


Abstract
Objective: To determine whether complete resection of small-bowel metastases from melanoma improves patient survival.
Design: A computer-aided chart review.
Setting: Hospitals associated with McGill University.
Patients: Twenty patients (17 men, 3 women), identified from 1524 patients with melanoma, who underwent surgery to the small bowel for metastases. Patient age and clinical presentation, tumour site and stage were recorded.
Intervention: Exploratory laparotomy with complete or partial resection of involved small bowel.
Main Outcome Measures: Operative morbidity, mortality and length of survival related to the extent of small-bowel resection.
Results: Eleven patients had complete resection, 8 patients had partial resection and 1 patient had a palliative bypass only. Long-term survival (ranging from 2 to 10 years) was 36% in those who had complete resection and 0% in those who had partial resection; operative morbidity and mortality were 20% and 15% respectively.
Conclusion: Complete resection of small-bowel metastases in patients with metastatic melanoma can result in long-term survival.
Melanoma is an unpredictable tumour that may metastasize to any organ in the body. It has an unusual predilection for the gastrointestinal tract, particularly the small bowel, and is the most common cause of malignant intussusception in adults. Intestinal metastases are reported in 50% to 60% of cases in autopsy series but are diagnosed before death in only 1% to 4% of patients.1
The role of surgery to achieve long-term survival in these patients is not well established and is generally viewed with scepticism. We present our experience with melanoma metastatic to the small bowel and identify the clinical, radiologic and pathological features. We studied the mortality and morbidity of surgical intervention to see if long-term survival could be achieved by complete resection of involved small bowel.
Patients and method
Between 1970 and 1994, malignant melanoma was diagnosed in 1524 patients at McGill University-affiliated hospitals. A computer-aided chart review identified 20 patients (17 men, 3 women) who had surgical intervention for melanoma metastatic to the small bowel. Data on patient age and clinical presentation and tumour site, stage and diagnosis were collected. The TNM classification of the American Joint Committee on Cancer was used for staging of the primary lesion.2 The surgical procedures were documented, and the available pathological slides were reviewed to confirm the original diagnosis. Postoperative outcome was analysed, and the Kaplan–Meier method was used to construct actuarial survival curves. The log-rank test was used to test significance of discrete variables on survival.
Findings
At the time of the initial diagnosis the mean age of the 20 patients was 48.4 years (range from 26 to 78 years). At the time of intestinal involvement the mean age was 52.4 years (range from 28 to 84 years).
Two patients were found to have small-bowel metastases at the time their primary cutaneous lesions were identified. In the remaining 18 patients the mean time interval between diagnosis of the primary disease and the appearance of metastatic disease was 4.4 years (range from 1.8 to 14.7 years).
The primary lesions were stage I in 1 patient, stage II in 2 patients, stage III in 10 patients and stage IV in 7 patients. The sites of the primary lesions included the trunk in nine patients, the head and neck in six patients and the extremities in three patients; two patients presented with metastatic lymphadenopathy with unknown primary site. The sites of metastases in the stage IV patients included lung, liver, brain and distant subcutaneous sites. For the 17 patients in whom the Clark level of invasion3 of the melanoma was known, one tumour was level I, four were level II, six were level III and six were level IV.
Symptoms were variable and nonspecific, but pain and vomiting were the most frequent, followed by rectal bleeding, fatigue and weight loss. The commonest clinical presentation was intestinal obstruction (10 patients), followed by gastrointestinal bleeding (7 patients). Obstruction was secondary to intussusception in seven patients and was associated with rectal bleeding in four of them. Four patients had peritonitis due to bowel perforation by the tumour. A palpable mass was detected on physical examination in four patients.
In six patients surgical exploration was based only on clinical findings and an abdominal series showing free air or complete small-bowel obstruction. Eight patients underwent an upper gastrointestinal series or enteroclysis: small-bowel dilatation, intraluminal filling defects and the spring-coil appearance characteristic of small-bowel intussusception were found. Computed tomography, done in two cases, demonstrated extraintestinal metastases and a mass representing the intussuscepted bowel. In two patients who presented with lower gastrointestinal bleeding of unknown etiology, surgical exploration was based on a positive angiogram in one patient and a positive nuclear scan in the other.
The most common site of involvement was the jejunum (80%), with 10 patients having isolated jejunal lesions and 6 patients having combined jejunal and ileal lesions. The lesions were almost invariably in the proximal segment of the jejunum and the distal segment of the ileum. Three patients had isolated ileal metastases, and one patient had a duodenal lesion. The lesions were multiple in 15 patients; both the mesentery and omentum were involved in 11 patients, whereas multiple segments of the small bowel were involved in 4 patients.
Complete resection was achieved in 11 patients (55%), 8 patients (40%) had partial resection with or without enteroenteric bypass and 1 patient (5%) underwent palliative gastrojejunostomy and biopsy for an unresectable duodenal lesion.
Three patients died in the 30-day postoperative period. One patient, who had undergone bowel resection for a perforated metastatic lesion, recovered but was re-explored 3 weeks later because of peritonitis, which proved to be due to another perforated metastatic lesion. A second patient, known to have liver metastases, underwent palliative resection but had ascites with peritonitis and died of septicemia 3 weeks after surgery. The third patient who had brain metastases improved symptomatically with radiotherapy but suffered unrelenting acute complete small-bowel obstruction and was operated on with palliative intent. He died postoperatively of disseminated malignant disease.
There were four complications: wound infection, pneumonia, prolonged paralytic ileus that resolved with nonoperative management and a postoperative anastomotic hemorrhage that was controlled by reexploration.
Of the 11 patients who had complete resection, 4 (36%) were alive and disease-free at 2, 5, 8 and 10 years, respectively, after resection. All had stage III disease prior to the development of their intestinal metastases. All had multiple lesions. In this group there was only one postoperative complication, which was the anastomoticsite hemorrhage. The mean survival in the remaining patients in this group, who died, was 19.5 months. Two of them were known to have lung and brain metastases prior to their intestinal disease. One patient was well and disease-free for 7 years after resection and died of disseminated prostatic cancer. The remaining four patients died with distant metastases (to liver in two patients and to brain in two patients) within 7 months of the small-bowel resection.
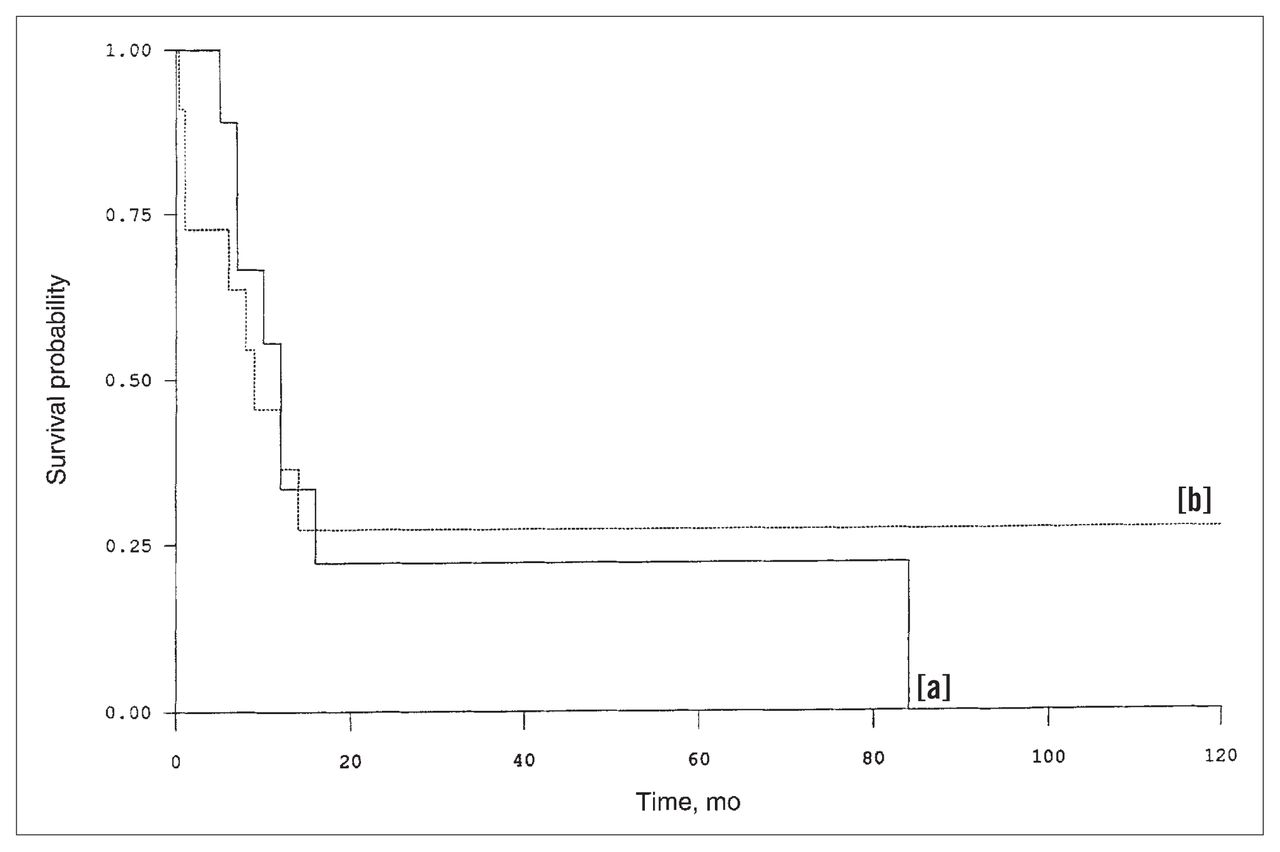
In the partial resection (and palliative bypass) group, all nine patients have died. Three patients died within 30 days of operation. For the remaining six patients, the mean postoperative survival time was 10.8 months (Fig. 1).

Survival of patients with melanoma metastatic to small bowel, according to type of resection: complete (solid line [a]) or partial (dotted line [b]).
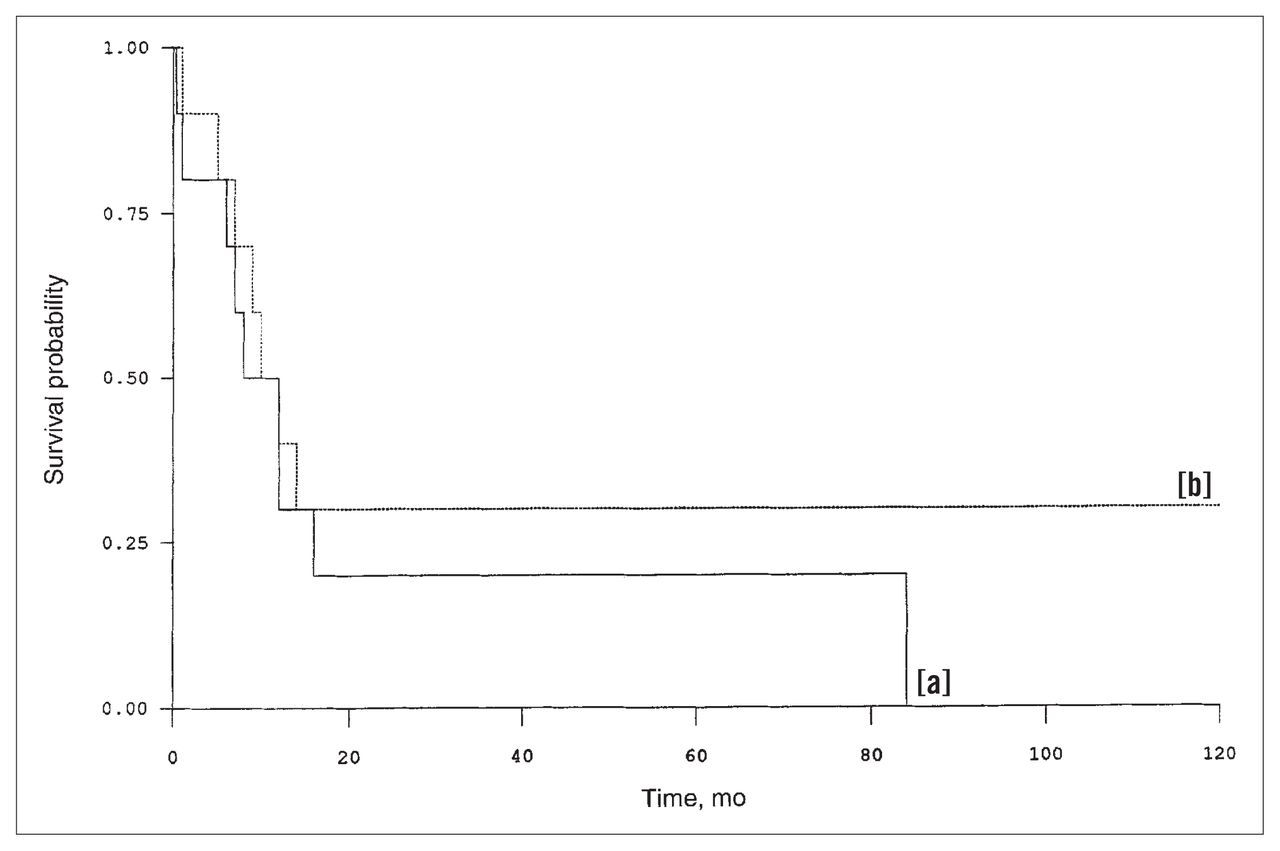
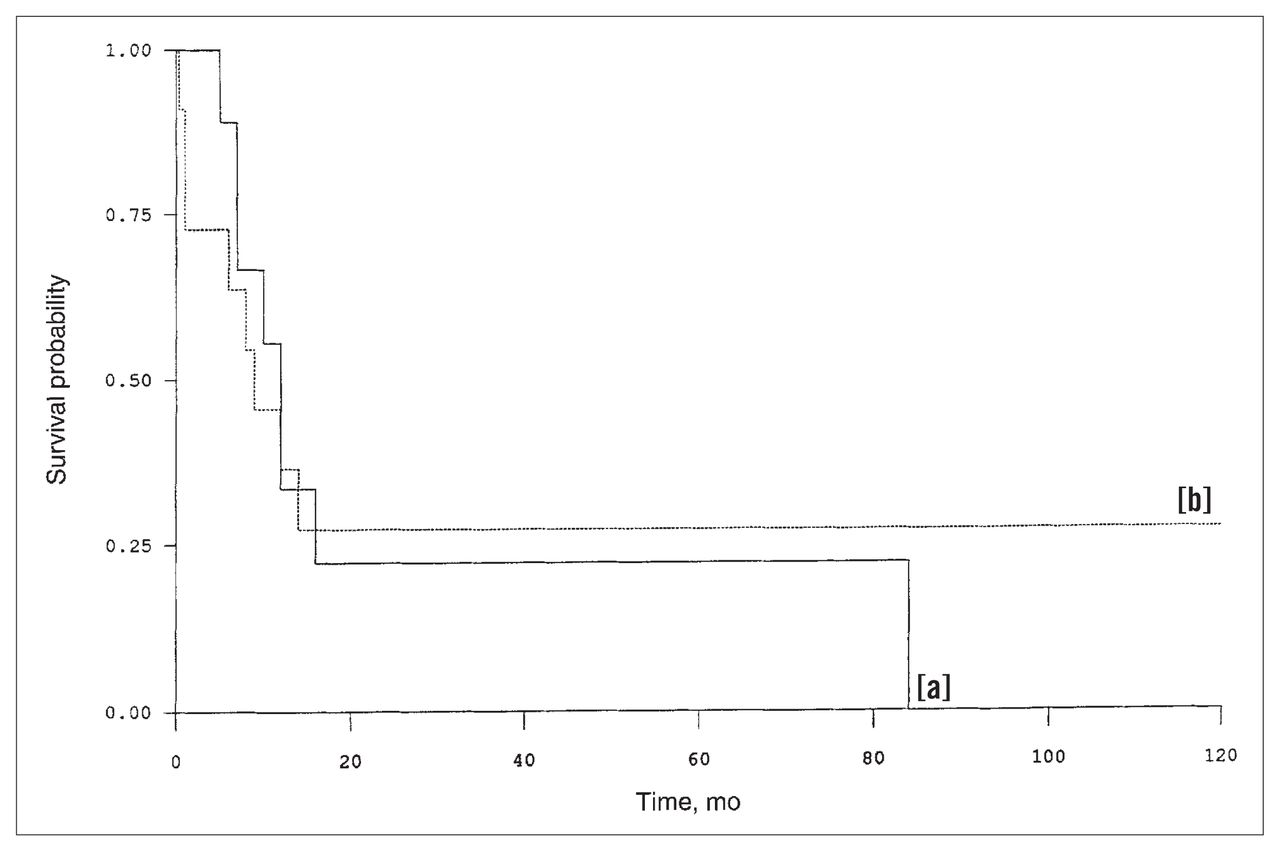
Analysis of actuarial survival figures showed a statistically significant difference (p < 0.036) according to type of resection performed, in favour of complete resection. When the patients were restratified according to the local extent of the disease, 9 patients had disease limited to the bowel wall and 11 patients had disease extending to the mesentery or omentum. However, there was no significant difference in survival between these two groups (Fig. 2). Likewise the time interval between the primary cutaneous melanoma and the development of intestinal metastases did not significantly influence survival (Fig. 3).
Survival according to extent of metastatic disease: intestinal (solid line [a]) or extra-intestinal (dotted line [b]).
Survival according to time from diagnosis of primary disease to intestinal metastatic disease: less than 3 years (solid line [a]) or 3 years or longer (dotted line [b]).
Discussion
The frequency of small-bowel metastases from melanoma in our study was 1.3%, similar to the 1.5% reported by Reintgen and colleagues1 and the 1.4% reported by Gutman and associates.4 The most common site was the jejunum, a finding that is in agreement with other reports.1,5 The lesions are described in the literature as either polypoid pedunculated masses arising from the mucosa or well-circumscribed submucosal nodules.1,6,7 Occasionally they are amelanotic or composed of spindle cells and thus may be confused with poorly differentiated carcinoma or leiomyosarcoma. Immunohistochemical methods are employed to detect markers like S-100 protein, which will help to differentiate between these tumours.
The resectability rate of small-bowel metastases from melanoma varies from 26% to 88%1,5 in different series. Our rate was 55%. Complete resection resulted in four survivors and seven patients who died. Two of them had other visceral metastases preoperatively and four had metastases shortly after resection (within 7 months). It is likely that their metastases were present preoperatively but were not detected on routine clinical and radiologic examinations. The remaining patient lived for 7 years after resection and died of another primary cancer. It has been shown that complete resection gives superior survival for gastrointestinal metastases and metastases at other sites.6,8,9 Our results are in agreement with this. Our 5-year survival rate was 15%, and one other patient was alive and disease-free 2 years after resection. Klaase and Kroon7 reported a 19% survival rate in 23 patients with gastrointestinal metastases and Caputy and associates10 reported a 9% survival in 41 patients.
After excluding the three perioperative deaths in our series, the mean and median survival rates were 2.5 years and 1 year respectively. It is hard to compare these results with those of previous reports because of different patient characteristics, but, generally speaking, the mean survival reported in the literature ranges from 1 to 2 years,1,5,11 the median survival time being less than 1 year.5,12
(Since compiling these data we have encountered another patient with small-bowel metastases from melanoma. This 26-year-old woman had a lower-extremity melanoma excised in 1988. Her first relapse was in the jejunum 4 years later. The involved bowel was resected, but she had another intra-abdominal recurrence 8 months later, which was also resected. She has been in good health for more than 2 years with no evidence of disease clinically or radiologically.)
The reports in the literature on the prognostic significance of relapse-free survival in malignant melanoma are conflicting. Roses and colleagues8 and Karakousis and associates13 have shown a better outcome with longer relapse-free survival in metastatic melanoma in general, but other reports7,10 of gastrointestinal relapse do not support this observation. In our study, the time interval between diagnosis of the primary melanoma and small-bowel metastases did not affect survival. Also, we found that extension of the disease to the mesentery or omentum did not affect survival, probably because it did not prohibit complete resectability. Unfortunately we could not find any other study that addressed this issue. The key determinants of survival are complete resection and the absence of other distant metastases. Because this is a retrospective study, the information on quality of life and relief of symptoms could not be accurately reported.
In summary, patients with a history of melanoma who present with gastrointestinal symptoms, especially obstruction or bleeding, should be investigated for intestinal metastases. Surgical intervention with complete resection of all visible tumour may be associated with long-term survival and should be attempted, since alternative therapeutic options are ineffective.
Acknowledgments
We thank Ms. Ita Smyth for typing the manuscript, and Mrs. Manuela Das Neves and Mrs. Virginia Raposo from the Tumour Registry of the Royal Victoria Hospital, Montreal, for their invaluable assistance.
- Accepted March 16, 1996.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.