


Abstract
Ampullary tumours are uncommon. They may occur with familial polyposis syndromes or neurofibromatosis. It can be difficult to distinguish them from their periampullary counterparts on clinical, radiologic or histologic grounds. Because most ampullary and periampullary tumours are malignant, they tend to be treated by radical surgery. A 67-year-old man was seen with a sporadic ampullary hamartoma that simulated cancer. It was succesfully treated by local excision through a transverse duodenotomy.
Ampullary tumours are uncommon. However, because of their strategic location at the confluence of the common bile duct and pancreatic duct, they are usually symptomatic.1–3 Periampullary neoplasms are far more common, and in this group carcinoma of the head of pancreas is most frequently seen.3,4 Because of the difficulties in differentiating ampullary from periampullary tumours clinically5 and radiologically3 and the problems in establishing a definitive tissue diagnosis based on endoscopic biopsies,1–3 it is often impossible to categorize these tumours preoperatively.3,6 A high proportion of the ampullary tumours are malignant, 1,3,6,7 so there is a tendency to manage them by extensive surgical excision. 1,3,5–9 We describe the case of a man who had a sporadic ampullary hamartoma that was treated by local transduodenal excision.
Case report
A 67-year-old man had severe epigastric pain and cachexia. He had a history of 2 episodes of acute uncomplicated pancreatitis 4 and 7 years previously. Endoscopic retrograde cholangiopancreatography (ERCP), abdominal ultrasonography and abdominal CT done shortly after the second episode gave normal results. His serum amylase, bilirubin and liver enzyme levels were normal except for mild elevation of the γ-glutamyl transferase level. Over the next 4 years, the epigastric pain worsened. It was “boring” in character, radiated to the back and was aggravated by eating. He lost approximately 9 kg over 18 months. On admission to hospital, the serum amylase, bilirubin and liver enzyme levels were again normal except for a mildly elevated γ-glutamyl transferase level at 67 U/L (normal 10 to 50 U/L). A secretin test indicated a diminished duodenal bicarbonate concentration of less than 70 mmol/L, and the bentiromide (Chymex) test value was 41% (normal 70% to 100%). ERCP demonstrated mild dilatation of the common bile duct. He was considered to have chronic pancreatitis and was treated with pancrelipase.
After 6 months of pancrelipase therapy, the pain was still severe but now was worse at night and when supine. He had lost his appetite and continued to lose weight. Serum bilirubin and amylase levels were normal, the serum aspartate aminotransferase level was 115 U/L (normal 10 to 40 U/L), the serum alanine aminotransferase level was 85 U/L (normal 0 to 40 U/L), the serum alkaline phosphatase level was 205 U/L (normal 30 to 110 U/L) and the serum γ-glutamyl transferase level was 298 U/L (normal 10 to 50 U/L). Abdominal ultrasonography revealed mildly dilated common bile and common hepatic ducts. CT of the abdomen gave normal results as did hepatobiliary nuclear imaging. ERCP demonstrated a dilated common bile duct and pancreatic duct (Fig. 1). The ampulla of Vater was abnormally protuberant and granular, but a biopsy specimen could not be obtained owing to technical difficulties.
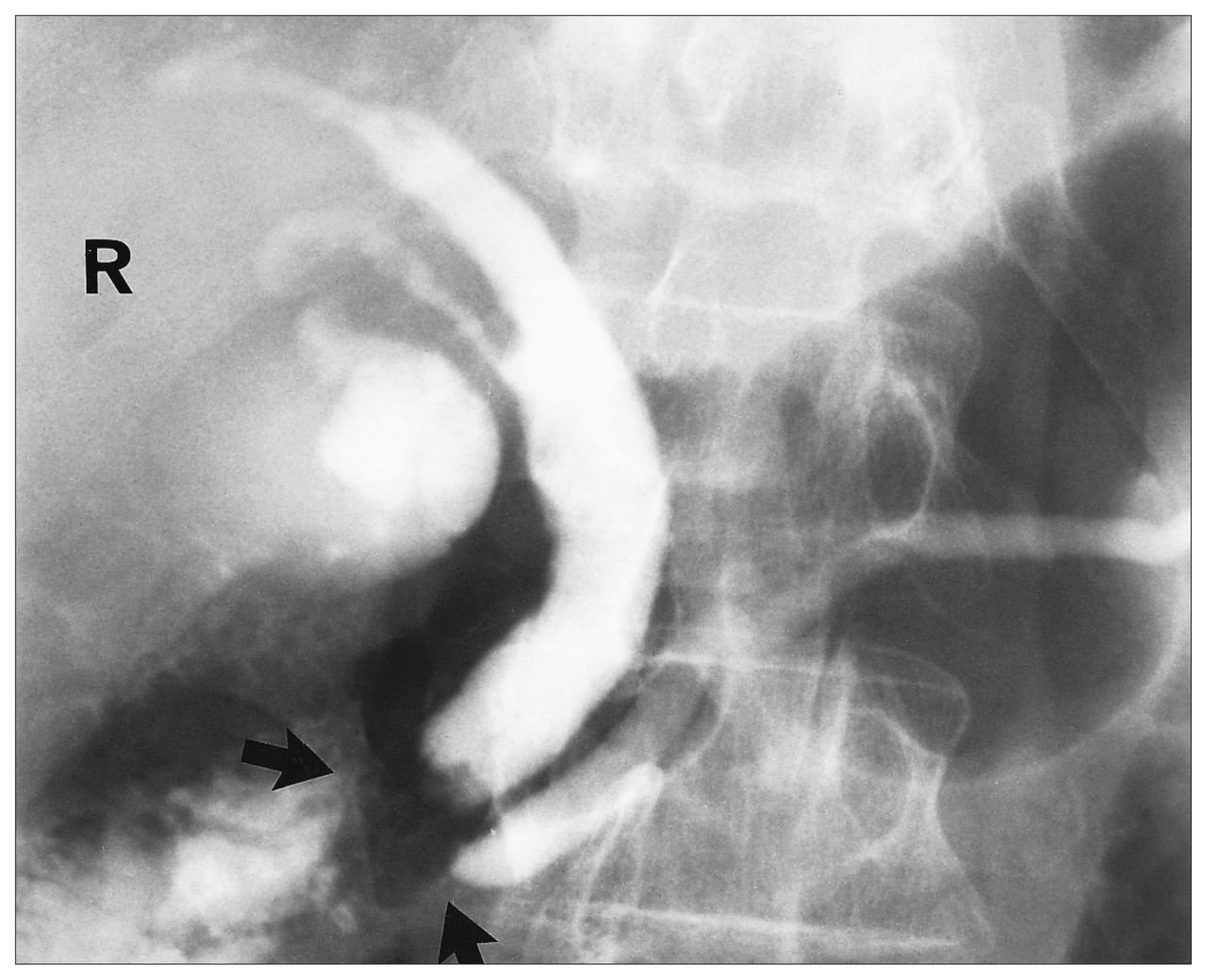
Endoscopic retrograde cholangiopancreatography showing dilatation of the common bile and pancreatic ducts. Note the irregular filling defect (arrows) suggestive of a neoplasm in the ampullary region. R = right.
It was suspected that this abnormal ampulla represented the cause of the patient’s symptoms, and because of suspected malignant disease of the ampulla, the patient agreed to undergo laparotomy. The mass was found to be limited to the ampulla, and there was no suspected periampullary involvement. For this reason, the ampulla was explored through a transverse duodenotomy. The mass was not unduly firm, and the mucosa overlying it appeared unremarkable; a frozen section was not ordered. The entire mass was removed by local excision of the ampulla of Vater (Fig. 2) with reanastomosis of the pancreatic and common bile ducts to the duodenum. A cholecystectomy was carried out at the same time. Pathological examination of the ampullary mass showed it was a hamartoma; it was composed of a haphazard admixture of cystically dilated glandular elements, associated with a slight degree of fibromuscular proliferation and an increased number of ectatic blood vessels and lymphatics (Fig. 2). The gallbladder was devoid of calculi and was essentially normal. The patient recovered from the procedure without complications and was discharged home pain free on the 14th postoperative day on the pancreatic enzyme supplement. More than 4 years later, he remained pain free and his weight was stable. At no time preor postoperatively did physical examination or upper and lower gastrointestinal endoscopy disclose any other hamartomas, nor did the patient have any family history of this problem.

Low-power view (left) of part of the hamartoma that is centred around a dilated duct (hematoxylin–eosin, original magnification × 5). High-power view (right) of the hamartoma showing a disorderly admixture of blood vessels, lymphatics, glandular structures and smooth-muscle elements (hematoxylin–eosin, original magnification × 115).
Discussion
The ampulla of Vater is a vaseshaped structure adjacent to the second part of the duodenum below the surface of the papilla into which the common bile duct and, in most cases, the main pancreatic duct drain.3,4 The embryologic development of the papilla and the variations thereof are complex,2–4 which in turn makes the clinicopathologic manifestations of its lesions rather interesting. The ampullary hamartoma is a case in point; these lesions are uncommon, and only a small number of cases have been described in the literature.1,2,9,10 They have also variously been referred to as adenomyosis, adenomyomas, cystadenomas or fibroadenomas depending on their histologic constitution.2,9,10 However, the central tenet to all these appellations is that they represent a haphazard, non-neoplastic overgrowth of tissues normally found at that site.1,4,9,10
With respect to ampullary growths as a whole, hamartomas are far outnumbered by real tumours.2,3,5,7 The commonest entity in the latter category is carcinoma,3,5 followed by other neoplasms such as adenomas, carcinoids, leiomyomas, fibromas, lipomas, lymphangiomas, hemangiomas and granular cell tumours.2–4,8–10 However, the clinical presentation of ampullary hamartomas is generally similar to that of the real neoplasm, the features being largely due to partial, intermittent or complete common biliary or pancreatic duct obstruction, or both,1,3,8–12 as was the case in this report.
Imaging modalities such as barium series, CT, routine and endoscopic ultrasonography and ERCP help considerably in defining the topography of these lesions.5,6,13,14 Despite this, it may be difficult to determine whether a tumour is primarily ampullary, with spread to the periampullary region, or vice versa.3,5,6 More importantly, it may be more difficult to detect small ampullary lesions especially if they do not protrude into the papilla;1,3 thus, the symptoms they produce may be erroneously attributed to chronic relapsing pancreatitis or to biliary lithiasis.1,3,11,12 Even with endoscopic biopsies, taken for instance at ERCP, there are also potential diagnostic pitfalls that relate to the special nature of biliary tract histology, particularly in the ampullary region. 2,4,6 Hence, normal ampullary tissues can be mistaken for carcinoma by virtue of such features as perineural invasion. Alternatively, lesions harbouring carcinoma may be labelled as normal or benign especially if the biopsy is superficial or from a well-differentiated carcinoma.2–4
There is an association between ampullary neoplasms and hamartomas on the one hand and familial polyposis syndromes such as Gardner syndrome and Peutz–Jeghers syndrome,15–18 or neurofibromatosis,12 on the other. However, ampullary lesions can also be isolated and sporadic as in our case. Apart from ampullary neoplasms, heterotopic pancreatic tissue has to be considered in the differential diagnosis, on embryologic grounds.3,4 However, the predominance of vascular structures with haphazardly ar ranged elements of smooth muscle and intestinal epithelium, as well as the absence of both exocrine and endocrine pancreatic tissue in the present case augurs against this possibility.
- Accepted June 25, 1996.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.