


Abstract
In adults splenorenal arterial bypass is a highly effective treatment for renovascular hypertension, but in children the procedure has been less successful because of the small size of the splenic artery. However, with the improvement in microvascular techniques the procedure is now possible in children. A 2-year-old child with Takayasu’s arteritis, previous right nephrectomy and severe renovascular hypertension required revascularization to salvage his remaining left kidney. A splenorenal arterial bypass was performed through a left retroperitoneal flank incision. Postoperatively his creatinine level returned to normal and his requirements for antihypertensive medication were markedly diminished. The advantages of a splenorenal arterial bypass for left renal revascularization in a developing child are discussed.
Splenorenal bypass is a highly effective treatment for renovascular hypertension in adults. Because of the small size of the splenic artery, this method has been less successful in children.1,2 However, with improved microvascular surgical techniques, the procedure has great potential in children. We describe a successful splenorenal bypass performed on a 2-year-old child with Takayasu’s disease (an inflammatory vascular disease, affecting most often the aorta and its main branches3).
Case report
A 2-year-old boy, weighing 13 kg, was referred for investigation and control of renovascular hypertension. The child initially presented at 9 months of age with intussusception and coincidentally was found to have severe hypertension. Investigation led to a diagnosis of Takayasu’s large cell arteritis localized to the abdominal aorta (middle aortic syndrome). The right renal artery was occluded, but the left renal artery appeared to be normal. The child was initially treated with captopril and nifedipine. A right nephrectomy was performed in an attempt to control the renovascular hypertension. After nephrectomy no antihypertensive medications were required to maintain a normal blood pressure.
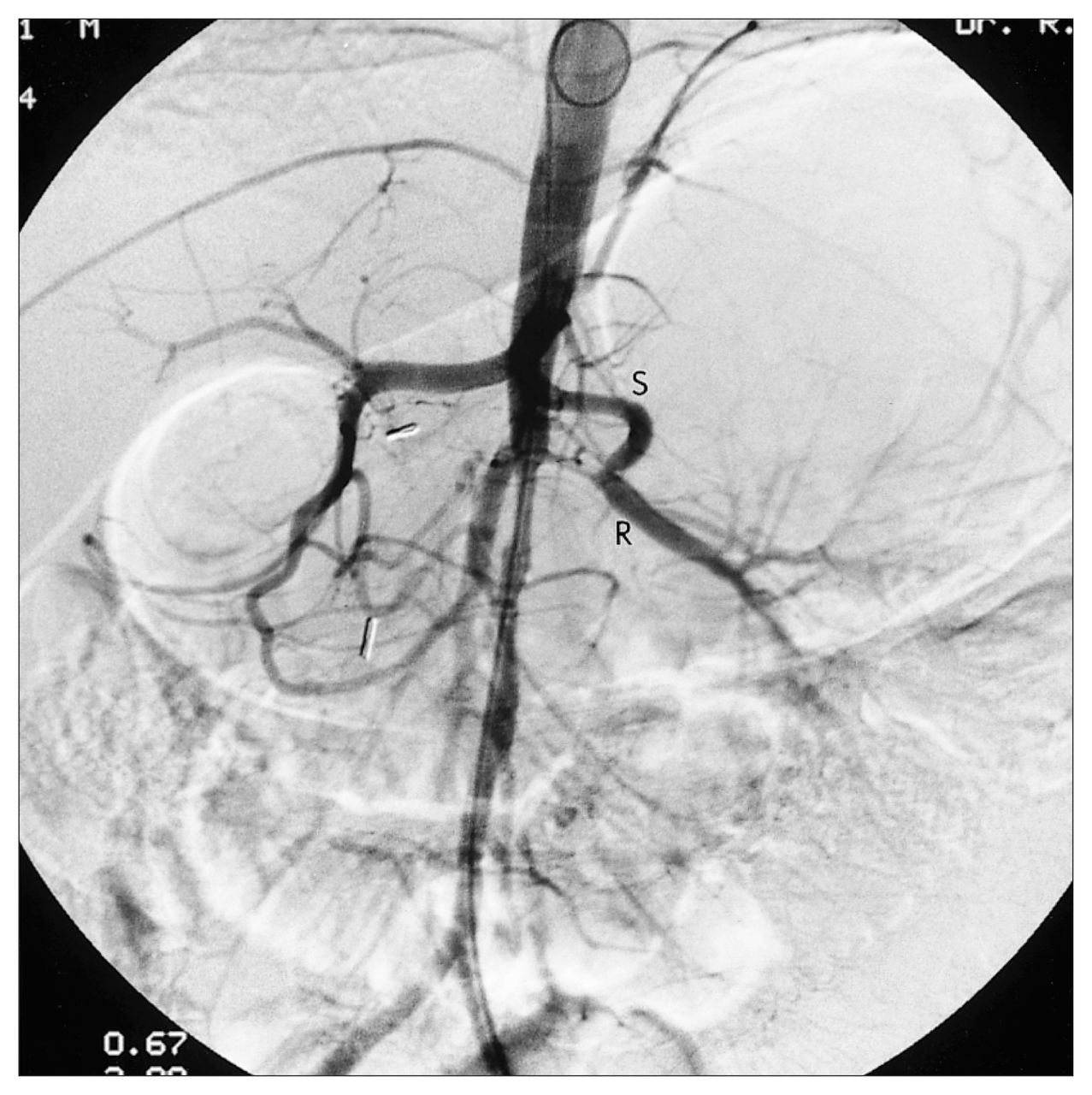
The child was readmitted at 27 months of age because the hypertension recurred. Physical examination revealed severe hypertension and an abdominal bruit. Antihypertensive medications, consisting of propranolol (15 mg three times daily), captopril (5 mg three times daily) and nifedipine (20 mg three times daily) were instituted. Despite these high doses, his hypertension remained poorly controlled. The serum creatinine level was elevated at 84 μmol/L. Repeat aortic angiography showed progression of his arteritis, with a severe stenosis of the origin of the left renal artery, as well as complete occlusion of the superior mesenteric artery (Fig. 1). The celiac axis and splenic artery were normal. Chest radiography revealed mild cardiomegaly, and electrocardiography demonstrated left ventricular hypertrophy.

Abdominal aortic angiogram prior to splenorenal bypass. There is significant narrowing of proximal left renal artery (R) and occlusion of superior mesenteric artery. Splenic artery (S) is well preserved and of good calibre.
Left renal artery angioplasty was attempted but was unsuccessful. After this procedure his creatinine level increased to 186 μmol/L but gradually decreased to preangioplasty levels over several days. Surgical revascularization of the left renal artery was scheduled in an attempt to salvage the remaining kidney and gain better control of the hypertension.
The operation was performed through a left retroperitoneal flank incision, and the left kidney, renal and splenic arteries were exposed. The diameter of the splenic artery was 4 mm and of the proximal left renal artery was 3 mm. Mannitol (12.5 g) was administered intravenously 45 minutes before renal cross-clamping, and heparin (100 units/kg intravenously) was given immediately before clamping of the arteries. The splenic artery was ligated and divided close to the splenic hilum. The spleen remained well perfused through the short gastric vessels. The proximal splenic artery was then anastomosed end to side to the renal artery with a running 7-0 polypropylene suture. The renal cross-clamp time was 34 minutes. After release of the clamps, there was a markedly improved pulse in the left renal artery distally. He was maintained on dopamine at 3 g/kg per minute for 24 hours postoperatively to optimize renal perfusion.
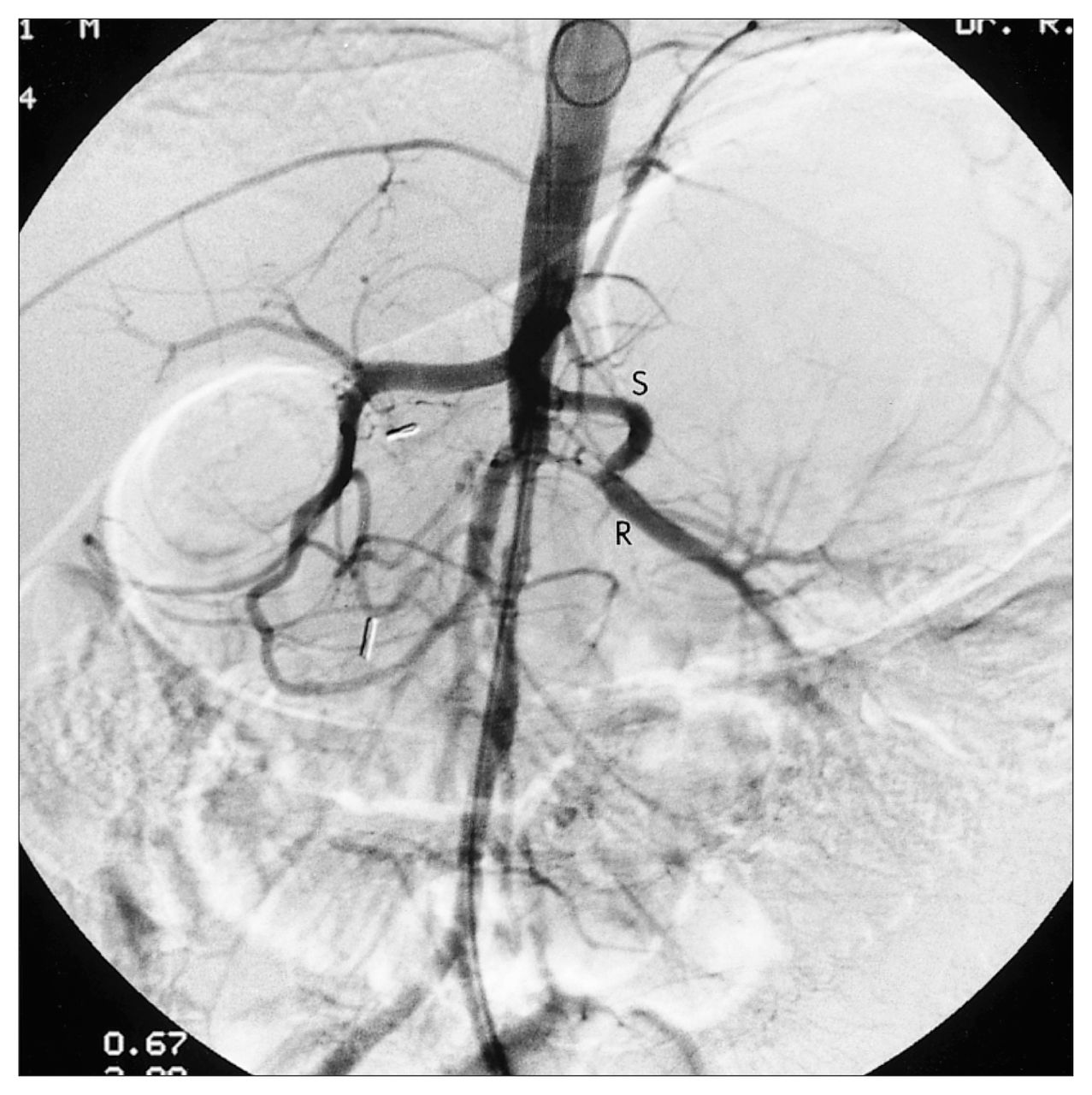
The splenorenal bypass was well tolerated. The serum creatinine level decreased to normal (55 μmol/L) over 2 days . Normal function of the left kidney was confirmed 6 days postoperatively by nuclear renal scanning. His hypertension became much more easily managed. He was started on prednisone in the hope of preventing further progression of his Takayasu’s disease. He was discharged on the 13th postoperative day. Five months postoperatively he was normotensive (120/70 mm Hg), being maintained on propranolol (10 mg orally twice a day) and prednisone (5 mg orally once a day). Repeat aortic angiography (Fig. 2) confirmed the patency of the splenorenal bypass with excellent perfusion of the left kidney. His serum creatinine level was stable 18 months postoperatively at 46 μmol/L.
Abdominal aortic angiogram 5 months after splenorenal bypass. Splenic artery (S) and splenorenal anastomosis are patent and there is excellent perfusion of distal left renal artery (R).
Discussion
Stenosis and occlusion of elastic arteries are characteristic features in the chronic phase of Takayasu’s disease.4 Although conservative treatment may be considered in the initial treatment of the inflammatory process, drug therapy cannot treat stenotic lesions in the aorta or great arteries.3 In this case, the severe hypertension caused by renal artery stenosis was poorly responsive to drug therapy, and the child had already required a nephrectomy. Surgical treatment was deemed necessary to salvage the remaining kidney and to reduce the severity of the hypertension. A splenorenal bypass was considered to be the most effective means of treatment.
The catastrophic consequences of uncontrolled high blood pressure during infancy and childhood are being recognized more frequently. Specifically, there is an increasing awareness of the relatively high incidence of renovascular hypertension in children.5 Pokrovsky3 found this type of hypertension in 55% of patients with Takayasu’s disease, based morphologically on primary involvement of the abdominal aorta and secondary involvement of the renal artery orifices. This finding is made even more significant by the fact that heart failure resulting from hypertensive cardiomyopathy is one of the major causes of death in Takayasu’s disease.3
The results of angioplasty for renal artery stenosis in children are quite variable. This technique is best suited for stenosis of the middle or distal renal artery.6 Attempts to dilate proximal ostial lesions, especially those associated with aortic anomalies are likely to be unsuccessful,7 as was the case with this child. In one series of pediatric cases,8 60% of unsuccessful angioplasties resulted in nephrectomy.
Surgical intervention is regarded as more effective than medical management in the treatment of renovascular hypertension.5 Revascularization of the kidney is a technically challenging operation, and several options for arterial reconstruction exist. The optimal procedure depends on specific factors.
Splenorenal bypass was considered to be the best option for revascularizing this small child’s left kidney. He had previously undergone a right nephrectomy, and therefore preserving his left kidney and avoiding renal dialysis was of paramount importance. Aortorenal bypass involves greater dissection and the use of a bypass graft. Use of polytetrafluoroethylene as graft material increases the risk of thrombosis and infection; use of saphenous vein would be technically difficult because of its small size (2 mm diameter) and has been associated with complications, including aneurysmal degeneration and subintimal hyperplasia.9 Dean, Berkowitz and O’Neill10 found that the incidence of aneurysmal degeneration of a saphenous vein graft in sequential long-term angiographic follow-up studies approaches 100% when grafted to the main renal artery. Neither a saphenous vein graft nor a synthetic graft could be expected to grow with the child and would therefore limit the chance of long-term success. Autotransplantation of the kidney involves an increased risk of renal failure particularly in a child who has already lost one kidney.
The case described demonstrates the excellent result possible with a splenorenal bypass to provide revascularization in a child with severe renovascular hypertension. A splenic artery bypass provides an autologous arterial connection. The risk of infection and thrombosis is reduced by avoiding the use of foreign materials. Use of an arterial conduit decreases the potential for aneurysmal degeneration. The splenic artery in this child was of comparable size to the renal artery and can be expected to grow with the child. The splenorenal approach avoids surgical dissection of the abdominal aorta. The retroperitoneal approach employed avoids entry into the abdomen, which may be important in patients having undergone previous abdominal surgery. The technique is efficient requiring only one vascular anastomosis. Use of the splenic artery does not endanger the vascular supply to the spleen as it continues to be fed by the short gastric vessels from the stomach.11
There have been a number of reports of splenorenal arterial bypass in children,2,3,5,9,11,12 but to our knowledge this 2-year-old child is the youngest to undergo this procedure.11 The results of the splenorenal bypass for treatment of renovascular hypertension secondary to Takayasu’s disease in this young boy have been excellent. A splenorenal arterial bypass should be considered an effective option for left renal revascularization in children.
- Accepted August 15, 1995.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.