


Although surgically correctable hypertension is usually related to renovascular stenosis from atherosclerosis or fibrodysplasia, other disorders should also be considered in any differential diagnosis. This case report summarizes 2 such uncommon causes: Takayasu’s disease and coarctation of the abdominal aorta. These disease processes are contrasted in the context of surgically correctable hypertension.
Case report
History and physical examination
A 35-year-old woman presented with fatigue, dysphoria and a blood pressure of 215/115 mm Hg. Initial assessment revealed arteriovenous nicking of the fundal vessels, absence of papilledema and normal findings on neurologic examination. She was admitted for control of her hypertension. Subsequently, she suffered a right hemispheric cerebrovascular accident, consisting of left hemiparesis and sensory loss, with neurologic defects involving left cranial nerves VII and XII. There were no recorded episodes of hypotension. Other physical findings included diminished femoral pulses and bruits of the abdominal and subclavian arteries. There were no carotid artery bruits. Although she had been treated for systemic hypertension during early adolescence, she was not compliant and had discontinued her antihypertensive medications after a short period. She was on no medication at the time of presentation.
Investigations
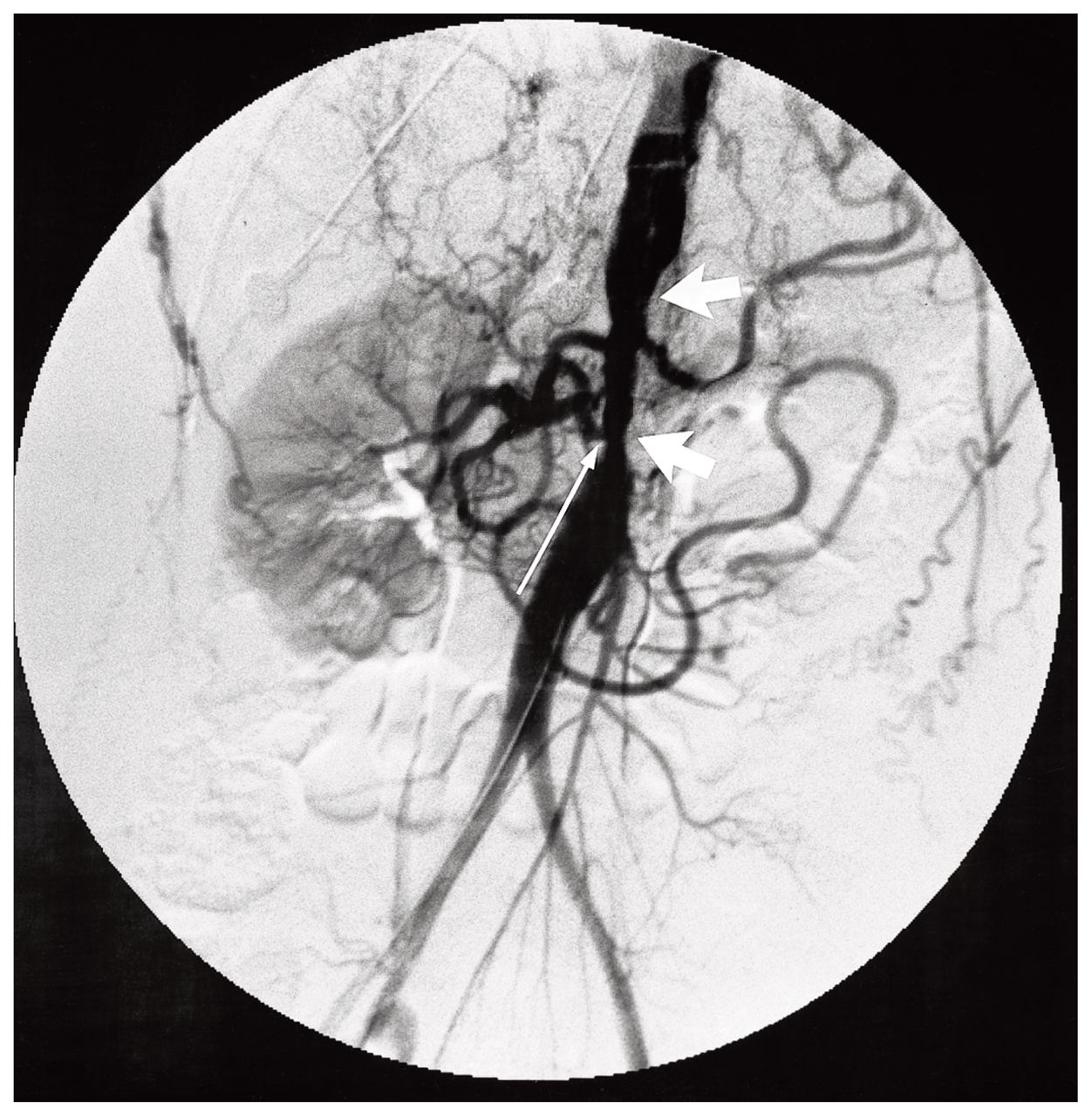
Cerebral computed tomography demonstrated hypodense lesions of the right putamen and capsule consistent with infarction. Angiographic studies demonstrated multiple stenotic lesions of the intracranial carotid and middle cerebral arteries consistent with atherosclerosis, and stenosis of the proximal right subclavian artery, abdominal aorta and the renal arteries (Fig. 1). The extracranial carotid arteries and thoracic aorta were normal. Kidney size was normal. The origins of the celiac and superior mesenteric arteries were involved in the disease process. An immunologic work-up gave negative results (Table I).
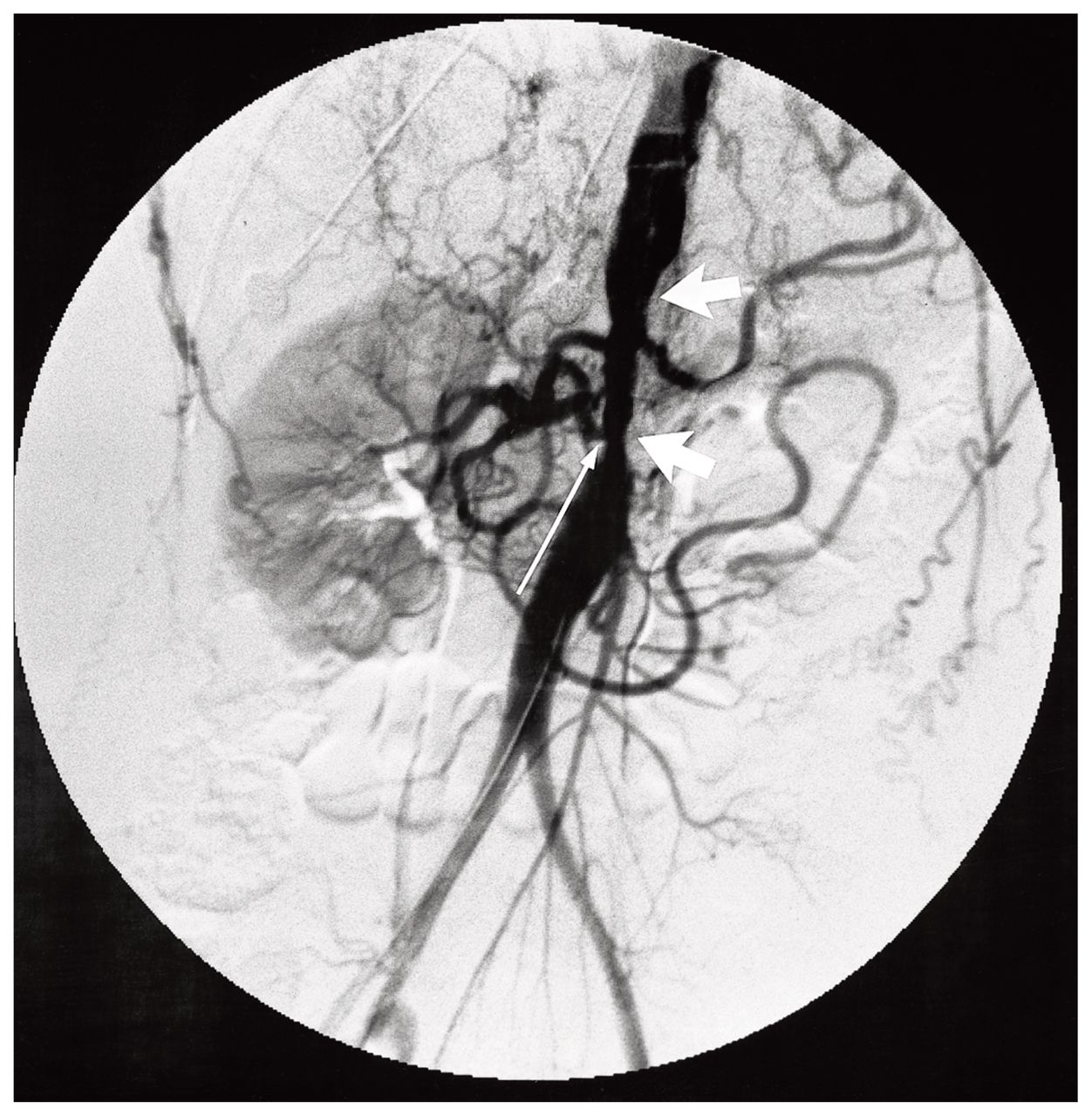
Angiography shows stenosis of the abdominal aorta (short arrows) and renal arteries (long arrow).
Results of Immunologic Investigations in a Patient Who Had Hypertension Suggestive of Takayasu’s Disease
Treatment
The patient’s hypertension was managed with intravenously administered labetalol followed by oral medication (nifedepine and atenolol). High-dose parenterally administered steroids, initially begun for a presumed diagnosis of Takayasu’s disease, were discontinued after it was decided that there was insufficient evidence for a diagnosis of acute arteritis. The patient eventually recovered all sensory and most motor function. She walked with mild disequilibrium.
During convalescence, excess renal potassium excretion was attributed to bilateral renal artery stenosis. Surgical intervention was indicated to control her renovascular hypertension, preserve renal function, prevent mesenteric ischemia and subsequent cerebrovascular accident and for peripheral problems related to her aortic stenosis. The coarctation of the abdominal aorta was demonstrated at operation (Fig. 2). A full-thickness aortic wall biopsy was done. Vascular reconstruction consisted of a thoracic-to-abdominal aortic bypass, with celiac, superior mesenteric and renal artery revascularization.

Operative view shows coarctation of the aorta (Ao) (short arrow). The long arrow demonstrates the left renal vein.
Follow-up
The aortic biopsy demonstrated chronic atherosclerotic occlusive disease. There was no pathological evidence of Takayasu’s disease (Fig. 3). The patient recovered without incident. She had normal renal function and was able to discontinue all antihypertensive medication.

Biopsy of the aorta. Small black arrows indicate the intima and the thick black arrow the outer media. The open arrows point to the adventitial surface. The biopsy demonstrates nonspecific intimal thickening with an absence of significant acute or chronic inflammatory changes or fibrosis (hematoxylin–eosin stain, original magnification × 100).
Discussion
Surgically correctable hypertension resulting from atherosclerosis or fibromuscular dysplasia of the renal arteries had been reviewed elsewhere.1,2 Abdominal aortic coarctation and Takayasu’s disease are uncommon causes of surgically correctable hypertension. The prevalence of both in North America and Europe is estimated to be 1 to 5 per million people.3–5 The etiology for each condition remains disputed. Historically, abdominal coarctation was attributed to a congenital lesion. However, the incidence of true aortic hypoplasia leading to coarctation may be considerable less than believed.6 Abdominal coarctation might represent the end-point of a number of disease processes, including rubella infection, nonspecific arteritis, Takayasu’s disease, neurofibromatosis, radiation therapy and atherosclerosis.7 The etiology of Takayasu’s disease, an autoimmune arteritis of the aorta and its main branches, also remains unknown. Viral and tuberculous infections, genetic and hormonal etiologies have been suggested.5,8,9
Abdominal aortic coarctation generally presents during the second or third decade of life with severe renovascular hypertension. 5 Recent series do not support any previously recognized specific race or gender distribution.10,11 A clinical triad of a thoracoabdominal bruit, diminished femoral pulses and hypertension is typical.6 Morbidity is primarily related to life-threatening stroke and congestive heart failure, resulting from severe uncontrolled hypertension. Less common clinical manifestations include claudication, angina, myocardial infarction, intestinal ischemia and renal failure.
Takayasu’s disease usually presents before the age of 40 years. There is a strong female predominance.5 The early disease phase is characterized by nonspecific symptoms such as fatigue, headache, malaise, arthralgia, myalgia and fever. Rarely, a patient will present in the acute phase with localized arterodynia, hypertension, bruits or asymmetric upper extremity blood pressures. In most patients, Takayasu’s disease is recognized in its chronic phase, with or without a history of systemic illness. Symptoms are related to the arteriopathies: hypertension, retinopathy, renal failure, extremity ischemia and visceral ischemia. Cerebrovascular accident from carotid artery occlusive disease or severe hypertension can occur.12 Proximal aortic or coronary artery disease can result in angina or myocardial infarction.
Angiography for abdominal coarctation demonstrates focal or diffuse occlusive disease along the length of the abdominal aorta. Renal artery involvment has been described in 80% of all cases.10,13 The mesenteric vessels are also often involved. 13 Takayasu’s disease is suggested by history, confirmatory immunologic investigation and an angiographic picture of occlusive or aneurysmal disease of the entire abdominal and thoracic aorta in association with subclavian and extracranial carotid artery occlusive lesions. Focal disease is uncommon.5 An elevated erythrocyte sedimentation rate is almost invariably found in the acute phase of the illness.14 Other nonspecific immunologic serum markers in Takayasu’s disease include antinuclear antibody, complement C3/C4, rheumatoid factor and antineutrophil cytoplasmic antibody. Arterial biopsy may help confirm the diagnosis.
Both abdominal coarctation and Takayasu’s disease require aggressive treatment in the third or fourth decade of life to prevent the sequelae of severe hypertension: stroke and congestive heart failure. The treatment of abdominal coarctation is usually surgical with acceptable morbidity and mortality.11,15 Repair of abdominal coarctation involves bypass of the involved aorta with renal and mesenteric revascularization. Isolated renal artery involvement has been treated with percutaneous balloon angioplasty. In contrast, treatment of Takayasu’s disease in the acute phase is directed to control of systemic symptoms and inflammation of the arteries. High-dose parenterally administered corticosteroids are usually effective for the symptoms and to halt progression of disease. Adjuvant immunologic therapy is occasionally necessary.5 Surgery is generally reserved for complications of Takayasu’s disease. Operation should be avoided during the acute phase, and vascular anastomoses should not be made in diseased segments of arteries. Surgical bypass of occlusive lesions from uninvolved aorta to the subclavian, carotid, renal and mesenteric arteries has been reported with morbidity and mortality comparable to bypass for atherosclerotic disease.12,13 Treatment of carotid, renal and peripheral occlusive lesions can prevent subsequent morbidity from the arterial lesions.6
The pathologic features of abdominal coarctation are not specific to the underlying etiologic factors. There is narrowing of the internal and external diameter of the aorta with nonspecific intimal hyperplasia. 16,17 The histologic features of Takayasu’s disease depend on the disease phase. Active lesions are characterized by dense granulomatous vasculitis with an intimal lymphocytic infiltrate and by the presence of Langhan’s and foreign body giant cells. Chronic lesions reveal a paucity of inflammatory cells with extensive transmural sclerosis, resulting in fixed occlusive lesions. Neither of these histologic findings of Takayasu’s disease is seen in abdominal aortic coarctation. Fibrotic arterial involvement is seen in the lesions of all patients with chronic phase Takayasu’s disease.16
Table II compares the important clinical, laboratory and pathologic findings of coarctation of the abdominal aorta and Takayasu’s disease.
Comparison of Clinical and Laboratory Characteristics of Abdominal Aortic Coarctation and Takayasu’s Disease
Final diagnosis
Our patient presented with an acute cerebrovascular accident as a complication of chronic, uncontrolled hypertension. The onset of hypertension occurred during early adolescence and was not associated with systemic illness. Immunologic investigation at this presentation provided no evidence of an acute inflammatory process. Angiography of the intracranial carotid circulation revealed multiple stenotic lesions consistent with chronic hypertensive changes. A mild stenosis of the right proximal subclavian artery was present; however, the extracranial carotid arteries were normal. The thoracic aorta was spared, but severe abdominal aortic occlusive disease was present with involvement of both renal arteries, the celiac axis and the mesenteric arteries.
The early age of onset of hypertension without systemic illness, the absence of serum immunologic markers and the sparing of the thoracic aorta and carotid arteries suggest a diagnosis of abdominal aortic coarctation over Takayasu’s disease. Additional information weighing against a diagnosis of Takayasu’s disease in this case was the absence of the characteristic acute or chronic histologic changes on full-thickness aortic wall biopsy.
Conclusions
Coarctation of the abdominal aorta and Takayasu’s disease are uncommon causes of surgically correctable hypertension. Both occur in young patients and if left untreated result in significant morbidity and mortality related mainly to cerebrovascular disease and congestive heart failure. Although similar in their presentation, distinction between these conditions may be possible, based on history, physical examination and radiologic findings. Surgical intervention is indicated for control of hyperetension, prevention of cerebrovascular accident and preservation of cardiac and renal function.
Footnotes
Presented at the annual meeting of the Canadian Society for Vascular Surgery, Halifax, NS, Sept. 29, 1996.
- Accepted November 26, 1997.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.