


Abstract
Objective: To describe the clinical course of a group of patients in whom sarcoma of the proximal femur was diagnosed at the time of reconstructive hip surgery.
Design: A retrospective case series.
Setting: Final management of all patients took place at a tertiary care centre.
Patients and Interventions: Six consecutive patients with sarcoma of the proximal femur diagnosed at the time of reconstructive hip surgery. The mistaken diagnoses made before surgery were benign tumour (2 patients), avascular necrosis (2 patients), subtrochanteric fracture due to metastasis (1 patient) and granuloma from a loose hip implant (1 patient). The final diagnosis was osteosarcoma in 3 patients and chondrosarcoma in 3. Three patients with high-grade sarcoma received neoadjuvant chemotherapy followed by femoral or pelvic resection, or both, and reconstruction. Two patients with chondrosarcoma underwent wide excision of the tumour with allograft or modular implant reconstruction. One patient with widespread metastasis received only palliative chemotherapy.
Main outcome measures: Overall survival with respect to oncologic and functional results of treatment.
Results: Two patients (1 who received only palliative chemotherapy) died after 5 and 21 months’ follow-up, respectively. Average follow-up for the remaining 4 patients was 65.2 months (range from 51 to 75 months). They were disease free at latest follow-up. One patient required amputation for septic complications related to the reconstruction.
Conclusions: Limb salvage surgery for sarcoma of the proximal femur is challenging when the diagnosis is made at the time of reconstructive surgery rather than through an appropriately planned biopsy. However, this series suggests that limb preservation is feasible and that hindquarter amputation is not the only solution.
Sarcomas of bone are rare tumours; most orthopedic surgeons will see only a few examples during their career.1 The initial diagnostic work-up of this malignant tumour is an important aspect of planning successful limb salvage therapy, and an appropriate biopsy is considered fundamental to limb preservation. 1–3 Extensive surgery performed at the site of an unrecognized bone sarcoma compromises the eventual surgical resection of the lesion by spreading disease into the surrounding tissues.1,3 Hindquarter amputation (hemipelvectomy) probably offers the most straightforward option for local disease control in a patient referred with a diagnosis of sarcoma found at the time of reconstructive surgery. However, after extensive manipulation of a tumour in the proximal femur, even hemipelvectomy may not remove all contaminated tissues.
In this paper we present a consecutive series of 6 patients referred to a tertiary care musculoskeletal oncology unit after a primary bone sarcoma had been discovered during reconstructive hip surgery. We describe the initial errors made in diagnosis of the bone sarcoma and the principles of subsequent management.
Patients and method
Six consecutive patients ranging in age from 35 to 74 years (average 54 years) were referred to our institution after having undergone inappropriate reconstructive surgery on the hip for suspected benign disease (5 patients) or metastatic carcinoma (1 patient), which eventually turned out to be bone sarcoma. The initial diagnosis was benign tumour in 2 patients, subtrochanteric fracture secondary to metastatic carcinoma in 1 patient, avascular necrosis of the femoral head in 2 patients and granuloma due to a loose total hip arthroplasty in 1 patient (Table I).
Summary of Diagnosis, Treatments and Final Outcome in 6 Patients Who Had Bone Sarcoma Diagnosed at the Time of Reconstructive Surgery
The final diagnosis was osteosarcoma in 3 patients and chrondrosarcoma in 3. We reviewed the charts of these patients to determine what steps could have been taken to avoid the initial inappropriate surgery, what subsequent therapy they received after referral to the oncology unit and what were the oncologic and functional results of treatment. The duration of follow-up ranged from 4 to 71 months.
Results
Two patterns of inappropriate management were recognized in the initial care of these patients: (a) the surgeon recognized that there was a tumour present in the proximal femur but did not establish the appropriate histologic diagnosis; (b) the surgeon failed to recognize that a tumour was present.
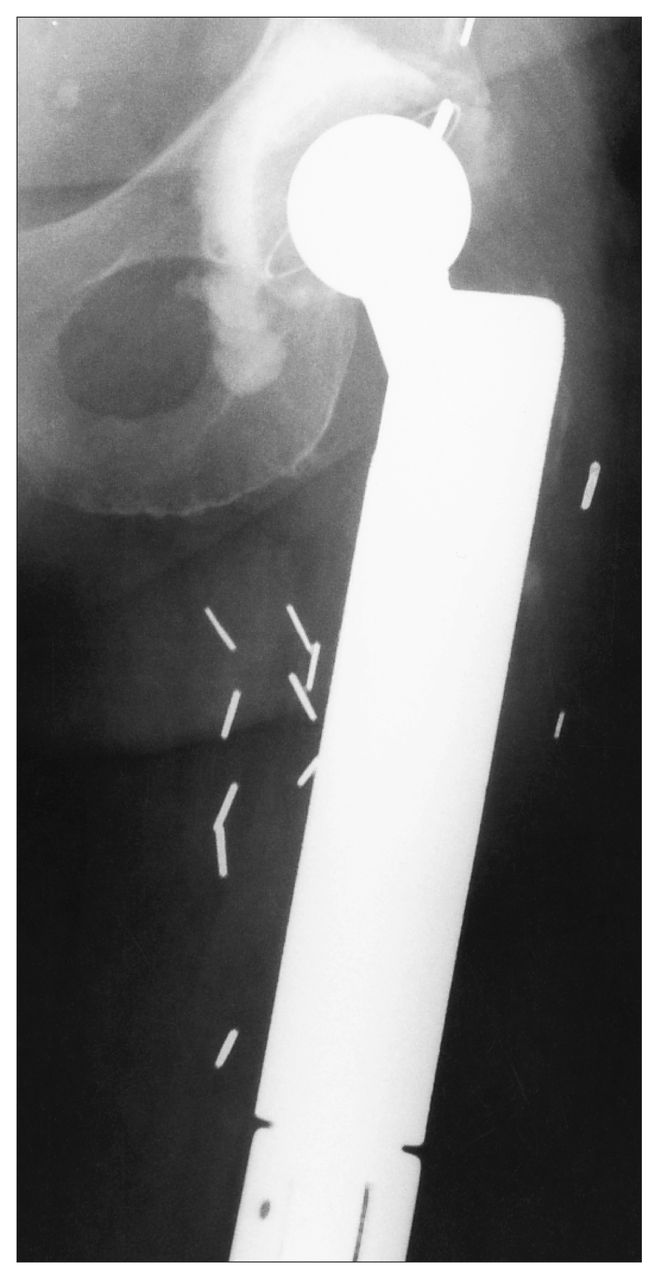
In 3 patients the surgeon identified a tumour using plain radiographs and cross-sectional imaging. In none of these 3 was a biopsy specimen or frozen section obtained before proceeding with definitive management. In 2 patients (nos. 1 and 2 in Table I) the surgeon decided that the lesion was benign (giant cell tumour and enchondroma) without benefit of any pathological evaluation (Fig. 1). These 2 patients underwent curettage and bone grafting of the “benign” tumour; in one of them (no. 2) a hip screw and side plate were also inserted (Fig. 2). In a third patient (no. 3), the initial surgeon assumed that a pathologic subtrochanteric fracture of the proximal femur was due to metastatic carcinoma and performed closed reduction, inserting a locking nail without obtaining a biopsy specimen for diagnosis (Fig. 3). Several days later the tumour was recognized as a de-differentiated chondrosarcoma. In none of these 3 patients was a frozen section obtained early in the operation. The diagnosis of sarcoma was recognized only from the permanent specimens reported several days after the initial procedure had been completed.
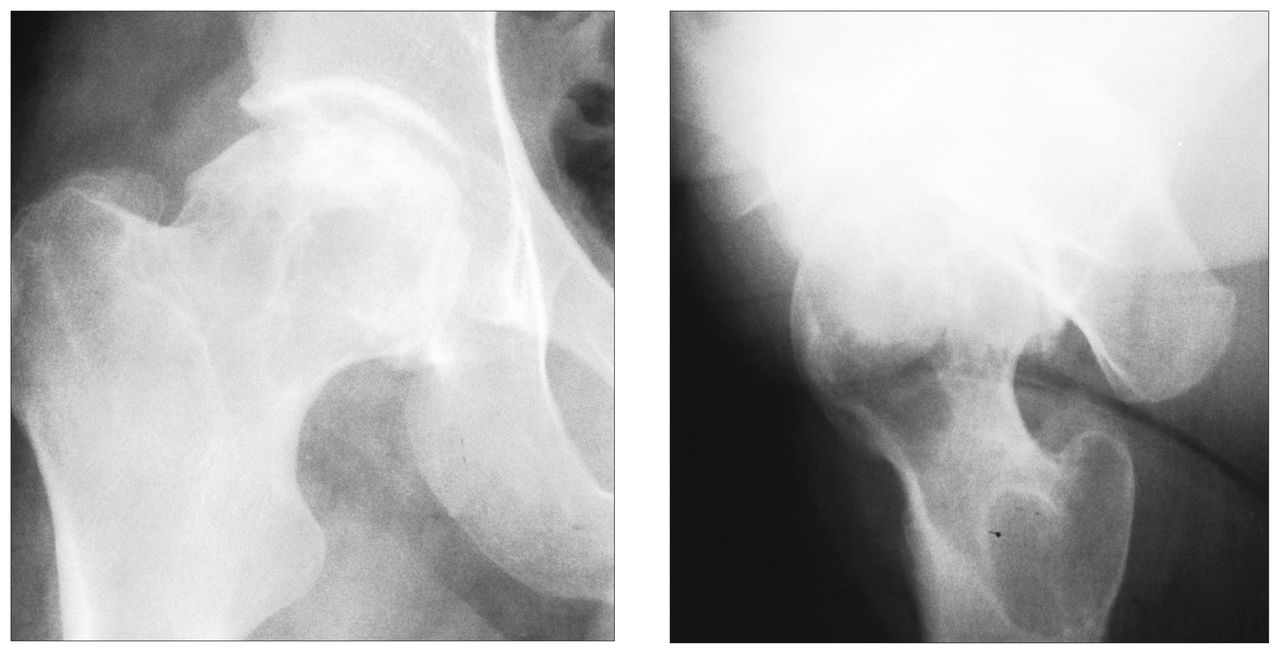
Case 1. Anteroposterior (left) and lateral (right) conventional radiographs of the right hip illustrate a lytic lesion within the anteroinferior aspect of the right femoral head, with extension into the anterior aspect of the femoral neck, thought to be a benign giant cell tumour. On histologic examination after curettage and autografting, the mass was found to be an osteosarcoma.

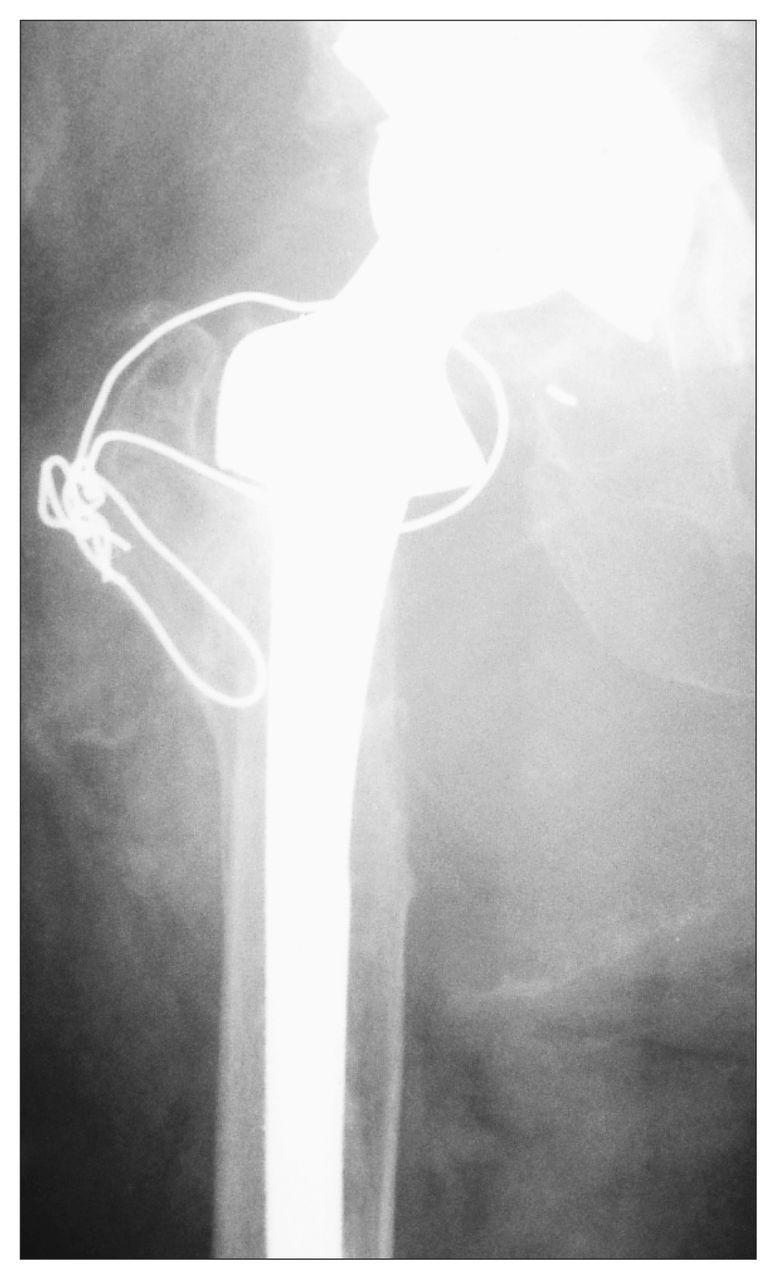
Case 2. A plain radiograph of the left hip illustrates fracture of a prosthesis in a patient treated by curettage, autografting and screw/plate fixation for what was thought to be an enchondroma. The lesion was found to be a chondrosarcoma (grade 2/3).

Case 3. An anteroposterior plain radiograph of the right hip after closed reduction and insertion of an intramedullary locking nail for what was presumed to be a pathologic fracture through metastatic carcinoma. The lesion was found to be a dedifferentiated chondrosarcoma.
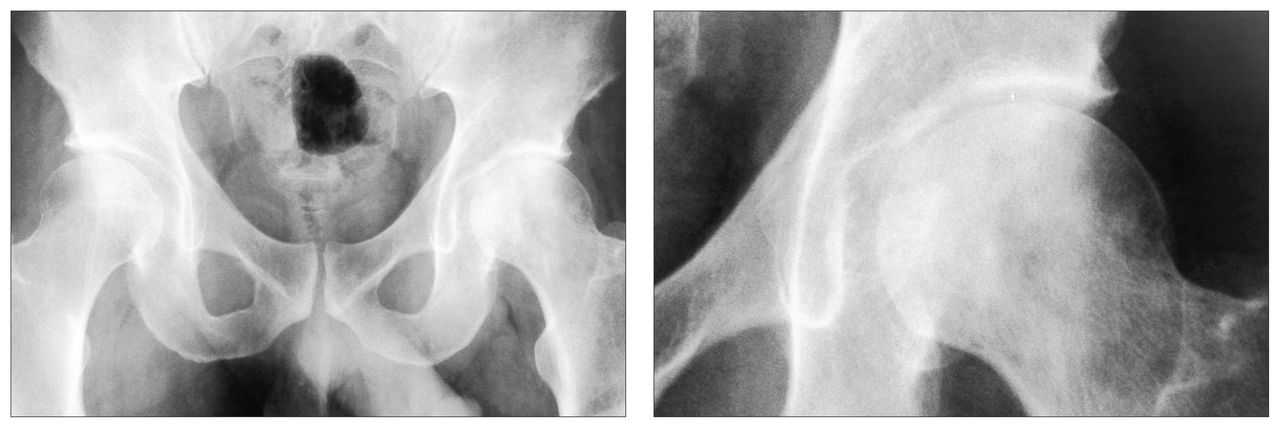
In the remaining 3 patients, the surgeon mistakenly diagnosed avascular necrosis preoperatively in 2 patients (nos. 4 and 5). In both, plain radiographs initially showed mottled sclerosis and lucency in the femoral head without subchondral crescentic lucency or joint collapse (Fig. 4). Nuclear medicine bone scanning demonstrated marked increased uptake. Neither patient underwent magnetic resonance imaging before the total hip arthroplasty. In patient 4, the sarcoma was not recognized on review of the pathological appearance of the resected femoral head. The diagnosis was made 2 months later after reexploration of the hip for presumed sepsis (Fig. 5). By this time the tumour was unresectable even by amputation and the patient died rapidly from metastasis. In patient 5 sarcomatous tissue was recognized intraoperatively after removal of the femoral head and reaming of the acetabulum (Fig. 6).

Case 4. Plain radiographs showing mottled sclerosis and lucency in the left femoral head without a subchondral crescentic lucency or joint collapse.

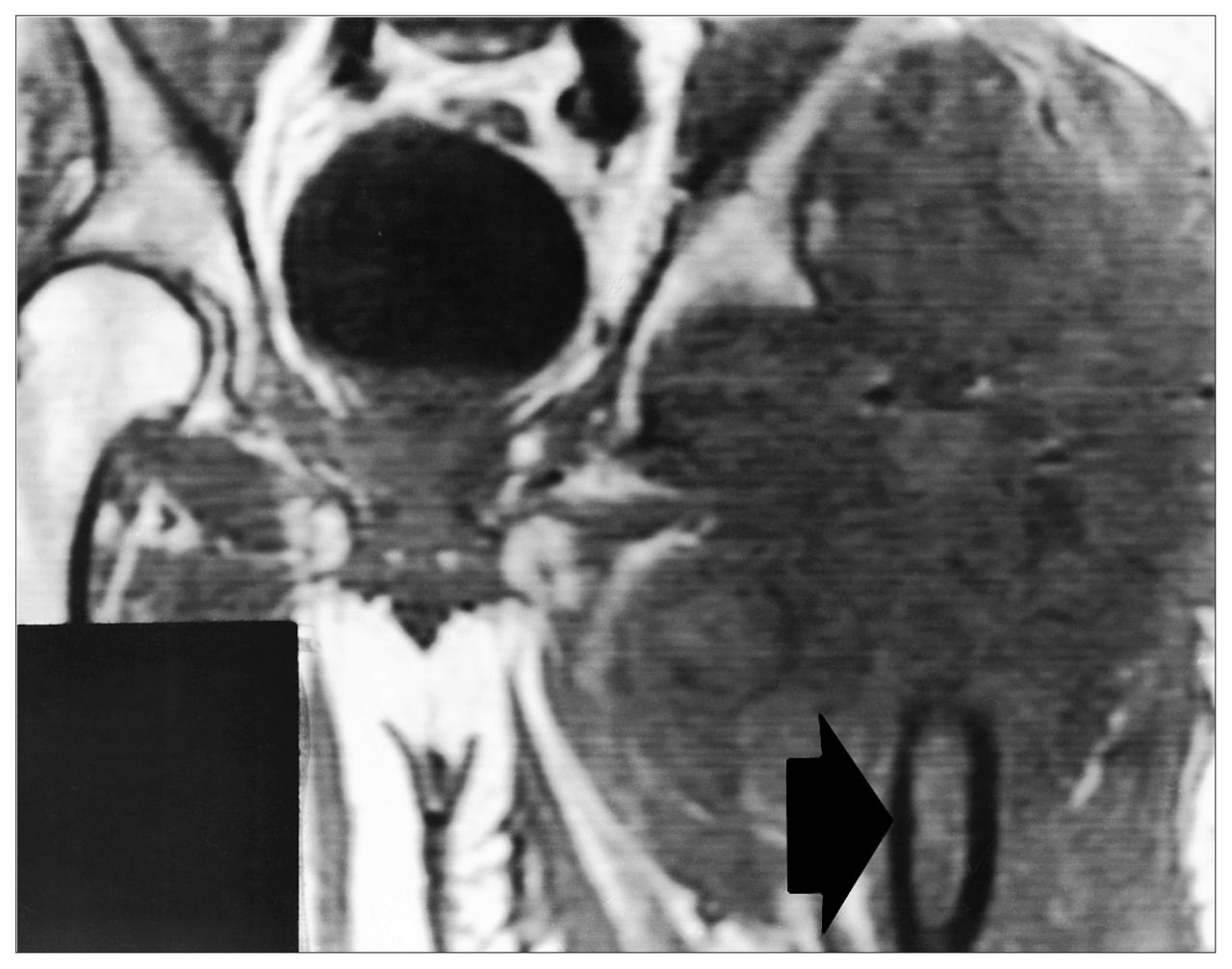
Case 4. Coronal T1-weighted magnetic resonance image of the pelvis 4 months after total hip arthroplasty was performed for avascular necrosis. The implant was removed 2 months after the initial procedure and an osteosarcoma was identified. A large extraosseous mass of low T1-weighted signal intensity is seen centred over the region of the left hip (arrow). Additionally, loss of normal T1-weighted marrow fat signal is seen within the residual proximal femur, presumably secondary to marrow edema or intramedullary tumour extension. The patient was given palliative chemotherapy and soon died from systemic metastasis.

Case 5. Postoperative radiograph of the left hip after removal of the femoral head and reaming of the acetabulum. Osteosarcoma was recognized intraoperatively during attempted total hip arthroplasty for presumed avascular necrosis. Old screw tracts are seen within the proximal femur from initial treatment with a hip screw and plate.
In the final patient in this series (patient 6), a large mass developed in the soft tissues surrounding a hip with a loose total joint replacement (Fig. 7). This was assumed to be a granuloma related to implant loosening. At the time of revision, the acetabular component was found to be loose, and extensive membrane was removed from the site. Within 3 months the mass reappeared and grew (Fig. 8). Biopsy demonstrated chondrosarcoma.

Case 6. A conventional anteroposterior radiograph of the right hip obtained before acetabular revision of the patient’s total hip arthroplasty. A large soft-tissue mass is seen medial to the proximal femur. The tissue pathological findings were not reviewed at the time of surgery.

Case 6. Computed tomography scan through the proximal thighs performed 3 months after acetabular revision. Despite the scatter from the femoral prosthesis, a large soft-tissue mass can be clearly seen along the medial and posterior aspect of the right femoral diaphysis. Irregular serpiginous calcification is seen within the posterolateral aspect of the mass.
The final diagnoses and presenting symptoms are summarized in Table I. After initial consultation, each patient was advised to undergo hindquarter amputation to achieve the best chance for local disease control. Every patient rejected this advice.
After review of the pathological findings, all patients with high-grade sarcomas were advised to receive neoadjuvant (i.e., preoperative) chemotherapy, which was subsequently given to 2 patients with osteosarcoma (patients 1 and 5) and 1 patient with de-differentiated chondrosarcoma (patient 3). The chemotherapy consisted of cisplatin and doxorubicin.4–9 In patient 4 (with unresectable osteosarcoma) the disease progressed despite chemotherapy and no surgery was performed.
The definitive surgical management of patients with a sarcoma who have undergone prior surgery involves the removal of all tumour and potentially contaminated tissue at the local site.1 The patients in this series required extensive resection in order to achieve this goal since their initial reconstructive procedures violated a number of tissue planes and involved acetabular reaming in 2 patients (nos. 5 and 6). In these patients, most of the musculature about the hip and thigh required resection, as well as any neurovascular structures that were contaminated with tumour.
Staging studies of the local site of tumour origin were difficult to interpret in 4 of the 6 patients since metallic devices had been inserted in the hip. Despite these limitations, both MRI and CT provided useful information (Figs. 5 and 8). Pathological review of the resected tumours revealed resection margins that were free of malignant cells in every case.
In 2 patients, the pelvis was contaminated with tumour; this occurred in 1 patient from tumour extension and in the other from acetabular reaming at the time of attempted total hip arthroplasty (Fig. 6). These 2 patients required en bloc pelvic and femoral resection. Reconstruction was achieved using hemipelvic and proximal femoral allografts with a long-stemmed total hip arthroplasty (Figs. 9 and 10).10,11

Case 5. After neoadjuvant chemotherapy, the proximal femur and a portion of the pelvis were resected and reconstructed with an allograft implant. This radiograph of the hip was obtained 5 years after the reconstruction.

Case 6. Radiographs of the proximal right femur (left) and pelvis (right) after hemipelvic and proximal femoral resection and reconstruction with a hemipelvic allograft and proximal femoral allograft implant.
The remaining 3 patients had proximal femoral tumours without acetabular extension. They underwent wide resection of their tumours with reconstruction of the femoral defect using either an allograft-implant (patient 1) or a modular endoprosthesis (patients 2 and 3) (Figs. 11 and 12).

Case 1. Anteroposterior view of the right hip after neoadjuvant chemotherapy and limb salvage surgery shows resection of the proximal femur and reconstruction with a composite allograft implant.
Case 2. A radiograph of the left hip after limb salvage surgery shows resection of the proximal femur and reconstruction with a proximal femoral tumour prosthesis.
Two patients died of disseminated disease during the follow-up period; the one who received palliative chemotherapy only and the one with a dedifferentiated chondrosarcoma who had a total femoral replacement.
The average follow-up for the remaining 4 patients was 65.2 months (range from 51 to 75 months). One patient with osteosarcoma had a solitary pulmonary metastasis resected 24 months postoperatively.12 She was free of disease, both systemically and locally, 75 months postoperatively. There were no local tumour recurrences.
Of the 4 patients who underwent limb salvage and were alive at follow-up, 3 were functioning well. Two patients (nos. 2 and 5) were walking with a single cane and 1 patient (no. 1) was walking with no assistance. All 3 were performing activities of daily living without difficulty. Two of the 3 patients who were working preoperatively had returned to work at the time of follow-up.
One patient (no. 6) suffered a spontaneous bowel perforation 8 months after pelvic allograft replacement. Subsequently, chronic dislocation of her prosthesis developed and eventually she required hindquarter amputation 5 years postoperatively for recurrent abdominal sepsis associated with her pelvic allograft.
Discussion
The topic of unrecognized primary malignant bone tumour discovered at the time of reconstructive hip surgery has not been discussed in the literature. Cases of sarcoma arising from a total hip arthroplasty or a metallic implant have been reported.13–17 It is possible that in some of these patients (especially those in which the period between the hip arthroplasty and discovery of the tumour was short) the tumour was present and missed at the time of initial arthroplasty.
The diagnosis of a primary bone tumour can be difficult,1,2 and certainly the appropriate diagnosis should be sought by a consultative process involving the pathologist, radiologist and orthopedic surgeon. In the patients we have presented, the process of diagnosis failed because either the surgeon recognized a proximal femoral tumour but thought that the lesion was not a primary sarcoma or the surgeon failed to recognize the presence of a tumour.
Mankin, Lange and Spanier3 have discussed the hazards of taking a biopsy in patients with primary bone tumours. For patients with these rare tumours who are treated by non-experts, the risks of inappropriate diagnosis or management are high. The present series emphasizes a further danger: definitive treatment of a bone tumour before a definitive diagnosis has been made.
In this review, 2 patients were treated for presumed benign lesions of the femoral neck. The risk of fracture after biopsy of a femoral neck lesion is certainly worrisome, and reconstruction of the proximal femur at the time of biopsy may be warranted if a definite diagnosis of benign tumour is obtained from a frozen section of the biopsy sample. However, a definitive diagnosis may be difficult to achieve with immediate frozen sections, and it is critical that expert pathologists, radiologists and clinicians agree with all aspects of the diagnosis before the patient receives further treatment. We therefore advise that these patients be referred to a centre with subspecialty expertise in musculoskeletal pathology before the biopsy is undertaken. We recognize that bone biopsy at most skeletal sites is performed at primary or secondary care hospitals in Canada. However, the difficulty in planning and interpreting primary tumour bone biopsies from the proximal femur is such that these patients warrant referral.
In this review, patients 1 and 2 were treated with curettage and bone grafting (as well as insertion of fixation devices in patient 2). The treatment would likely have been easier and the outcome better had the initial surgeon delayed definitive management and performed only a biopsy.
Patient 3 demonstrates the error of assuming that all pathologic fractures in adults are due to metastatic cancer. This patient presented with a subtrochanteric fracture through an obvious lytic lesion. Although there was no history of tumour elsewhere, the surgeon assumed that this lesion must be metastatic from another site and proceeded to fixate the fracture with an intramedullary device thereby spreading tumour from the femoral head to the knee and extensively contaminating the abductor muscles. Total femoral resection was required to remove the sarcoma. In older patients presenting with a solitary pathologic fracture the surgeon should always search for evidence (by history, physical examination and appropriate investigations [i.e., total body bone scanning]) of a primary tumour that may have metastasized to the bone. Even if a primary cancer is identified, the surgeon should proceed with caution and ensure that a pathologist is present to interpret a frozen section at the time of biopsy before proceeding with definitive fixation. If the frozen-section findings are inconclusive the patient should be placed in traction until a reliable diagnosis is made. Reaming the fracture site in order to pass an intramedullary device is particularly contraindicated if the lesion is a sarcoma since tumour implants may embolize into the venous circulation.
These misdiagnosed cases of proximal femoral lesions suggest that referral to a subspecialty unit was indicated before biopsy. Subspecialty management is not necessary for most patients with metastatic disease in the proximal femur. However, those who have solitary lesions (especially if there is no history of malignant disease elsewhere) should probably be referred before a biopsy is done.
In the first 3 cases, recognition of the tumour could have prompted referral to a surgical oncologist. However, in the latter 3 cases, patients were thought to have conditions that are normally managed by reconstructive surgeons. The 2 patients thought to have avascular necrosis demonstrated mottled lucency and sclerosis of the femoral head on plain radiographs (Fig. 4), but in neither case was the localized subchondral crescent sign or joint collapse typical of advanced osteonecrosis demonstrated. To avoid this management error, patients with symptomatic osteonecrosis who do not show typical changes should be assessed through MRI.18 If the image obtained is not typical of osteonecrosis, biopsy should precede any reconstructive procedure.
A similar situation applies in patients with soft-tissue masses or dramatic bone lysis associated with an implant. Although the diagnosis in most of these cases will be granulomatous pseudotumours caused by wear debris from the implant, the surgeon should not neglect the possibility of a sarcoma. Before any definitive treatment, a biopsy of the mass should be taken, and material from cystic lesions should always be sent for pathological evaluation.
Radical surgical treatment of all 6 cases would have entailed a hind-quarter amputation,1,19 since extensive spread of the tumour around the hip had resulted from the initial procedure. The extent of tissue contamination was difficult to assess in the patients with implanted metallic devices because of inherent imaging artifacts encountered on cross-sectional imaging. Generally it was necessary to discuss personally with the surgeon the initial surgical approach in order to plan the extent of tissue resection necessary to achieve local tumour control. In most patients it was necessary to excise critical muscular structures around the hip (abductors and hip flexors) that had been contaminated at the initial operation. In 3 patients, contamination of the anterior pelvis also required femoral nerve resection along with the hip flexors.
After an initial assessment, all patients were advised to undergo amputation at the level of the sacroiliac joint to achieve the highest chance of local disease control. All patients rejected this advice in favour of the limb salvage option even though they recognized the higher risk of local tumour recurrence. All patients with high-grade bone sarcomas were treated with adjuvant chemotherapy before their eventual resection. Limb-salvage surgery with adequate tumour-free margins was possible in 5 of the 6 patients in this series and the sixth patient could not have been managed adequately even with a hindquarter amputation. There were no local relapses after a minimum follow-up of 2 years in the 4 surviving patients. These cases represent extreme examples of limb salvage surgery, but there is no question that they are functionally better than they would have been with a hindquarter amputation.5,6,9,20–24
Conclusions
It would be unwise to draw definitive conclusions about the course of treatment in this small series of patients. However, it is fair to comment that a biopsy should be done in cases of presumed benign lesions of the proximal femur before definitive treatment and in cases of solitary bone lesions in which the tumour is assumed to be metastatic. Cases of avascular necrosis should be investigated preoperatively by MRI if subchondral crescentic lucency and femoral head collapse are not evident on conventional radiographs, and “pseudotumours” presumed to arise from implant wear debris should be viewed with suspicion if they are growing rapidly. The surgeon should obviously avoid the situation of discovering a sarcoma during or after performing a reconstructive procedure. However, the results in this small series of patients suggest that hemipelvectomy is not the only solution when this occurs and that limb salvage surgery should be considered if the patient refuses amputation.
- Accepted October 22, 1997.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.