Response Team (DART). This humanitarian mission was called Operation RENAISSANCE. The DART is a multidisciplinary military unit comprising headquarters, logistics, engineering, security and medical sections that can respond to natural disasters anywhere in the world in order to conduct emergency relief operations within 48 hours of being notified. Its responsibilities are to stabilize the primary effect of the disaster by providing medical care, clean water, infrastructure repair, security and prevention of secondary disaster effects, such as disease spread. The goal is to gain time for other organizations to prepare and deliver long-term recovery programs. Working with governmental and nongovernmental organizations, the DART serves 3 critical needs: production of safe drinking water, engineering aid and primary medical care.2 After an advance team comprising members from the CAF and Canadian government officials met with local officials in the Philippines, it was determined that the DART would be deployed to the city of Iloilo to provide relief to Panay Island.
The medical component of the DART comprises medical officers (physicians), physician assistants, nursing officers and medical technicians. Combined with a pharmacist, preventative medicine, laboratory and radiology technicians, this team of approximately 50 personnel provides a substantial and flexible primary care medical capability. The medical team is responsible for meeting the medical needs of the disaster-affected population as well as the DART itself. By providing primary care to the local population, one of the mission objectives of the DART medical component is to lessen the impact on local hospitals and medical facilities, thereby allowing these local resources to focus on the more seriously ill or injured individuals. The DART was able to begin providing patient care to this population on Nov. 16, 2013, 8 days after Typhoon Haiyan struck.3
In this paper, we describe the health care needs of the 6596 members of the local population treated by the medical section of the DART during their 1-month deployment to the Philippines after Typhoon Haiyan. By prospectively collecting data on the population treated, the CAF was able to acquire accurate data in a timely manner to document the nature of medical issues encountered and aid in the determination of optimal mission duration. This approach demonstrates the feasibility of real-time data collection as a means to guide military aid mission parameters and may be used in collaboration with other civilian aid agencies to achieve rapid and increasingly targeted medical assistance in future relief operations.
Methods
Operational structure
In planning the optimal approach to provide medical aid to Panay Island, the following factors were taken into account: 1) the availability of health care in urban centres remained similar to pre-typhoon levels; 2) there was a large geographic area requiring assistance; and 3) the socioeconomic status of the people most in need, combined with damage to infrastructure, resulted in their inability to travel to the urban centres for care. Therefore a decision was made to reconfigure the usual static format and deploy smaller, more agile teams, known as mobile medical teams (MMTs), which were able to provide primary care in an outreach format. Though the overall composition of the MMTs varied, each MMT included a family physician, a nurse and 2 medical technicians at a minimum. Originating from the centrally located headquarters in Roxas City, there was a maximum of 4 MMTs operating at 1 time. The MMTs would use either land or air transport to travel to affected areas and provide care for a predetermined timeframe, which was communicated in advance to the local population. All team members were stationed in Roxas City and departed to different locations based on guidance from the local health authority.
Data collection
As extensive data had not been collected on prior DART deployments, the operational medical headquarters prospectively developed a database for use in this mission using Microsoft Excel, version 14.3.8. Instructions on data field definitions were provided to the DART medical team on location in the Philippines. Data on patient encounters during a given MMT visit were collected from patient records. The nurse designated to each MMT was responsible for entering and transmitting data daily to the medical headquarters. We attempted to mitigate data heterogeneity by having the senior nursing officer review all data before final entry into the mission database. Any questions regarding patient classification were clarified with the medical officer or medical technician directly involved in that patient’s care at the time the data was entered into the database.
All infectious diagnoses were entered according to the system affected. The “health check” category was included, as locals presented to the MMT simply for a check-up, often never having encountered a health care professional before and not having a specific presenting complaint. If the patient presented with more than 1 symptom, the most acute diagnosis was entered into the database as the final diagnosis. All data entered into the database were stripped of individual patient identifiers and kept on secured hard drives.
Data collected included the MMT location, basic patient demographic characteristics and the primary reason for the encounter based on the patients’ chief complaint, along with any treatment provided. These encounters were then classified into 3 separate categories:
disaster (i.e., injury or illness that occurred as a direct result of the typhoon, such as cough or diarrhea in patients displaced by the typhoon and living in unsanitary conditions),
acute (injury or illness that was not directly attributable to the typhoon and whose onset was within 4 weeks of the patient encounter), or
chronic (injury or illness not directly related to the disaster that had been a concern for longer than 4 weeks).
Statistical analysis
All patients assessed by the DART MMTs were included in the data analysis. Members of the CAF or other Canadian government agencies who received care from the DART were excluded. Descriptive statistical analyses were used by the mission command as a metric to determine ongoing population health care needs.
Results
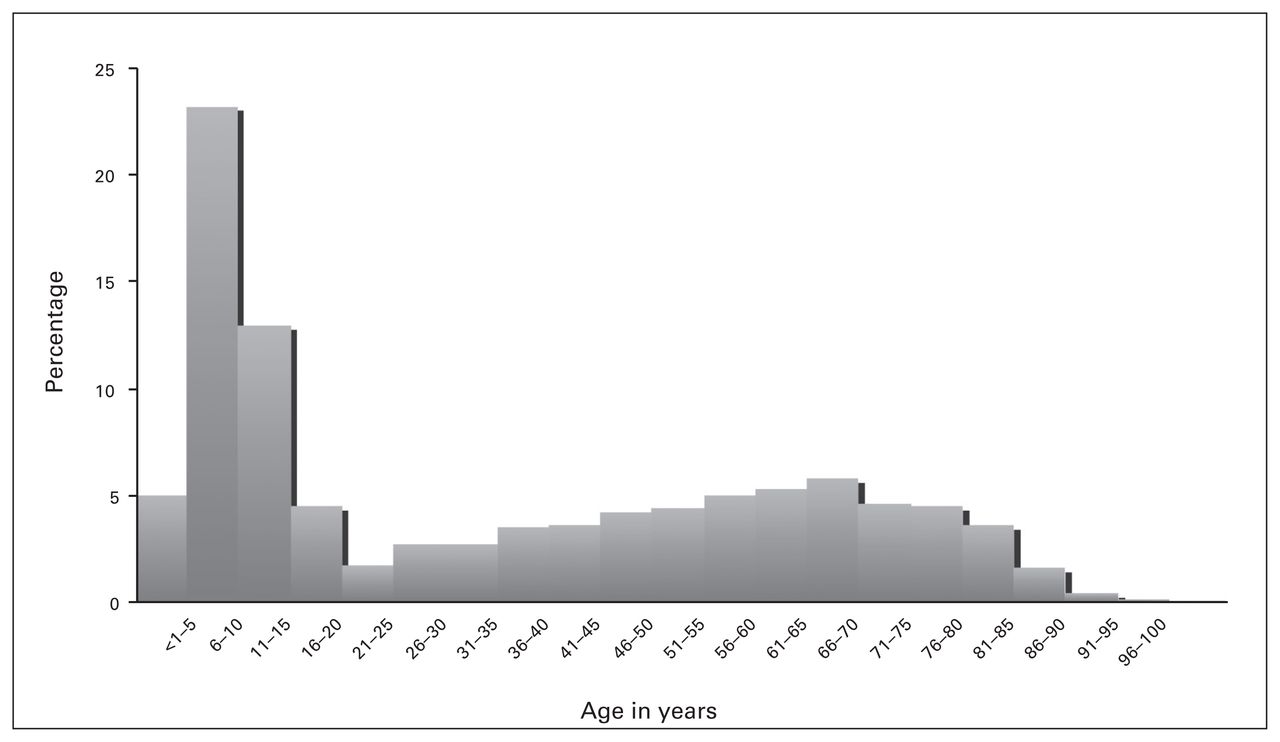
Between Nov. 16 and Dec. 16, 2013, medical care was provided to 6596 local nationals. Demographic data for the treated population are presented in Table 1. The patients’ age ranged from 2 weeks to 98 years. A substantial proportion of patients were children. Specifically, more than 40% of patients seen were younger than 10 years of age, and 28% of all patients seen were younger than 5 years (Fig. 1). Approximately 64% of patients were female and 36% were male. The DART MMTs treated between 65 and 345 patients per day. During the mission, MMTs visited 69 villages in 16 separate municipalities over an estimated area of 2700 km2 (Fig. 2).

Age distribution of local population patient encounters.
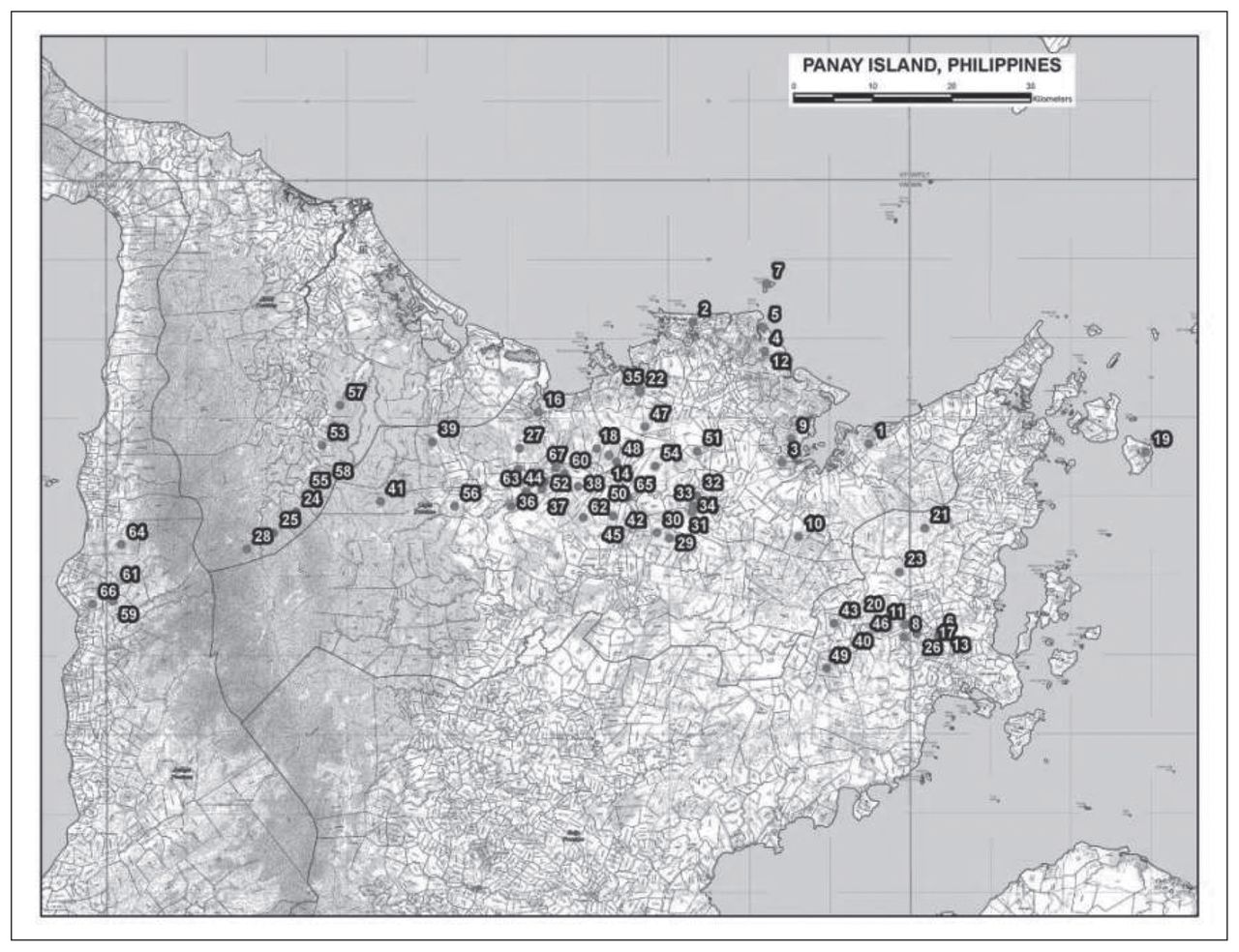
Sites of mobile medical team visits.
Demographic characteristics of local population seen by the CAF DART medical team, n = 6596
Table 2 demonstrates the incidence of primary diagnoses in each age group. It is notable that respiratory illness showed a strong predominance in the pediatric population; 70.9% of infants younger than 1 year of age and 61.8% of children between the ages of 1 and 5 years presented with respiratory illnesses. Gastrointestinal and dermatological illnesses were other important contributors in the pediatric burden of illness.
Diagnoses by system affected in each age group*
We next determined which diagnoses occurred most frequently in each of the disaster, acute and chronic categories (Table 3). Of the 6596 patients who were encountered during the mission, 238 patients (3.6%) suffered disaster-related illness or injury while 4321 patients (65.5%) had acute post-disaster medical conditions and 2037 patients (30.9%) sought medical care from the DART for chronic conditions.
Illness and Injury classification by category as attributable to the typhoon
Traumatic injury accounted for 3.9% of all patient encounters. Of the 257 patients treated for traumatic injuries, 28 (11%) had injuries classified as related directly to the disaster and 214 (83%) were considered to be acute injuries that occurred postdisaster. This finding may be attributable to the population having to live in the physically unsafe posttyphoon destruction and sustaining secondary injuries. Of interest, 8% of all disaster-related illnesses were psychiatric in nature, with patients experiencing symptoms of anxiety or insomnia after the devastation of the typhoon. This group constituted 43% of all psychiatric complaints encountered during the mission. As mentioned, a substantial proportion of the patient population sought medical attention from the MMTs for chronic health problems. For example, 50% of musculoskeletal and more than 60% of cardiovascular diagnoses were determined to be of a chronic nature.
The number of disaster-related patient encounters was relatively stable throughout the deployment at 2%–3% of all patient encounters per day, with increases seen at day 16 (26.5%) and day 23 (11.1%) postdisaster (Fig. 3). These increases corresponded with targeted visits to villages in Sara after information was obtained during the operation that these areas were particularly affected by the typhoon. At day 31 posttyphoon the MMTs started to encounter a slight predominance of chronic conditions compared with acute medical issues that recurred at days 34 and 38 posttyphoon.
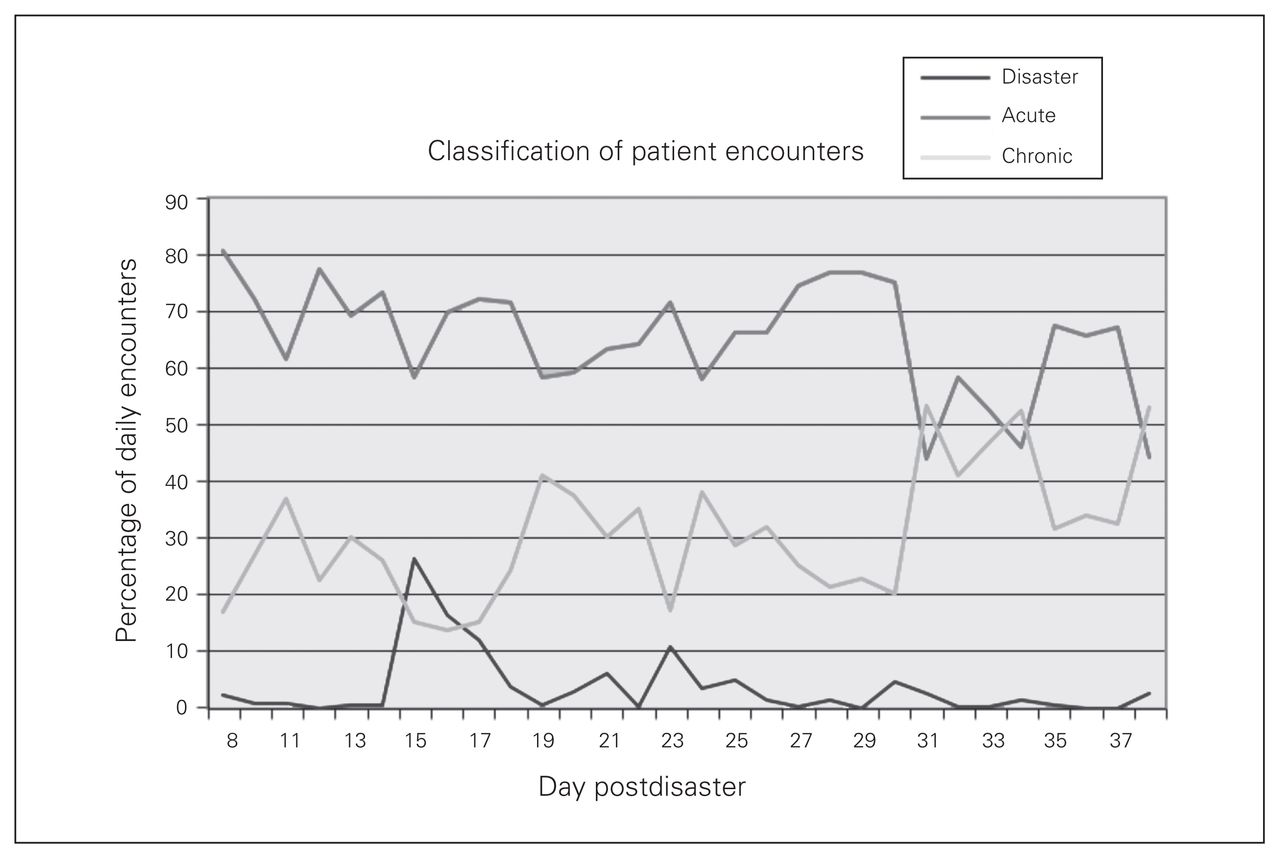
Classification of daily patient encounters by disaster, acute and chronic categories. Disaster refers to an injury or illness that occurred as a direct result of the typhoon. Acute refers to injuries or illnesses that were not directly attributable to the typhoon and had an onset within 4 weeks of the patient encounter. Chronic refers to an injury or illness not directly related to the disaster that had been a concern for longer than 4 weeks.
Discussion
The medical component of the DART was able to commence providing care in the Philippines within 8 days of the destruction caused by Typhoon Haiyan. The standard practice in previous DART missions was to establish a single static site for the delivery of medical aid to the affected population with occasional mobile teams. This mission was the first time that the DART medical component delivered all medical care to the local population in a mobile format. This was advantageous as it permitted care to be delivered to many isolated villages across a sizeable geographic area; however, it limited the volume of patients that could be seen in 1 day and also the ability of clinicians to follow up with patients and monitor clinical response to treatment.
Though patients in the extremes of age were encountered, almost 50% were younger than 20 years and 40% were younger than 10 years. The finding of such a high prevalence of the children within the patient population suggests that disaster response elements should be appropriately prepared to care for a high pediatric patient burden. This reinforces the current level of pediatric training the DART medical team receives prior to deployment.
Disaster-related illness and injuries represented approximately 4% of all patient encounters, with an increase in more severely affected areas, such as the village of Sara, to 26.5%. Overall, respiratory, gastrointestinal, dermatological and MSK diagnoses were the most common classifications of illness and injury among the entire patient population. The majority of patient presentations were for health issues that could be managed by the primary care providers in the DART MMT. This finding is consistent with those of other studies that have demonstrated that a significant primary health care burden follows the onset of humanitarian disaster crises.4,5 The MMTs saw only 11.8% disaster-related trauma, which may have been specific to Panay Island. Though psychiatric diagnoses were a moderate contributor to the disaster-related illness burden, they may have been underrepresented. It is possible that patients who presented with vague somatic complaints may have had an underlying psychiatric illness related to the disaster. Though all of the patients seen could be managed at the primary care level by the medical officers present, the literature surrounding the need for specific mental health providers is mixed. Certain studies of previous disasters have found that most acute mental health symptoms are self-limited,5–8 while other studies state that there is a justifiable need to include them.7
The use of prospective, detailed data collection was also a novel approach as prior DART missions exclusively reported the numbers of patients seen per day. The purpose of data collection was to provide daily information regarding the percentage of disaster, acute nondisaster and chronic cases seen by the MMTs to the operational headquarters. This information was compiled with performance metrics from the other DART components to help advise the Canadian government regarding mission duration. However, throughout the mission it was also identified that the data collection could be prospectively transmitted by the MMTs to the United Nations Office for the Coordination of Humanitarian Affairs (UN OCHA) cluster meetings. Data collection could also confirm when the MMTs had reached an area that was substantially affected by the disaster and indicate when disaster-related illnesses and injuries no longer represented a considerable burden of illness in that particular area. The data were also analyzed retrospectively to drive changes to the composition of future medical teams, their training and equipment.
Limitations
Though it is recognized that data collected during disasters can drive the disaster response,4 data collection during a relief mission is technically challenging.9 As this was the first attempt at prospective data collection for the DART, there were clinical parameters that were not included that would have been beneficial; for example, the monitoring of infectious diseases so that outbreaks could be identified early. Future missions using this approach would benefit from being able to capture data on infectious disease diagnoses that could be transmitted to UN OCHA and World Health Organization cluster meetings.
Conclusion
Within 8 days of the destructive effects of Typhoon Haiyan on the Philippines, the CAF DART’s medical component was able to deliver primary health care to the local population of Panay Island. This was accomplished using mobile multidisciplinary health care teams, which allowed care to be provided to more than 60 villages and more than 6000 local patients.
For the first time, the DART prospectively collected epidemiological and clinical data from patient encounters, which helped the Canadian government to determine optimal mission duration. It is recommended that data collection continue on all future missions and be modified to provide further information to larger disaster coordination teams, such as the UN OCHA.
Footnotes
Competing interests: None declared.
Contributors: E. Savage and D. Pannell designed the study. E. Savage, S. Smith and D. Pannell acquired the data, which all authors analyzed. E. Savage, S. Smith and D. Pannell wrote the article, which all authors reviewed and approved for publication.
- Accepted February 23, 2015.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.