


Esophageal intramural pseudodiverticulosis (EIP) is an uncommon condition in which submucosal glands within the esophageal wall become dilated and appear as pseudodiverticuli.1 Since the disorder was first described in 1960,2 fewer than 150 cases have been reported in adults.3 Only 12 cases have been described in children.
The diagnostic and pathological features of EIP are well documented,4 but the etiology and pathogenesis are unknown. In children, this rare disorder has been associated with gastroesophageal reflux (GER), corrosive acid ingestion5 and dysmotility. 6 In adults, diabetes and candidiasis are additional associations.4
Although EIP is usually a benign discovery, 3 cases of the perforation of the pseudodiverticuli have been reported in the adult literature.7–9 We describe the first case of a ruptured pseudodiverticulum in a teenager.
Case Report
An 11-year-old boy of East Indian descent presented with dysphagia to solid food and intermittent central chest pain, associated with occasional vomiting and postprandial eructation. Endoscopy at that time showed a proximal esophageal stricture. He was treated with omeprazole (20 mg orally once a day) and cisapride (10 mg orally three times a day) with reasonable symptom relief. He was lost to follow-up until the age of 14 years when he was seen because of recurrent symptoms while off medication. Endoscopy showed concentric rings (trachealization of the esophagus) and evidence of reflux esophagitis, confirmed by biopsy. Dilatation was performed up to 11 mm with Savoury dilators.
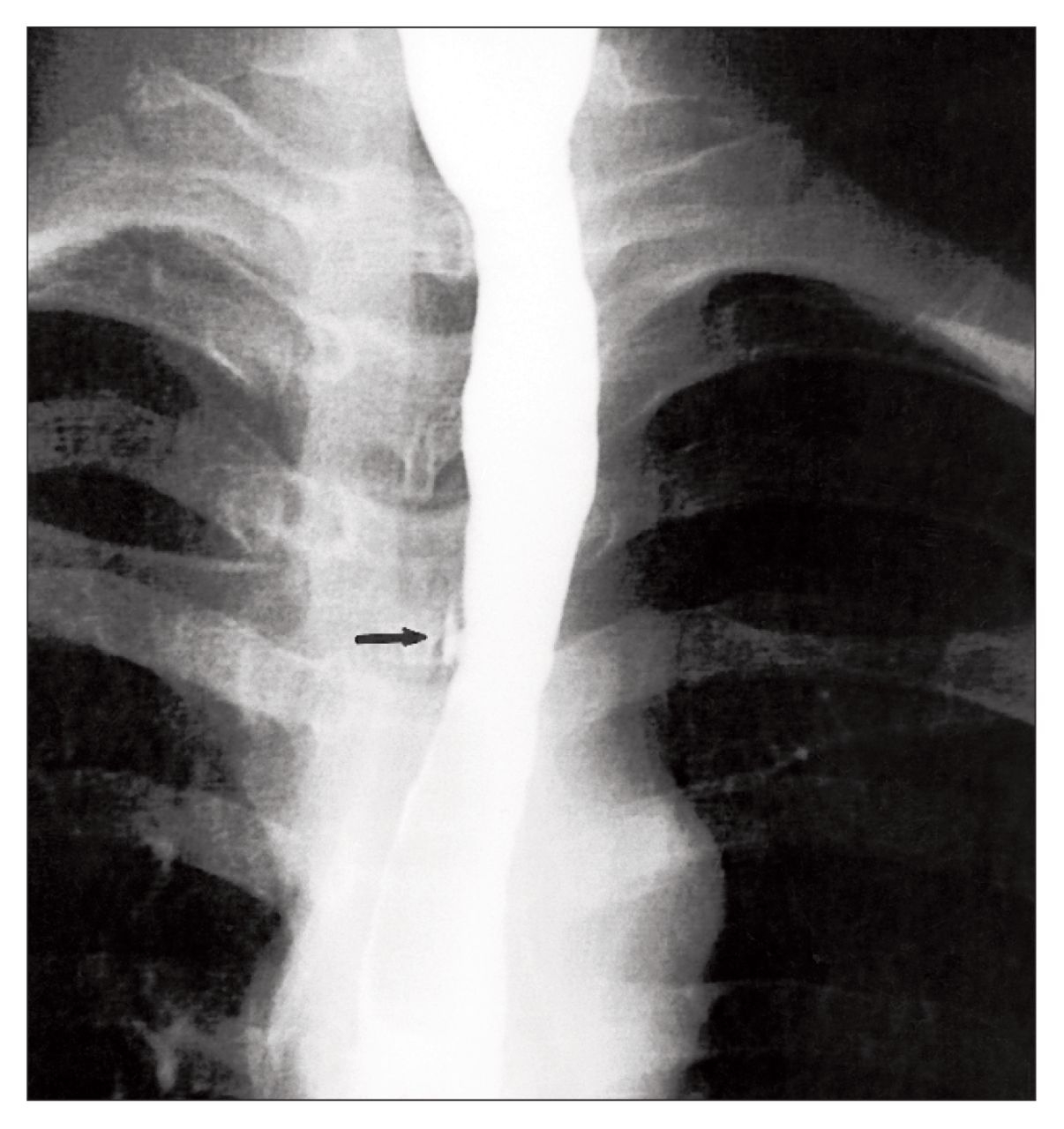
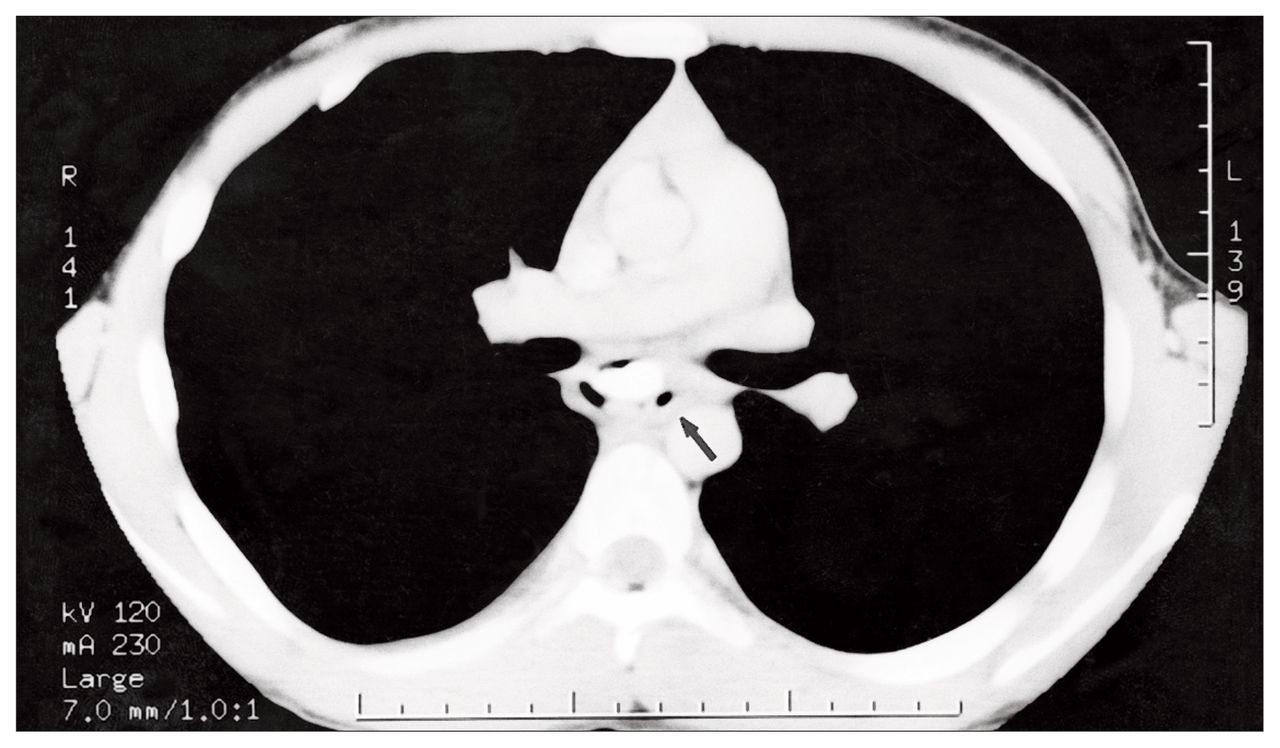
Two months later, he presented with a sudden onset of retrosternal chest pain associated with a dry cough and a temperature of 39.3 °C. He also complained of ongoing dysphagia as well as odynophagia but had not been retching or vomiting. No other abnormalities were found on physical examination. Laboratory studies and chest radiography gave normal results. Ampicillin (1 g every 6 hours), gentamicin (50 mg every 8 hours) and metronidazole (80 mg every 8 hours) were started intravenously. The following day, barium swallow examination showed a small EIP with the characteristic appearance within a long proximal esophageal stricture (Fig. 1). There was longitudinal tracking of barium intramurally with no free leak. An extrinsic mass effect was noted, suggesting local inflammation. Computed tomography of the chest showed mediastinal air from a localized esophageal perforation, which was thought to be secondary to a ruptured EIP with associated peridiverticulitis (Fig. 2). The possibility of a small, contained perforation from the previous dilatation was considered. However, the fact that he had been asymptomatic for 2 months made this unlikely.
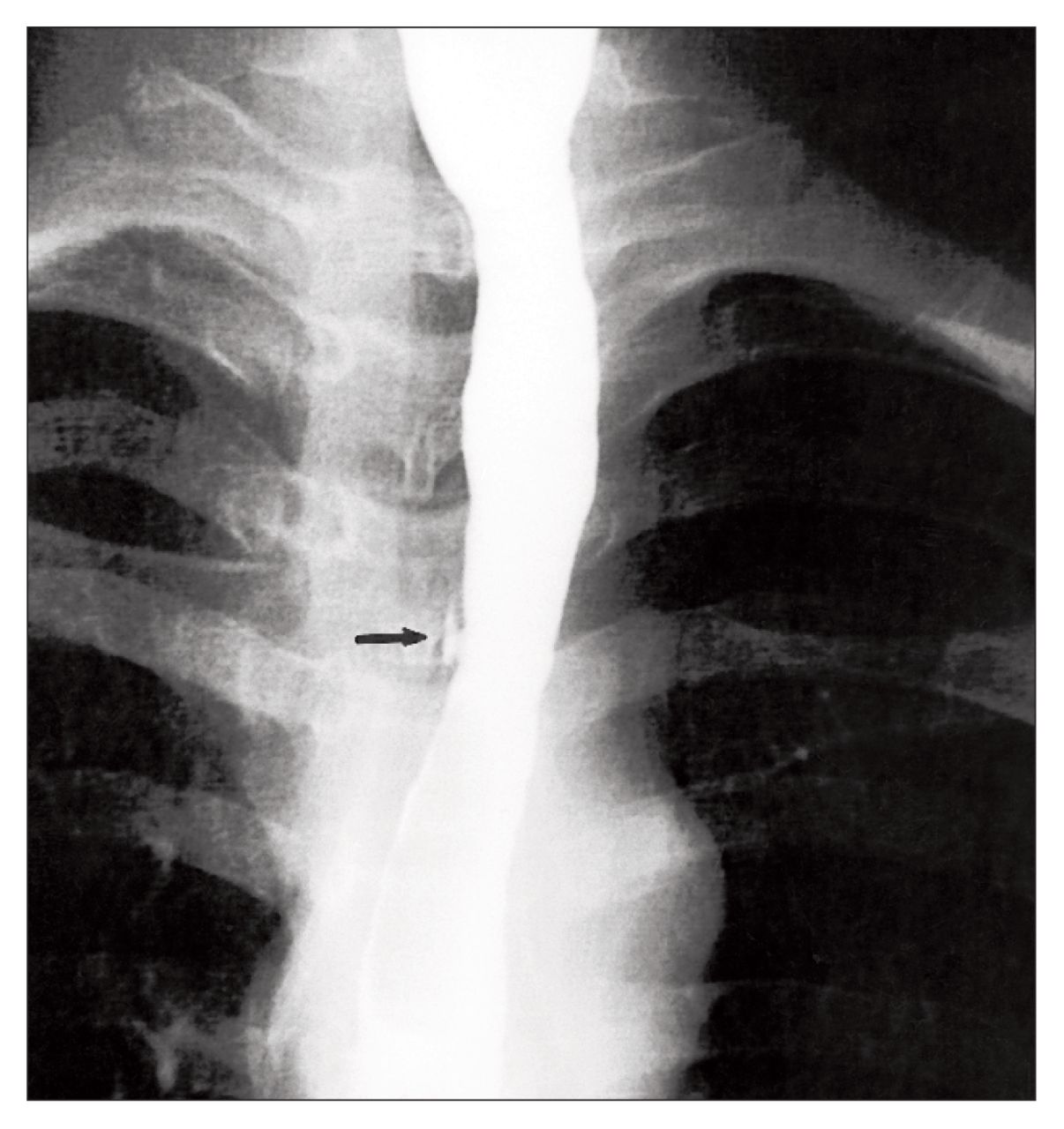
Barium esophagogram shows a long, but mild stricture of the proximal esophagus. An esophageal intramural pseudodiverticulum (arrow) is seen.

Oral and intravenous enhanced CT scan of the chest reveals mediastinal air adjacent to the barium column (arrow).
The patient was started on parenteral nutrition. He responded to medical management with resolution of his fever and chest pain in 2 days. On a repeat barium study 5 days later, the EIP and the extrinsic mass effect were no longer evident. His diet was advanced and he was discharged after 9 days of hospitalization to continue amoxicillin-clavulanate (500 mg orally three times a day) for 1 week and omeprazole (20 mg orally twice a day) in the long term. A repeat barium swallow examination a month later showed the stricture but no EIP. Esophageal manometry and 24-hour pH study (off omeprazole for 4 days) gave normal results.
When the boy was 15 years old, ulcerative colitis was diagnosed. Upper and lower gastrointestinal endoscopy both showed persistent esophagitis and also colitis involving the left colon and transverse colon. At the time of writing, at 17 years of age, his main symptoms are related to his ulcerative colitis.
Discussion
Thirteen cases of EIP (including the present case) have been reported in the pediatric literature (Table I5,6,10–15). The mean age at diagnosis was 11.4 years, with the youngest child being 4 years old. The slight male predominance observed in children is consistent with that in the adult literature.4 The high preponderance of this disorder in East Indian children is skewed by the series of Kochhar and associates5 who reported 14 East Indian patients with corrosive acid-related EIP, 4 of whom were under the age of 18 years.
Summary of Features of 13 Children Who Had Esophageal Intramural Pseudodiverticulosis (EIP)
Four children had feeding difficulty in infancy6,10,14 and 2 had tracheoesophageal fistula repair.13,15 Underlying long-standing GER probably contributed to the development of EIP in these cases. The etiologic role of dysmotility in children, however, has yet to be examined because manometry has seldom been used in children with EIP.6 In adults, up to 77% of those tested revealed abnormalities including aperistalsis, poor contractions, uncoordinated motor activity and an incompetent lower esophageal sphincter.4
Four patients had dysphagia after acid ingestion (1 to 48 months before presentation) and had evidence of EIP. Acid-induced esophagitis followed by healing and fibrosis leads to stricture formation and possible shortening of the esophagus. This may result in the development of GER and chronic esophagitis, which predisposes to the formation of EIP. Candidiasis and diabetes have been associated with EIP in adults,4,5 but much less so in children.6,10
An esophageal stricture was found in all children regardless of the presence of GER or a history of acid ingestion. This finding suggests that chronic esophagitis represents the common pathway in the development of EIP. The stricture is only a part of the disease process rather than the cause of EIP, as its anatomic relationship to EIP is not constant (Table I). Paradoxically, EIP has been seen in adults without a stricture.1,2
GER has been reported in 5 children with 1 associated hiatus hernia,12,13,15 but the diagnostic modalities for GER were not clearly indicated in these cases. Our patient had clear endoscopic evidence of GER (concentric rings) as well as biopsy-proven reflux esophagitis. There was no history of caustic ingestion. The normal 24-hour pH study done at only 4 days off omeprazole might be due to partial acid suppression. A proper study for a child of this age would require 10 days without omeprazole.
Barium swallow examination offers the most sensitive method of diagnosis. The appearance of pin-head sized outpouchings projecting perpendicularly from the mucosal surface is pathognomonic.4 An interesting observation was made in previous reports that the appearance of the EIP would become less obvious11 and the number of cases of EIP would decrease10 with time. In our patient, with proper treatment, the EIP disappeared in the repeat barium study. CT may be of value in making the diagnosis, as it was in our case. Typical findings on CT consist of intramural gas collections with associated wall thickening and mucosal irregularity.16
Endoscopy was performed in less than 50% (6 of 13) of the children and showed esophagitis (4 children) and strictures (5 children). Ostia of the dilated glands were seen in only 2 patients.13,15 This direct endoscopic evidence of EIP was observed infrequently (17%) in adults.4 The ostia on the mucosal surface correspond to the main excretory ducts of the dilated esophageal submucosal glands, which are lined by stratified squamous epithelium. In most cases, acute or chronic inflammation, or both, are noted, presumably causing ductal obstruction leading to subsequent dilatation of the glands and squamous metaplasia. In uncomplicated cases, these dilated glands do not penetrate the muscularis propria. Endoscopic mucosal biopsies were non-diagnostic because of the submucosal location of the EIP.6,10,12,15
Treatment of EIP should be directed toward the underlying cause to prevent further damage and should deal with complications. In the 12 children reported previously (Table I), 6 underwent dilatation of the stricture, 1 had dilatation and fundoplication, 1 had colonic interposition bypass. Three children had no treatment; 2 of them had no complications during a long follow-up.14,15 Although not mentioned in any of the cases, GER or esophagitis should be treated aggressively. Our patient underwent dilatation and received medical therapy for GER. Because of difficulty in obtaining medical control of his ulcerative colitis, fundoplication has not been performed since his esophagitis is currently not his main problem.
Only 3 cases of perforation of EIP have been reported.7–9 All were in adults older than 50 years. The 2 patients with mediastinitis were treated successfully with antibiotics. 7,9 Kim and associates8 reported a 67-year-old man who underwent a subtotal esophagectomy for a distal esophageal mass that was actually a periesophageal abscess from a perforated pseudodiverticulum.
Our case appears to be the first one of perforation of EIP with associated mediastinitis in a child. Despite the potential morbidity and mortality, the patient recovered successfully with conservative therapy. Unlike other forms of esophageal perforation, that from a ruptured EIP is likely microscopic and is sealed off relatively rapidly by the surrounding tissue reaction. Contamination is therefore limited, thus allowing adequate control with antibiotics alone. It is apparent that pediatric EIP is most likely a result of long-standing chronic esophagitis. The etiology of the esophagitis should be identified and aggressive treatment should be instituted to avoid possible progression to perforation.
- Accepted July 27, 1998.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.