


Abstract
Background: The shape of the association between preoperative hemoglobin level and outcomes after primary arthroplasty has not been adequately described. This study aimed to characterize the association between preoperative hemoglobin level and important outcomes after primary hip and knee arthroplasty and how this association is influenced by other key confounders.
Methods: Using de-identified, population-based health administrative data for Ontario housed at ICES, we identified all primary hip and knee arthroplasty procedures performed in Ontario between April 2007 and March 2017. Preoperative hemoglobin level, age, sex, Charlson Comorbidity Index score, American Society of Anesthesiologists score, preadmission living status, Hospital-patient One-year Mortality Risk (HOMR) score, and serum sodium and creatinine levels were extracted. All relevant postoperative outcomes that could be measured accurately were identified. We performed multivariable logistic regression and restricted cubic splines analyses.
Results: A total of 188 176 patients clustered within 532 surgeons were studied. The adjusted likelihood of transfusion increased notably and progressively when the preoperative hemoglobin level was below 135 g/L; duration of surgery, patient age and HOMR score amplified this association. Risk of postoperative admission to critical care showed a linear association with preoperative hemoglobin level. Risks of unplanned 30-day emergency department visit, 30-day readmission and 1-year all-cause mortality showed curvilinear associations with baseline hemoglobin level, with risks being notably greater as the level deviated from 137 g/L to 141 g/L.
Conclusion: Preoperative hemoglobin levels, both high and low, were independently significantly associated with primary arthroplasty outcomes, and levels at which outcome risks started to increase exceeded threshold values commonly used to define “normal.” Preoperative hemoglobin level should be considered in future bundled payment models that aim to account for case-mix when grading postarthroplasty outcomes.
Rates of primary hip and knee arthroplasty are increasing continually; more than 1.4 million primary joint replacement operations were performed in North America in 2019 alone.1,2 Although advancement in the performance of these procedures has occurred,3 the incidence of peroperative complications remains consequential, varying between 6% and 19%.4,5 Preoperative patient optimization may improve the body’s “reserve” and ability to recover after surgery.
Hemoglobin level is a modifiable preoperative factor that is immediately relevant to arthroplasty. Preoperative anemia is relatively common, with a documented prevalence of 21%–35% that has remained unchanged over the years.6,7 Furthermore, arthroplasty is associated with considerable blood loss, even with contemporary preventive measures in place.8–12 As a result, more than 90% of patients are anemic after arthroplasty.13,14
Anemia before arthroplasty has been associated with increased transfusion risk,13,15,16 morbidity, mortality and length of stay.4,5,17–26 However, these associations have been analyzed almost exclusively after categorization of preoperative hemoglobin levels (i.e., grouping patients with or without anemia, however defined). Categorization of continuous variables decreases the power of analyses to identify associations substantially and leads to information loss.27
In addition, the shape of the association between preoperative hemoglobin level and outcomes has not been adequately described. For example, it is unclear whether supranormal hemoglobin levels (i.e., polycythemia) are protective (as they could reduce transfusion risk) or a potential risk factor (owing to a possibly increased risk of venous thromboembolism). Therefore, analyzing the continuous, but possibly nonlinear, association of preoperative hemoglobin level with outcomes could help to identify levels at which outcome risks threaten the procedure’s utility, as well as identify patients in need of hematologic optimization. Furthermore, to our knowledge, the influence of other factors on the association between preoperative hemoglobin level and outcome has not been examined to any substantial degree.
The aims of this population-based study were to characterize the association between hemoglobin level and a number of outcomes — red cell transfusion, postoperative admission to a critical care unit, unplanned 30-day emergency department visit, unplanned 30-day hospital readmission and 1-yr all-cause mortality — after primary arthroplasty and describe the characteristics of the association; and test for any interactions of this association with other key confounders influencing outcome.
Methods
Study design and data sources
This was a retrospective cohort study using de-identified, population-based health administrative data for Ontario, Canada, housed at ICES, a publicly funded, independent research organization. The following data sets were linked deterministically by means of encrypted patient health card numbers in order to obtain the information necessary for this study: Discharge Abstract Database, Ontario Laboratory Information System (OLIS), Registered Persons Database, National Ambulatory Care Reporting System, Ontario Health Insurance Plan and Continuing Care Reporting System (Appendix 1, available at www.canjsurg.ca/lookup/doi/10.1503/cjs.020720/tab-related-content). The study was approved by ICES and was legally exempt from research ethics board review owing to the de-identified nature of the data.
Study cohort
We searched the Discharge Abstract Database from Apr. 1, 2007, to Mar. 31, 2017, to identify all elective admissions with total hip arthroplasty (Canadian Classification of Health Intervention codes 1VA53LAPN and 1VA53PNPN), including resurfacing arthroplasty, and total knee arthroplasty (Canadian Classification of Health Intervention codes starting with 1VG53) as the primary procedure. We linked to OLIS to identify all hemoglobin tests conducted in these patients; patients with no hemoglobin measured in the year before arthroplasty were excluded. To ensure that the unit of analysis was the patient, we limited inclusion to the first procedure meeting the inclusion criteria during the study period for individual patients and excluded patients who had undergone arthroplasty in the 6 months before their index procedure. We included the latter exclusion criterion since recent surgery is associated with anemia13,14 and leads to selection bias.
Hemoglobin level
We identified all hemoglobin measures for each patient in the year before his or her operation from OLIS. We recorded the final preoperative hemoglobin level and the number of days before the operation that it was measured.
Outcomes
We identified all relevant postoperative outcomes that we could measure accurately using our data;28 we did not prioritize these outcomes (i.e., none was nominally chosen as the “primary outcome”). In-hospital outcomes included transfusion of packed red cells and transfer to a critical care unit. Postdischarge outcomes included unplanned emergency department visits and hospital readmissions within 30 days of discharge from hospital, and death from any cause within 1 year of surgery. We chose the 30-day period since this is typical of the literature on readmission.18 We identified all outcomes before analyzing the data.
Covariables
We determined patient age, sex, year of surgery, Charlson Comorbidity Index score29 (using a 1-year look-back period with comorbidity coding criteria from Quan and colleagues30 and score weights from Schneeweiss and colleagues31), number of hospital admissions in the previous year and procedure factors (laterality, anesthetic technique and operation duration) from the Discharge Abstract Database. We retrieved each patient’s serum sodium and creatinine levels closest in time to his or her operation from OLIS because a significant association between hyponatremia32–37 and decreased renal function38 and mortality has been described. We determined the American Society of Anesthesiologists Physical Status score from Ontario Health Insurance Plan data.39 We determined preadmission living status (independent, inpatient rehabilitation, home care, nursing home [i.e., long-term care institution] or chronic care hospital [i.e., complex continuing care]) from the Continuing Care Reporting System. We determined death risk using the Hospital-patient One-year Mortality Risk (HOMR) score. This model combines values for 12 covariables regarding patient demographic characteristics, health burden and acuity of illness to create a score that is highly discriminative (C-statistic 0.89) and well calibrated for 1-year all-cause death risk.40 It has been validated externally with administrative data41 and primary data.42
Statistical analysis
We used SAS 9.4 (SAS Institute) for all analyses. We used multivariable logistic regression accounting for the clustering of patients within surgeon to model the independent association of each covariable with each outcome (PROC GLIMMIX). In this generalized linear mixed model, the surgeon was treated as the random-effects term, and all other factors were treated as fixed effects. We reasoned that several of the outcomes — notably receipt of transfusion and critical care use — might be strongly dependent on surgeon-specific practice patterns; as such, accounting for these issues by clustering patients within surgeon could explain much variation in the data.
Before analyzing the data, we specified all covariables to be included in the models; no post hoc or variable selection based on inferential testing was used. All continuous variables were centred before modelling. Those included age, sex, HOMR score, sodium level, baseline estimated glomerular filtration rate, type of procedure (hip or knee), American Society of Anesthesiologists score, type of anesthetic (spinal, general, combined or other), laterality (unilateral or bilateral) of procedure and duration of surgery. For patients with missing sodium or serum creatinine levels, we imputed median values of the cohort, since this returns results that are less biased than if normal values are used for simple imputation.43 We converted serum creatinine values to a baseline estimated glomerular filtration rate using the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation.44 We used restricted cubic splines to model the independent association of all continuous variables (including their interactions) with each outcome using 5 knots for all variables except those with restricted distributions, including sodium (3 knots) and the interaction between hemoglobin with arthroplasty type (3 knots) and with patient sex (2 knots). We used restricted cubic splines because the main effect estimate is continuous and we wanted to identify any potential nonlinear relations present.
Results
We identified 364 480 elective hospital admissions between Apr. 1, 2007, and Mar. 31, 2017, in which total hip or knee arthroplasty was coded as the primary procedure. Of the 364 480 patients, 131 932 were excluded because no preoperative hemoglobin value had been registered in OLIS, 43 004 were excluded because the patient was already included in the study, and 1368 were excluded because they had undergone arthroplasty within the previous 6 months. The remaining 188 176 patients, clustered within 532 surgeons (median number of patients per surgeon 176.5, interquartile range 2.5–616), formed the study’s cohort. The proportion of arthroplasty procedures excluded because of lack of a hemoglobin value in OLIS varied substantially over time owing to temporal changes in OLIS coverage (77.3% in 2008 v. 8.8% in 2016).
The cohort basic demographic characteristics are presented in Table 1. Almost two-thirds of operations (120 273 [63.9%]) were knee arthroplasty procedures. Patients were upper-middle-aged (mean age 67.8 yr [standard deviation 10.2 yr]) and predominantly female (112 009 [59.5%]). The mean hemoglobin level was 136.2 g/L (standard deviation 14.2 g/L). Most patients (96 228 [51.1%]) had their preoperative hemoglobin level measured within a month of undergoing primary arthroplasty. Spinal anesthesia was the most common anesthetic technique (148 942 procedures [79.2%]). Operations lasted a median of 1.75 hours, and patients remained in hospital a median of 3 days. Death in hospital was rare (245 patients [0.1%]); the risk was significantly higher with hip arthroplasty (114/67 903 [0.2%]) than with knee arthroplasty (131/120 273 [0.1%]) (χ2 = 11.6, p < 0.001).
Characteristics of patients who underwent primary hip or knee arthroplasty in Ontario, Apr. 1, 2007, to Mar. 31, 2017
The findings of the logistic regression models, including the performance of the model, are summarized in Table 2. After adjustment for all other covariates in the model, there was no independent association of year and type of anesthesia with outcome for any of the variables. A more detailed presentation of the performance is provided in Appendix 1.
Summary of logistic regression models for all outcomes*
Outcomes
Red cell transfusion
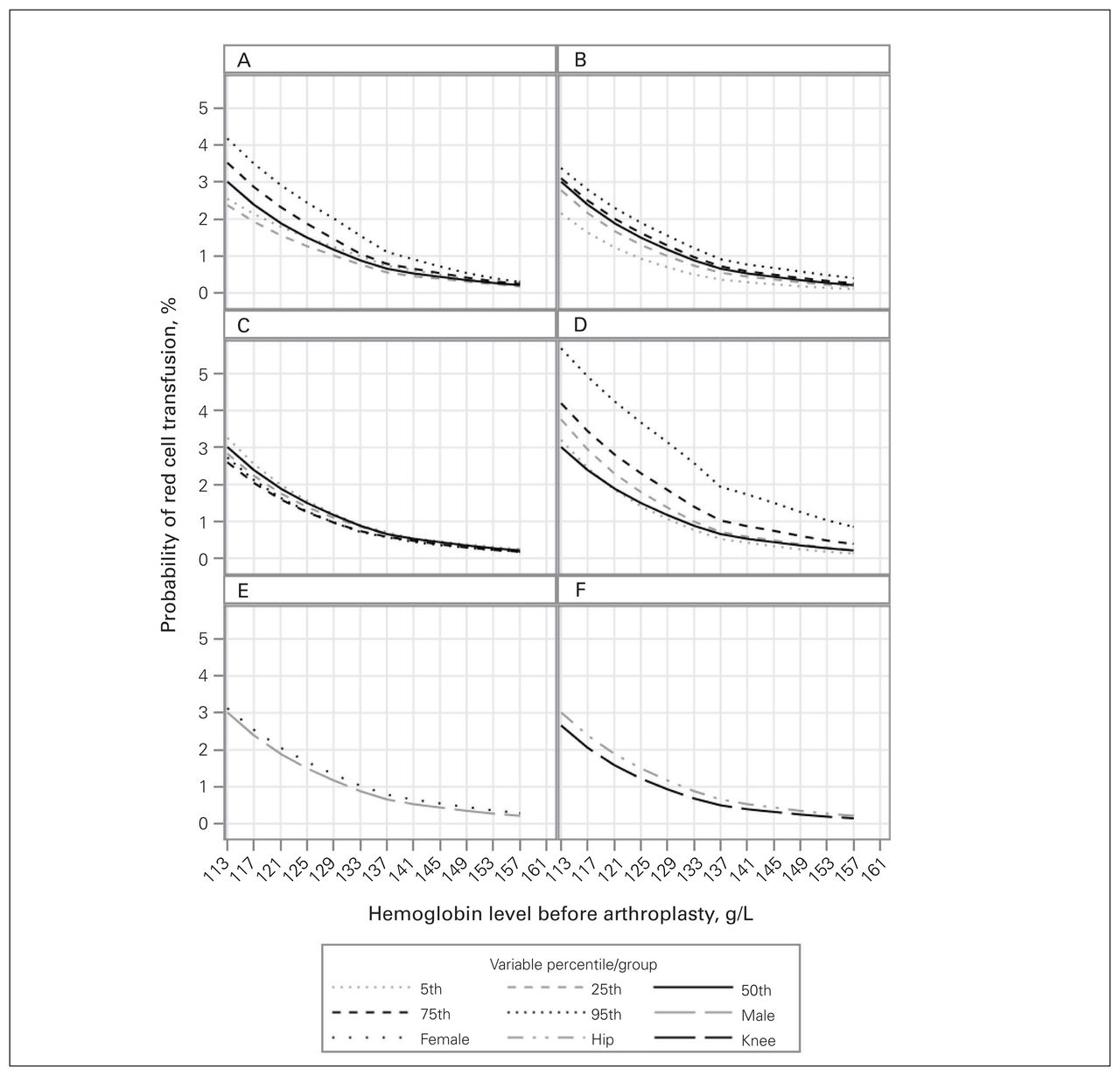
The adjusted likelihood of transfusion was strongly associated with preoperative hemoglobin level, increasing notably and progressively when the level fell below 135 g/L (Figure 1). Factors exaggerating this association included duration of surgery, patient age and HOMR score. At higher baseline hemoglobin levels, transfusion was significantly more likely with longer procedures; however, this progressive pattern diminished as baseline hemoglobin values decreased owing to the strong interaction term between hemoglobin value and duration of surgery (Table 2).

Association between preoperative hemoglobin level and probability of red cell transfusion by age (A), Hospital-patient One-year Mortality Risk score (B), estimated glomerular filtration rate (C), duration of surgery (D), sex (E) and joint (F). Percentile values for each continuous variable are presented in Appendix 1, Table S1. All results are adjusted for the covariables presented in Table 2.
Postoperative critical care
The likelihood of postoperative admission to a critical care unit increased significantly as baseline hemoglobin level decreased (Figure 2). Critical care admission was notably more likely in younger patients and in those with higher HOMR scores, a feature especially notable at lower hemoglobin levels (Table 2); however, the degree of association was similar for the different age and HOMR score percentiles.

Association between preoperative hemoglobin level and probability of postoperative admission to a critical care unit by age (A), Hospital-patient One-year Mortality Risk score (B), estimated glomerular filtration rate (C), duration of surgery (D), sex (E) and joint (F). All results are adjusted for the covariables presented in Table 2.
Unplanned 30-day emergency department visit
Baseline hemoglobin level was independently associated with the risk of an unplanned 30-day emergency department visit (Table 2), with a notable concave-up formation; its nadir occurred at hemoglobin levels around 140 g/L and increased at levels both above and below (Figure 3). This association was not importantly influenced by the other covariables (Table 2).

Association between preoperative hemoglobin level and probability of unplanned 30-day emergency department visit by age (A), Hospital-patient One-year Mortality Risk score (B), estimated glomerular filtration rate (C), duration of surgery (D), sex (E) and joint (F). All results are adjusted for the covariables presented in Table 2.
Unplanned 30-day hospital readmission
The risk of unplanned 30-day hospital readmission had a curvilinear relation with baseline hemoglobin being notably more likely as baseline hemoglobin levels deviated from normal (Figure 4). The association between hemoglobin values and readmission risk did not vary notably with other covariables; however, the degree of association was greater as HOMR score increased, in male patients and in knee arthroplasty.

Association between preoperative hemoglobin level and probability of unplanned 30-day hospital readmission by age (A), Hospital-patient One-year Mortality Risk score (B), estimated glomerular filtration rate (C), duration of surgery (D), sex (E) and joint (F). All results are adjusted for the covariables presented in Table 2.
One-year all-cause mortality
Baseline hemoglobin level was strongly associated with the risk of 1-year all-cause mortality (Table 2), also with a distinct curvilinear pattern (Figure 5). This risk was not modulated notably by the other covariables (Table 2). The risk of death was most strongly associated with HOMR score.

Association between preoperative hemoglobin level and probability of 1-year all-cause mortality by age (A), Hospital-patient One-year Mortality Risk score (B), estimated glomerular filtration rate (C), duration of surgery (D), sex (E) and joint (F). All results are adjusted for the covariables presented in Table 2.
Discussion
In this retrospective population-based study of more than 188 000 patients who underwent primary arthroplasty, we found that preoperative hemoglobin levels, both high and low, were significantly associated with important outcomes after primary arthroplasty. After adjustment for key confounders, preoperative hemoglobin level was associated with the risk of red cell transfusion, postoperative critical care admission, unplanned 30-day emergency department visit, unplanned 30-day hospital readmission and 1-year all-cause mortality. Furthermore, we found that preoperative hemoglobin values at which outcome risks started to increase exceeded threshold values commonly used to define “normal” hemoglobin levels. We also found that an elevated preoperative hemoglobin level was associated with increased risk of postdischarge complications.
Based on these findings, we suggest that preoperative hemoglobin level can be a reliable patient risk stratification tool. Considering that the risk of red cell transfusion was notably low when the preoperative hemoglobin value exceeded 135 g/L, we recommend that type and cross matching may not be indicated in such patients, especially when surgery is not expected to be complex. Given the significant association of hemoglobin level with all postoperative outcomes measured in this study, preoperative hemoglobin level should be considered in future bundled payment models that aim to account for case-mix when grading postarthroplasty outcomes.
In contrast to most previous analyses of the association between preoperative hemoglobin value and arthroplasty outcomes (Table 3), we did not categorize hemoglobin values. This allowed us to identify novel, distinct nonlinear associations between preoperative hemoglobin value and postoperative complications. We found that the odds of transfusion flattened notably when the level was above 135 g/L, an association that was consistent across all values of important confounders. This inflection point for transfusion was seen for both sexes. The World Health Organization classifies anemia based on sex,45 whereas international consensus experts recommend that hemoglobin values be considered independently of sex;46 our findings support the latter. Furthermore, the data suggest that the approach to preoperative hemoglobin testing and optimization could be stratified at 135 g/L (a value higher than typically considered a “normal” threshold) and that, in some cases, type and cross may not be required above this threshold.
Summary of previous studies examining association of hemoglobin level with outcomes after arthroplasty
We also found robust nonlinear associations between hemoglobin level and postdischarge complications. Unplanned 30-day emergency department visit, unplanned 30-day hospital readmission and 1-year all-cause mortality all showed a U-sshaped association, with the lowest probability of adverse outcome approximating 135–140 g/L. Although this finding may have been confounded by causes of chronic hypoxemia (such as smoking, obstructive sleep apnea or obesity hypoventilation syndrome) that can lead to both polycythemia and increased adverse outcomes after discharge, critical care use was not increased in the setting of higher hemoglobin values. With sleep apnea and hypoventilation, one would expect a similar causal pathway to exist between early in-hospital adverse events and longer-term adverse events. Future prospective research with detailed measurement of these risk factors is required. In the interim, these findings highlight to clinicians that supranormal hemoglobin values may necessitate a review of underlying risk factors; to researchers the importance of avoiding the categorization of continuous variables in analysis to identify nonlinear associations and maximize power;47 and to administrators and payers that, as payment models across the United States and Canada have shifted toward bundle payment,48 these results suggest that preoperative hemoglobin values should be considered for case-mix adjustment in future bundle models.
Limitations
Several potential weaknesses should be kept in mind when interpreting the study’s results. First, the study was capable of measuring the association between hemoglobin level and various outcomes in patients undergoing hip and knee arthroplasty, but not causation. This issue regarding association versus causation is key since it would influence any effect that preoperative hemoglobin optimization could have on postoperative outcomes. Second, comorbidities in this cohort, as gauged by the Charlson Comorbidity Index score, were notably low;29 this may have been due to comorbidity undercounting by administrative data codes.49 This is especially relevant in our population, since less than 5% of patients had been admitted to hospital in the previous year, which means that comorbidities had to have been coded at the time of the elective procedure in order to have been counted for the study.
Third, the external generalizability of the results remains to be tested in future studies using other population-based databases. However, findings from other studies reporting on arthroplasty outcomes from ICES2,50 are compatible with studies of North American, European and Austral-Asian cohorts.5,18,51,52 Fourth, the ICES data do not accurately capture medications given to patients during the hospital stay (or peroperatively). Thus, we could not accurately test the effect of the introduction of tranexamic acid use in arthroplasty procedures in this cohort. However, it is of interest that year of surgery over the study period (which includes the introduction of tranexamic acid into routine use in arthroplasty [2012–2014]) did not influence outcome after other covariables were accounted for.
Last, a substantial part of our cohort was excluded owing to missing hemoglobin levels in OLIS. Patient loss owing to lack of coverage from OLIS can be classified as missing completely at random since it is primarily due to patient location (i.e., whether or not the laboratory at which patients had any preoperative laboratory testing was captured in OLIS). Since outcomes (namely, patient survival) in hip and knee arthroplasty are extremely homogeneous throughout Ontario,53 the risk of systemic bias due to this issue is minimal.
Conclusion
Preoperative hemoglobin level was independently associated with risk of red cell transfusion, postoperative critical care admission, unplanned 30-day emergency department visit, unplanned 30-day hospital readmission and 1-year all-cause mortality after hip and knee arthroplasty. These associations were frequently nonlinear. Hemoglobin levels below 135 g/L were associated with a notable and progressive increased risk of requiring a blood transfusion peroperatively. This finding could act as a patient risk stratification tool and should be considered when devising algorithms to account for case-mix in bundle payment allowances.
Footnotes
Competing interests: George Grammatopoulos reports consulting fees from Formus Labs, outside the submitted work. Paul Beaulé reports grants from Zimmer Biomet and DePuy Synthes/Johnson & Johnson, and personal fees from MicroPort, MatOrtho, Zimmer Biomet, Medacta and Corin, outside the submitted work. No other competing interests were declared.
Contributors: All authors designed the study, acquired and analyzed the data, wrote and critically revised the manuscript, and gave final approval of the article to be published.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
- Accepted February 4, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.