


Abstract
Objective: To determine major thromboembolic and hemorrhagic complications and predictive risk factors associated with aortic valve replacement (AVR), using bileaflet mechanical prostheses (CarboMedics and St. Jude Medical).
Design: A case series.
Setting: Cardiac surgical services at the teaching institutions of the University of British Columbia.
Patients and Methods: Patients in 2 age groups who had undergone AVR between 1989 and 1994 were studied. Group 1 comprised 384 patients younger than 65 years. Group 2 comprised 215 patients 65 years of age and older.
Results: The linearized rates of major thromboembolism (TE) occurring after AVR were 1.54%/patient-year for group 1 and 3.32%/patient-year for group 2; the rates for major TE occurring more than 30 days after AVR were 1.13%/patient-year for group 1 and 1.55%/patient-year for group 2. The crude rates for major TE occurring within 30 days of AVR were 1.04% for group 1 and 3.72% for group 2. The death rate from major TE in group 1 was 0.31%/patient-year and in group 2 was 0.88%/patient-year. Of the major TE events occurring within 30 days, 100% of patients in both age groups were inadequately anticoagulated at the time of the event, and for events occurring more than 30 days after AVR, 45% in group 1 and 57% in group 2 were inadequately anticoagulated (INR less than 2.0). The overall linearized rates of major hemorrhage were 1.54%/ patient-year for group 1 and 2.21%/patient-year for group 2. There were no cases of prosthesis thrombosis in either group. The mean (and standard error) overall freedom from major TE for group 1 patients at 5 years was 95.6% (1.4%) and with exclusion of early events was 96.7% (1.3%); for group 2 patients the rates were 90.0% (3.2%) and 93.7% (3.0%), respectively. The mean (and SE) overall freedom from major and fatal TE and hemorrhage for group 1 patients was 90.1% (2.3%) and with exclusion of early events was 91.2% (2.3%); for group 2 patients the rates were 87.9% (3.1%) and 92.5% (2.9%), respectively. The 5-year rate for freedom from valve-related death for group 1 patients was 96.3% (2.1%) and for group 2 patients was 97.2% (1.2%).
Conclusion: The thromboembolic and hemorrhagic complications after AVR with bileaflet mechanical prostheses occur more frequently and result in more deaths in patients 65 years of age and older than in patients years younger than 65 years.
Mechanical and biological prostheses have been used for aortic valve replacement (AVR) for 25 years. For the past 18 years there has been a choice of bileaflet and monoleaflet mechanical prostheses, formulated primarily from pyrolytic carbon. The St. Jude Medical mechanical prosthesis (St. Jude Medical, Minneapolis, Minn.) was introduced in 1977 and has been the most widely implanted bileaflet mechanical prosthesis. 1–10 The CarboMedics mechanical prosthesis (Sulzer-CarboMedics Inc., Austin, Tex.) was introduced in 1989 and received market approval from the Food and Drug Administration of the United States in 1993.11–15
In this study we evaluated the combined experience in AVR surgery of the St. Jude Medical and CarboMedics mechanical prostheses. The study was not a randomized trial but was conducted by the same cardiac surgical services at the teaching institutions of the University of British Columbia.
We evaluated our experience with the CarboMedics and St. Jude Medical mechanical prostheses from September 1989 to June 1994 to determine overall the clinical performance of pyrolytic carbon bileaflet prostheses in AVR for patients younger than 65 years and for patients 65 years of age or older. Patients were considered according to these 2 age groups because mechanical prostheses are recommended for patients younger than 65 years, whereas extensive experience from our centre has suggested that bioprostheses be used for patients 65 years of age and older because of the markedly reduced incidence of structural valve deterioration necessitating reoperation.16–19 The freedom from structural valve deterioration 12 years postoperatively was 94% for patients 65 to 69 years of age at implantation and 96% for patients 70 years of age or older at implantation.
Patients
The CarboMedics prosthesis was implanted in 293 patients (206 men, 87 women) and the St. Jude Medical prosthesis in 306 patients (219 men, 87 women) between September 1989 and June 1994 for AVR. The populations were divided into 2 groups: group 1, those younger than 65 years and group 2, those 65 years of age or older.
Group 1
There were 384 patients (285 men, 99 women) in group 1. The mean age (and standard deviation) was 52.3 (10.4) years (range from 19 to 64 years). Of the 384 patients, 24% were in New York Heart Association (NYHA) class II, 56% in class III and 17% in class IV. Previous cardiac procedures had been performed in 15.4% of the patients. Concomitant procedures were performed in 24.0%; 16.7% were coronary artery bypass. AVR was performed electively in 87.5%, urgently in 10.7% and emergently in 1.8%. The mean follow-up was 2.53 (1.49) years with a total cumulative follow-up of 971.7 years. The follow-up was 97.4% complete.
Group 2
In this group there were 215 patients (140 men, 75 women). The mean age was 70.5 (4.6) years (range from 65 to 87 years). Of these patients, 27.9% were in NYHA class II, 57.0% in class III and 13.2% in class IV. Previous cardiac procedures had been performed in 14.9% of the patients. Concomitant procedures were performed in 40.5%; 39.1% were coronary artery bypass. AVR was performed electively in 90.2%, urgently in 7.9% and emergently in 1.9%. The mean follow-up was 2.10 (1.39) years with a total cumulative follow-up of 452.1 years. The follow-up was 93.0% complete.
The similarities between the 2 patient populations were evaluated for the incidence of coronary artery disease, previous cardiovascular surgery, concomitant procedures, valve disease and status of procedures (Table I).
Incidence of Coronary Artery Disease, Previous Cardiovascular Surgery, Concomitant Procedures, Valve Disease and Patient Status After Aortic Valve Replacement in Patients Less than 65 Years of Age (Group 1) and 65 Years of Age and Older (Group 2)
Methods and statistical analysis
The Guidelines for Reporting Morbidity and Mortality After Cardiac Valvular Operations were used for definitions of valve-related complications, categorization and statistical methods.20 The recommended definitions of thromboembolic and hemorrhagic events proposed by Bodnar and associates21 were incorporated in the evaluation. They categorized thromboembolic complications as follows: (a) valve thrombosis; (b) cerebrovascular accident, as occlusive (ischemic) or hemorrhagic in origin (in terms of transient ischemic attack [less than 24 hours]), reversible ischemic neurologic deficit (minor stroke) (more than 72 hours with complete resolution within 3 weeks) or major stroke; (c) systemic (noncerebral) embolism; and (d) systemic (noncerebral) bleeding.
The information on valve-related complications for this study was obtained by direct contact with patients, family physicians, consultants, hospital health records and official death registries over a closing interval of 6 months.
The valve-related complications and composite indices of these valve-related complications were evaluated in the time-related manner by actuarial life-table techniques (Cutler–Ederer method). The Lee–Desu statistic was used to provide comparison of complication-free curves. Linearized occurrence rates (events per 100 patient-years or percentage per patient-year) were used specifically for documenting thromboembolic and hemorrhagic complications. The hazard function graphs were determined from the life tables. The hazard function is expressed at 6-monthly intervals for 72 months.
Results
Death rates
Group 1
The early mortality of the overall population younger than 65 years was 2.6% (10 patients). There was 1 valve-related death due to prosthetic valve endocarditis, 5 cardiac deaths and 4 noncardiac deaths. The late mortality for this group was 1.75%/patient-year. The valve-related rate of late death was 0.51%/patient-year. Three deaths were due to thromboembolism and 2 to hemorrhage. The cardiac death rate was 0.62%/patient-year. Mean (and standard deviation) patient survival at 5 years was 88.9% (2.6%).
The clinical performance related to mortality for AVR revealed a total of 6 valve-related deaths (0.62%/patient-year), 1 early and 5 late, plus 1 sudden unexpected death (0.10%/patient-year). The freedom from valve-related death for patients in this group was 96.3% (2.1%) at 5 years.
Group 2
The early mortality of the overall population in this group was 7.0% (15 patients). There were 2 (13%) valve-related deaths, 7 (47%) cardiac deaths and 6 (40%) noncardiac deaths. The 2 valve-related deaths were due to thromboembolism. None of the other deaths were from valve-related causes.
The late mortality for these patients was 4.2%/patient-year. The valve-related mortality was 0.66%/patient-year. There were 2 thromboembolic deaths and 1 related to nonstructural dysfunction (periprosthetic leak). The cardiac death rate was 1.33%/patient-year. Mean patient survival at 5 years was 81.0% (3.1%).
The clinical performance related to the death rate for this group revealed a total of 5 (1.11%/patient-year) valve-related deaths, 4 thromboembolic (2 early and 2 late) and 1 from nonstructural dysfunction. There were no sudden unexpected deaths. The freedom from valve-related mortality for AVR was 97.2% (1.2%) at 5 years.
Major thromboembolic and hemorrhagic complications
The linearized rates of overall major thromboembolism were 1.54%/ patient-year for group 1 and 3.32%/ patient-year for group 2, and for major events that occurred beyond 30 days 1.13%/patient-year and 1.55%/ patient-year, respectively (Table II). The death rates associated with these complications were 0.31%/patient-year for group 1 and 0.88%/patient-year for group 2. There were no documented thrombotic events in either group. The linearized rates of hemorrhage were 1.54% and 2.21%/patient-year, respectively, for groups 1 and 2.
Major Thromboembolic and Hemorrhagic Complications After AVR in Group 1 and Group 2 Patients*
Major thromboembolic and hemorrhagic events have been further considered, in detail, for 2 time intervals, 30 days or less (Table III) and more than 30 days (Table IV). The major thromboembolic complications are documented as major reversible, major permanent and major systemic for the 2 groups. The hemorrhagic events are all major events. The crude rates of major thromboembolic events within 30 days were 1.04% (4 events) for group 1 patients and 3.72% (8 events) for group 2 patients.
Major Thromboembolic and Hemorrhagic Complications Occurring Within 30 Days After AVR in Group 1 and Group 2 Patients
Major Thromboembolic and Hemorrhagic Complications Occurring More Than 30 Days After AVR in Group 1 and Group 2 Patients
The anticoagulant status of patients with major thromboembolic events was obtained. Of the events that occurred within 30 days, all patients in both groups were inadequately anticoagulated (INR less than 2.0). Inadequacy for major TE occurring more than 30 days postoperatively was 45% (5 of 11) and 57% (4 of 7), respectively, for groups 1 and 2. Of the 10 events that occurred in hospital, overall 100% were associated with inadequate anticoagulation, and of the out-of-hospital complications 50% (6 of 12) of group 1 and 63% (5 of 8) of group 2 were associated with inadequate anticoagulation.
Table V illustrates the mean (and standard error) freedom from major thromboembolic and complications overall and with exclusion of early events (within 30 days) for the 2 age groups. At 5 years, the freedom from major thromboembolism for group 1 patients was 95.6% (1.4%) overall and 96.7% (1.3%) with exclusion of early events compared with 90.0% (3.2%) overall and 93.7% (3.0%), respectively, for group 2. There was 100% freedom from prosthesis thrombosis in our experience with the CarboMedics and St. Jude Medical prostheses in the aortic position.
Freedom From Major Thromboembolism, Overall and With Exclusion of Early Events, After AVR in Group 1 and Group 2 Patients
At 5 years’ follow-up, the freedom from major and fatal thromboembolism and hemorrhagic events for group 1 patients was 90.1% (2.3%) overall and 91.2% (2.3%) with exclusion of early events compared with, was 87.9% (3.1%) overall and 92.5% (2.9%), respectively for group 2 patients (Table VI).
Freedom From Major or Fatal Thromboembolism, Thrombosis and Hemorrhage, Overall and With Exclusion of Early Events, After AVR in Group 1 and Group 2 Patients
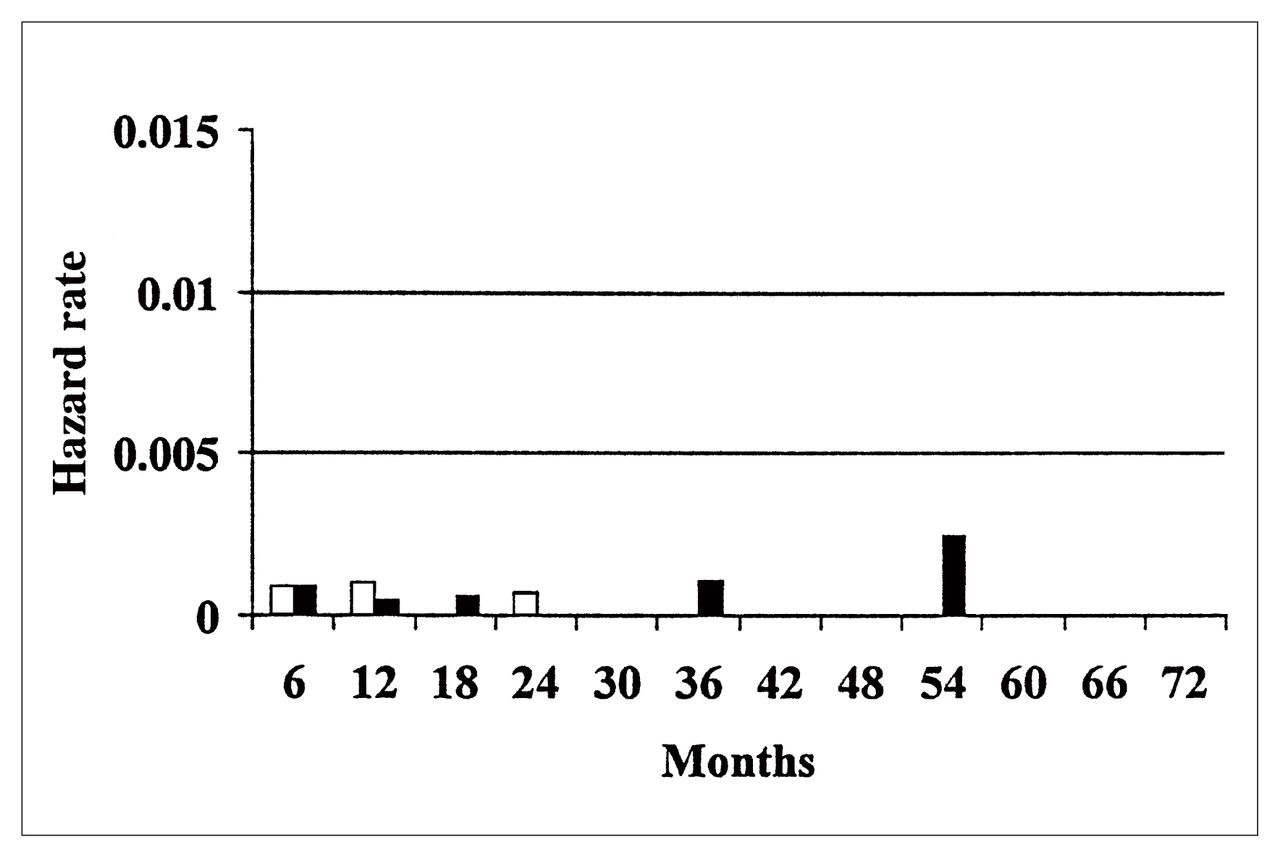
The hazard rates for overall thromboembolic and hemorrhagic events are demonstrated in Figs. 1 and 2 and for valve-related mortality and reoperation, including the death rate from reoperation, in Figs. 3 and 4.
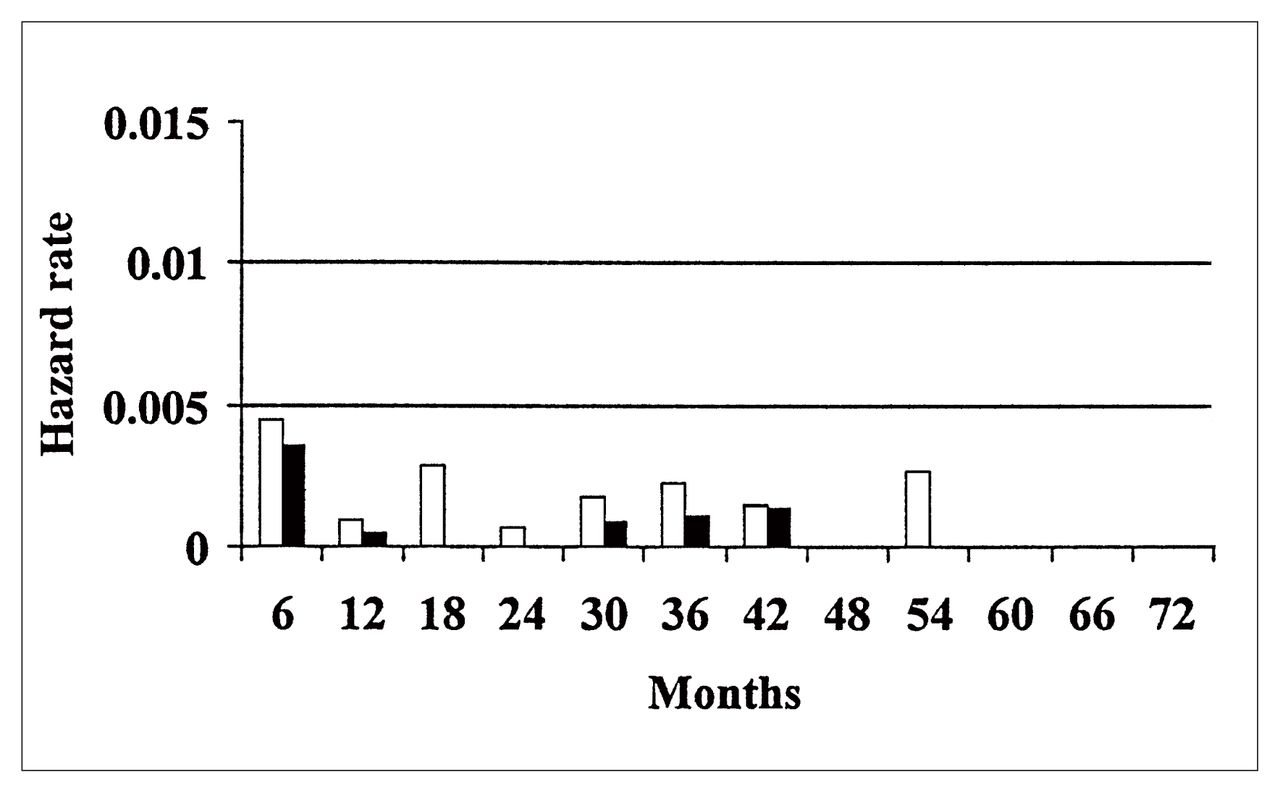
The hazard function of thromboembolic and hemorrhagic events after aortic valve replacement (AVR) in patients younger than 65 years (group 1). White bars = major thromboembolism, thrombosis, fatal thromboembolism and hemorrhage, black bars = major thromboembolism, thrombosis and fatal thromboembolism, without hemorrhage.
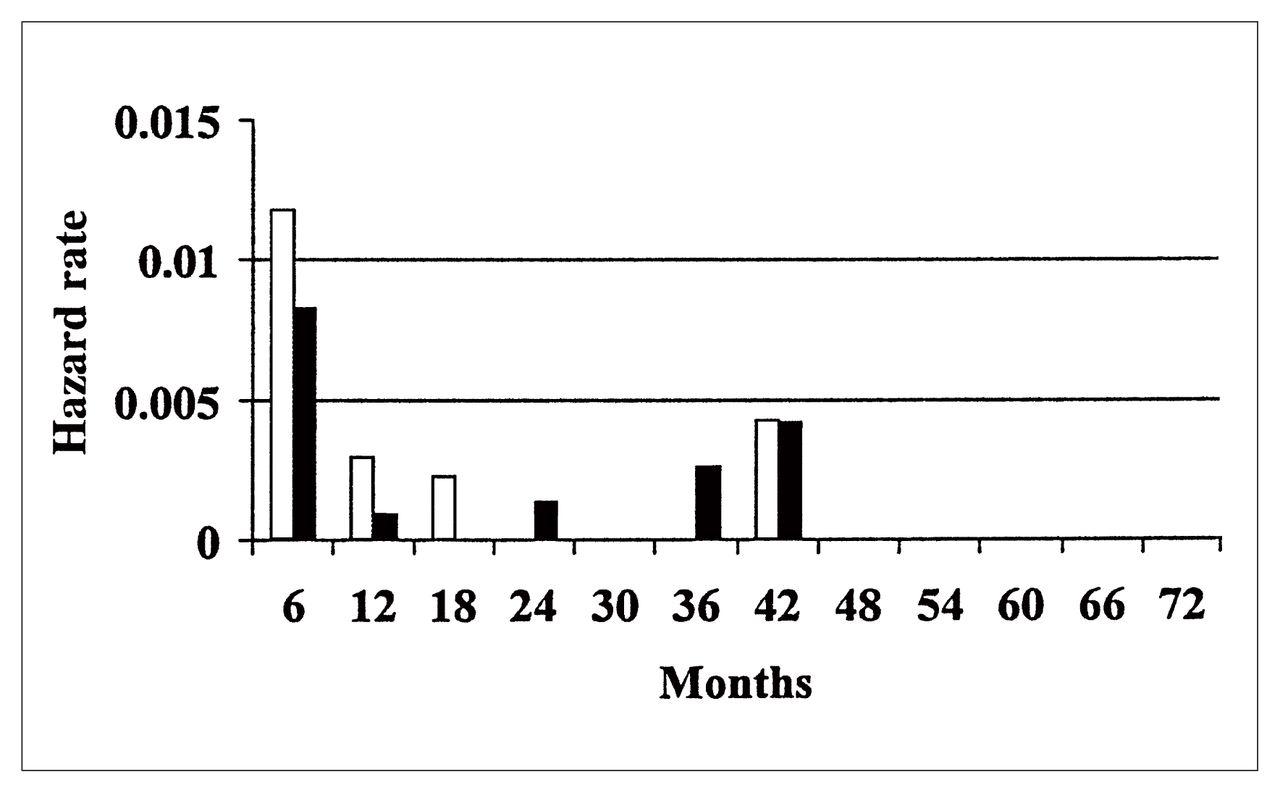
The hazard function of thromboembolic and hemorrhagic events after AVR in patients 65 years of age and older (group 2). White bars = major thromboembolism, thrombosis, fatal thromboembolism and hemorrhage, black bars = major thromboembolism, thrombosis and fatal thromboembolism, without hemorrhage.
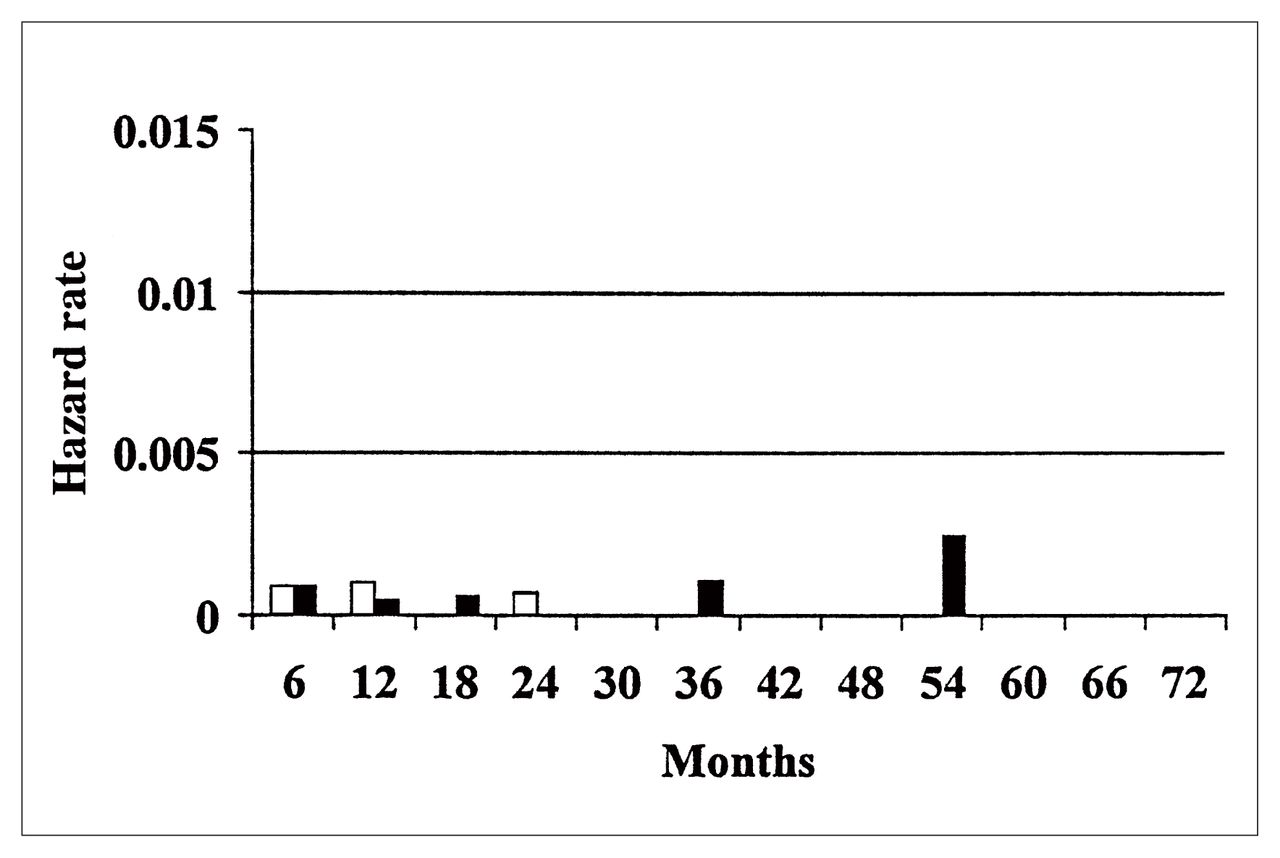
The hazard function of valve-related mortality after AVR and reoperation in group 1 patients. White bars = valve-related reoperation, black bars = valve-related death.
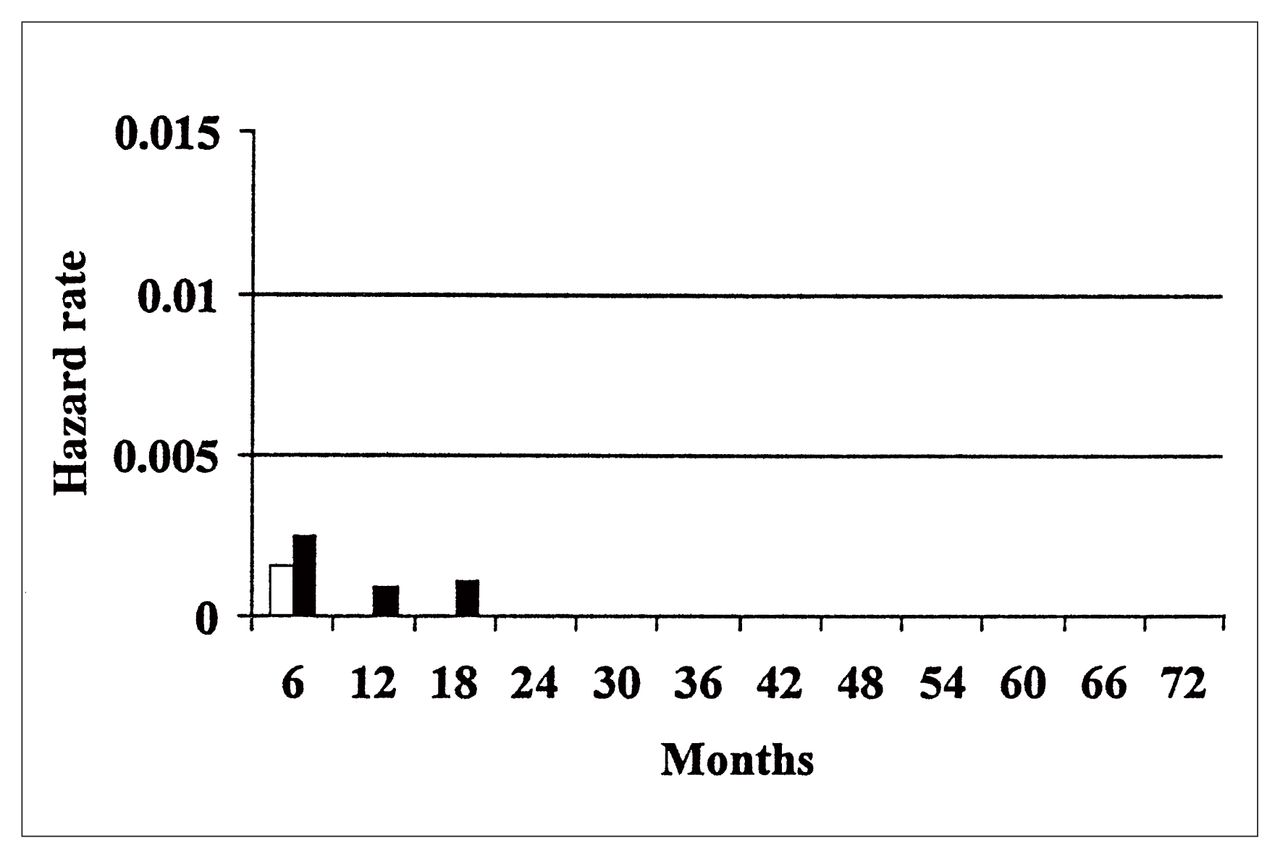
The hazard function of valve-related mortality after AVR and reoperation in group 2 patients. White bars = valve-related reoperation, black bars = valve-related death.
Discussion
The choice of valve substitute for AVR continues to evolve. Mechanical and biological prostheses have been used for 25 years. The choice of biological prostheses over this period has been allografts, for young adults and patients with native or prosthetic valve endocarditis,22 and stented porcine and pericardial bioprostheses for elderly patients over the age of 65 years.19,23–25 The reduced structural valve deterioration with advancing decades of life (at implantation) was first reported from the University of British Columbia in 1988.17 This and subsequent reports by others led to the recommendation that heterograft prostheses be used for AVR in the elderly. 17,23,25 The past 5 to 8 years has seen a resurgence of the pulmonary autograft for aortic root replacement in younger patients, especially children, for whom growth potential is of the utmost importance.26 Stentless porcine bioprostheses have recently been released and are currently being implanted in the elderly with some liberalization of age requirements.27–30 The favourable hemodynamic performance of the pericardial bioprostheses and the stentless porcine bioprostheses has fostered implantation in small aortic annuli to facilitate regression of left ventricular mass.24,28,31
Mechanical prostheses still predominate for AVR, especially in patients younger than 65 years, although they are also used in patients over 65 years of age for AVR. For the past 18 years there has been a choice of bileaflet and monoleaflet mechanical prostheses formulated from pyrolytic carbon.
Of interest is that our experience with porcine bioprostheses revealed an overall thromboembolic rate of 1.5%/patient-year for AVR.16 The rate of major events was 0.8%/patient-year with a fatality rate of 0.4%/patient-year. There has been no published comparison from our centre of bioprostheses and mechanical prostheses in the elderly with AVR. In an unpublished series of elderly patients with AVR, the linearized rate of major thromboembolism and hemorrhage from anticoagulation with mechanical prostheses was 5.6%/patient-year and with porcine bioprostheses was 1.8%/patient-year. The fatality rates were 1.1%/patient-year and 0.6%/ patient-year, respectively. The current series of elderly patients is essentially the same population with an overall major thromboembolic rate of 3.3%/patient-year and hemorrhage rate of 2.2%/patient-year.
The St. Jude Medical prosthesis has been extensively evaluated, and most recent publications have provided 10-year clinical performance results.1–10 An increasing number of studies on the CarboMedics prosthesis has been published.11–15 One of the primary purposes of our report was to evaluate thromboembolic and hemorrhagic complications with these prostheses in AVR. The reported incidence of thromboembolism with the St. Jude Medical prosthesis ranges from 0.6% to 5.1%/patient-year and for the CarboMedics prosthesis, 0.3% to 1.1%/patient-year.1–3,9,11,13,14 This great variation of clinical performance must be related to extent of follow-up evaluation, adequacy of anticoagulation management and the reporting of events whether overall or only major events. The reporting of events only after 30 days postoperatively obviously influences the incidence of thromboembolism.1–3,4,7,12,13
There is no documented comparison of the performance of mechanical AVR by age groupings at the time of implantation. The limited sample size and duration of follow-up do not support statistical comparison, but the 2 age groupings provide clinically relevant information. The incidence of major thromboembolic events in our experience was 1.54%/patient-year and 3.32%/patient-year, respectively, for groups 1 and 2. There were no documented cases of prosthesis thrombosis, and the major reports on the St. Jude Medical and CarboMedics prostheses have not alluded to thrombosis as a significant problem.
The Guidelines for Reporting Morbidity and Mortality After Cardiac Valvular Operations20 of the Society of Thoracic Surgeons form the basis of reporting of valve-related complications. In 1994, Bodnar and colleagues21 recommended more detailed methodology for reporting thrombosis, embolism and bleeding after heart valve replacement. The current study evaluated events by both reporting methods. The methodology recommended by Bodnar and colleagues was used to document major events occurring after 30 days. The rates of reversible (more than 24 hours to 3 weeks) cerebrovascular thromboembolism after 30 days were 0.21%/ patient-year for patients younger than 65 years and 0.22%/patient-year for patients 65 years of age and older. The rates of major cerebrovascular thromboembolism were 1.13%/patient-year and 1.54%/patient-year for the younger and older age groups respectively. The rates of systemic major thromboembolic complications were 0.10%/patient-year for patients less than 65 years of age and 0.22%/ patient-year for patients 65 years of age and older. The death rates associated with cerebrovascular complications were 0.31%/patient-year and 0.44%/ patient-year for the younger and older age groups, respectively. The hemorrhagic event rates after 30 days, according to Society of Thoracic Surgery Guidelines,21 were 1.55%/ patient-year for those less than 65 years of age and 1.77%/patient-year for those 65 years of age and older.
The major events that occurred within 30 days were evaluated separately because of the significant influence on overall event rates. The major thromboembolic rate (crude) for patients less than 65 years of age was 1.02% and for those 65 years of age and older was 3.73%. Hemorrhagic complications occurring within 30 days were seen only in patients 65 years of age or older (Table III). There were 4 thromboembolic events in the group of patients younger than 65 years and 8 in the group 65 years of age and older. Of the 8 major events in the latter group there were 2 deaths.They were in elderly patients, both 81 years old, on the second and fifth days postoperatively. Both patients were in atrial fibrillation, neither was receiving Coumadin, but 1 was receiving heparin and salicylic acid.
Adequacy of anticoagulation was evaluated for all patients who had thromboembolic events. For patients in hospital in both age groups, all patients (10) were inadequately anticoagulated (INR less than 2.0) at the time of the event. For consideration of events occurring within 30 days all patients in each age group were inadequately anticoagulated. For events occurring after 30 days postoperatively, 45% of those less than 65 years of age and 57% of those 65 years of age or older were inadequately anticoagulated. The anticoagulant status of patients who did not have an event or at times remote from an event was not studied. The cardiac rhythm at the time of the event was atrial fibrillation in 18% and sinus rhythm in 82% of patients.
The 10-year freedom from thromboembolism for the St. Jude Medical prosthesis has ranged from 67% to 97% and from hemorrhage due to anticoagulants from 73% to 93%.1–3,5,6,9 In our study of mechanical prostheses, the freedom from major thromboembolism at 5 years was 95.6% and 90.0% overall and with exclusion of early events and 96.7% and 93.7% for the groups of patients younger than 65 years and patients 65 years of age and older, respectively. The overall freedom from major or fatal thromboembolism and hemorrhage was 90.1% and with exclusion of early events was 91.2% for patients less than 65 years of age; for patients 65 years of age and older, these rates were 87.9% and 92.5% respectively. There was 100% freedom from documented obstructive thrombosis.
The optimal range of anticoagulation for various disease states, as well as the process of maximizing the adequacy of anticoagulation, has received considerable attention in recent years.20,31–38 The recommended range of anticoagulation for patients with mechanical prostheses, INR 3.0 to 4.5, has been questioned in randomized studies.39 The studies have shown that lower intensity anticoagulation provides significant reduction in hemorrhage due to anticoagulants with no appreciable change in the rate of thromboembolism.40–42 In their extensive report, Stein and collaborators37 concluded that anticoagulation to a level of INR 2.5 to 3.5 for current generation bileaflet and tilting disc mechanical prosthetic heart valves is the recommended therapeutic level. In 1994, Hirsh and Fuster43 recommended lowering the INR range of 3.0 to 4.5 to 2.5 to 3.5 for patients with mechanical prostheses. Butchart and colleagues44 evaluated low-level and moderate anticoagulation in a retrospective study with the Medtronic Hall monoleaflet prosthesis and recommended an INR level of 2.5 for AVR and 3.0 for MVR. These authors also recommended adjustments based on an analysis of the stroke risk factor. Butchart33 has also recommended patient-specific and prosthesis-specific anticoagulation. The low thrombogenicity mechanical valves and bioprostheses are recommended in the INR range of 2.0 to 2.5 for AVR and 2.5 to 3.0 for mitral valve replacement (MVR). The INR range of 3.5 to 4.0 for high thrombogenicity mechanical valves (e.g., Starr–Edwards caged-ball prosthesis) is recommended for both AVR and MVR. The recommendation for mechanical valves with severe turbulence, for both AVR and MVR, is 3.0 to 3.5 plus antiplatelet therapy. The Working Group on Valvular Heart Disease of the European Society of Cardiology32 has recommended the optimal therapeutic INR for second generation bileaflet and monoleaflet prostheses for AVR as 2.5 and for MVR as 3.0.
In patients with stroke risk factors, with concomitant coronary artery disease and with early generation turbulent prostheses, the role of antiplatelet therapy with valvular substitutes could be important during the early postoperative period until the sewing ring is endothelialized. Turpie and colleagues45 studied mechanical prostheses and tissue prostheses plus atrial fibrillation or a history of thromboembolism with a high INR level of 3.0 to 4.5 randomized to salicylic acid (100 mg/d), with no differentiation with respect to valve position. Major hemorrhagic events in this well-controlled randomized study revealed a hemorrhage rate of 8.5%/patient-year for the salicylic acid group and 6.6%/patient-year for the placebo group. The authors emphasized major systemic embolism, nonfatal intracranial hemorrhage, death due to hemorrhage or to vascular causes with respective rates of 3.9%/patient-year and 9.9%/patient-year for the 2 groups, but major systemic embolism of 1.6%/patient-year and 4.6%/ patient-year. This study has influenced patient management in some centres, but the study group had extremely high rates of hemorrhage and INR levels above recommended levels for current generation prostheses. The study identified some benefit against embolism with salicylic acid but unacceptable rates of hemorrhage. Previous studies had revealed uncertain benefit from concomitant antiplatelet therapy with anticoagulation in patients with prosthetic valves.40,46,47 The recommendation of Butchart33 with regard to patient-specific indications for concomitant antiplatelet therapy requires further assessment through clinical trials.
Our study provides evidence for consideration of more intense postoperative anticoagulant management and improvement in long-term care. Patients, especially in the older age group, who suffered in-hospital major thromboembolic events, had inadequate anticoagulant management. Since this study ended, we have altered our in-hospital management. Inadequate anticoagulation of patients with long-term thromboembolism has been reported previously.1 The role of patient-controlled home anticoagulation has been reported by Cortelazzo and associates35 and by White and colleagues. 38
Our study also demonstrated the elevation of both thromboembolic and hemorrhagic rates in elderly patients who underwent AVR with mechanical prostheses. Mechanical prostheses have a definite role in AVR surgery in patients younger than 65 years of age but reconsideration must be given to the use of mechanical prostheses in patients 65 years of age and older.
- Accepted December 12, 1997.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.