


Abstract
Objective: The aim of the study was to evaluate the technical feasibility and the postoperative course of aortic valve replacement through a ministernotomy.
Setting: The Montreal Heart Institute and the Hôpital Lariboisière, Paris, France.
Design: A case series from 2 institutions.
Patients: Fifty-one patients who underwent aortic valve replacement through a ministernotomy. The sternal incision was started at the level of the sternal notch extending down to the third or fourth intercostal space with a transverse section of the sternum at this level on both sides or limited to the right side (inverted T or L incision). Thirty-nine patients had aortic stenoses, 6 patients were operated for aortic insufficiency and 6 had mixed disease. The mean (and standard deviation) preoperative left ventricular ejection fraction was 0.56 (0.17).
Main outcome measures: Cardiac bypass time, complications and outcome.
Results: The patients received Carbomedics and St. Jude mechanical valves, Hancock and Carpentier–Edwards bioprostheses. Thirty-eight patients were administered antegrade and retrograde cardioplegia, 10 patients antegrade and 3 retrograde blood cardioplegia only. The mean (and standard error) cardiopulmonary bypass time and aortic cross-clamp time were 104 (38) minutes and 72 (16) minutes respectively. Two patients (4%) died and 2 patients (4%) showed evidence of a stroke after the procedure. Hospital stay averaged 8 (5) days.
Conclusion: We conclude that aortic valve replacement can be done through a ministernotomy approach with perioperative results similar to those obtained through a conventional sternotomy.
Minimally invasive procedures are currently being evaluated in many aspects of heart surgery. Pressure from percutaneous intervention methods and patient requests for less-invasive procedures have brought a new concern to the surgeon: How long a skin incision and thoracic opening are necessary to safely carry out cardiac surgical procedures? Minimally invasive approaches to aortic valve surgery have been previously described. 1–3 We believe that the approach to aortic valve surgery must avoid cannulation of the groin for cardiopulmonary bypass. A left ventricular vent and a retrograde cardioplegia cannula must be inserted. With these considerations in mind, we believe that maximal chest wall integrity can be maintained with a ministernotomy approach.
The objective of this study was to evaluate the feasibility of replacing aortic valves through a ministernotomy at the Montreal Heart Institute and at the Hôpital Lariboisière, Paris, France.
Patients and Methods
Study population
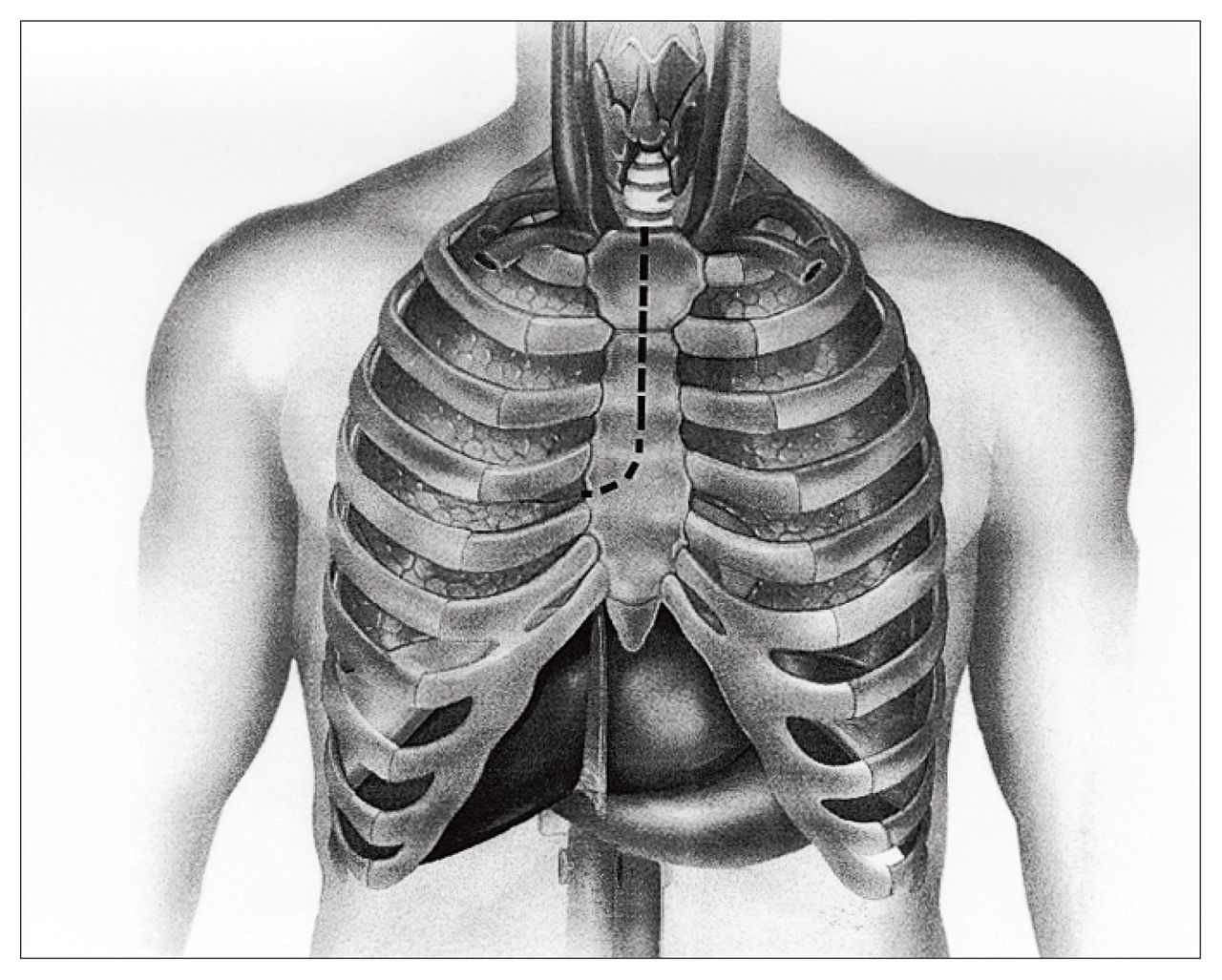
From January 1996 to January 1999, 51 patients underwent aortic valve replacement with a partial sternotomy. Forty consecutive, urgent and elective patients were operated on at the Montreal Heart Institute by 3 surgeons and 11 patients at the Hôpital Lariboisière, in Paris, by 1 surgeon. The differences in operative technique compared with the standard operative approach to aortic valve surgery were mainly the skin and the sternotomy incisions. Twenty-eight patients had a hemisternotomy incision, the shape of an inverted T at the level of the third intercostal space, with care not to damage the internal thoracic arteries (Fig. 1). One patient had the inverted T incision carried down to the fourth intercostal space to allow an additional aortocoronary bypass graft to be placed on the left anterior descending artery. Twenty-two patients had an inverted L incision carried down to the level of the right fourth intercostal space, which allowed right coronary artery bypass grafting in 2 patients (Fig. 2).
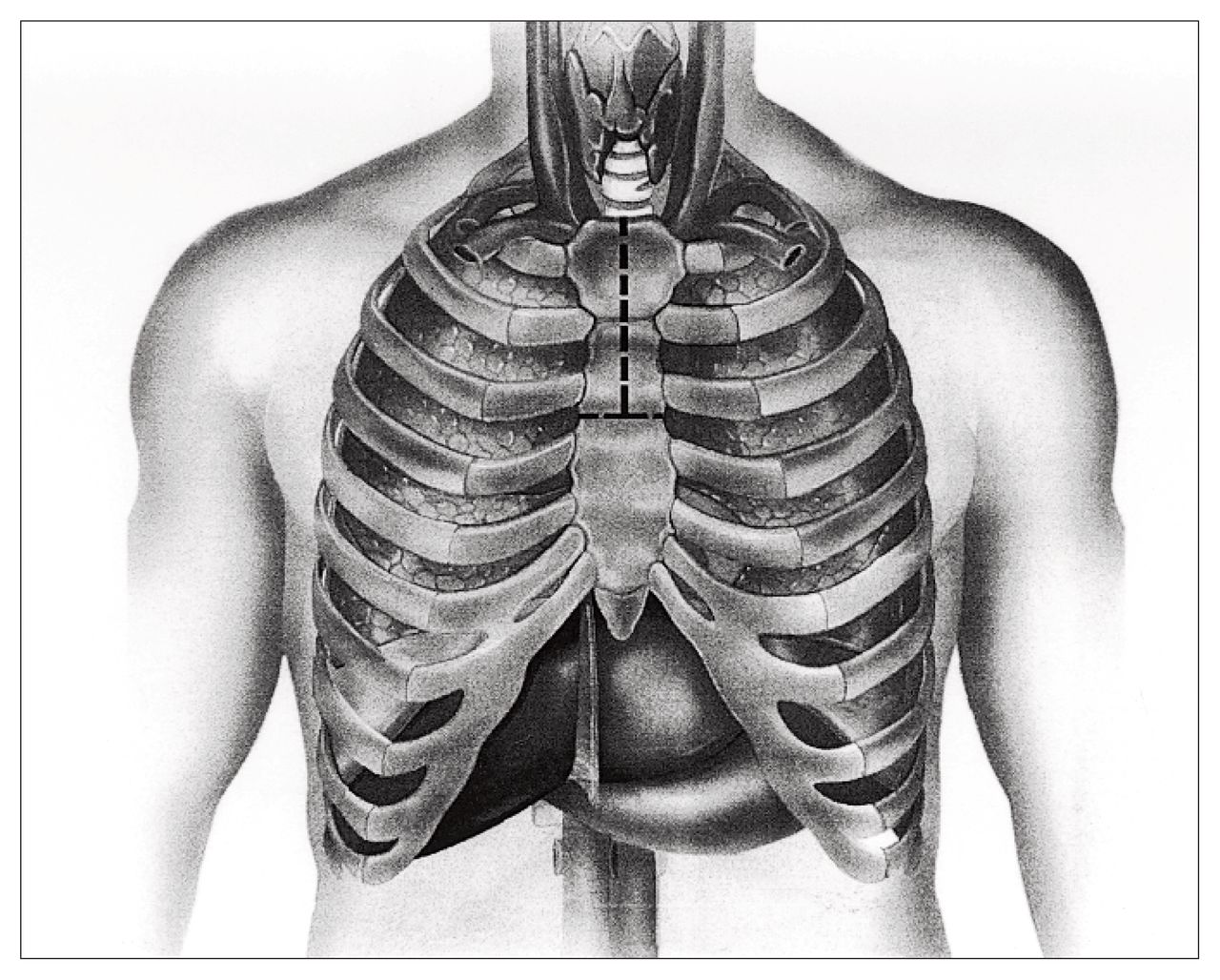
Hemisternotomy with an inverted-T incision.

Hemisternotomy with an inverted-L incision.
The mean (and standard deviation) age of the patients was 65 (13) years. Thirty-nine patients (76%) underwent aortic valve replacement for aortic stenosis, 6 patients (12%) had aortic insufficiency, 6 (12%) had mixed disease. One patient (2%) underwent aortic valve repair because of endocarditis. Carbomedics and St. Jude mechanical valves, Hancock and Carpentier–Edwards bioprostheses were implanted, and saphenous veins were used for aortic valve replacement in 3 patients. Thirty-eight patients had antegrade and retrograde cardioplegia, 10 patients had antegrade cardioplegia only and 3 had retrograde cardioplegia only. The mean (and standard deviation) preoperative left ventricular ejection fraction was 0.56 (0.17) (range from 0.20 to 0.70) (Table I).
Characteristics of the 51 Patients Who Underwent Aortic Valve Replacement Through a Ministernotomy
Surgical technique
External defibrillation paddles were fixed on the skin, and a transesophageal echocardiographic (TEE) probe was inserted. A midline skin incision 6 to 8 cm long, starting 1 to 2 cm inferior to the sternal notch was followed by a partial midline sternotomy extending to the third to fourth intercostal space. The incision was completed by a transverse sternotomy (inverted T) or a transverse sternotomy limited to the right hemisternum (inverted L). The pericardium was opened and fixed for suspension on both sides of the wound. The ascending aorta was cannulated as was the right atrium via the atrial appendage. A retrograde cardioplegia cannula was inserted by pulling lightly on the right atrium and inserting it blindly over a guide. Correct positioning was confirmed by the return of highly desaturated blood or by the pressure wave curve.
After cross-clamping of the ascending aorta, a left ventricular vent was inserted through the right superior pulmonary vein. Antegrade cardioplegia was initiated, followed by retrograde cardioplegia once cardiac electrical activity had stopped. Cold or tepid blood cardioplegic solution was used. Aortic opening, valvectomy and aortic valve replacement were done according to standard surgical techniques. After the ventricular cavities were filled, with partial occlusion of the venous return and lung ventilation, air was withdrawn from the aortic root through a needle connected to suction. This was continued until the transoesophageal echogram showed adequate “de-airing” of the left ventricle.
Once hemostasis was complete, 2 drains of the Jackson–Pratt type were inserted in the pericardium and brought out suprasternally in our early experience (first 19 cases). Later in the study, more extensive drainage with 2 sump drains was used to evacuate blood from the pericardium more effectively. The sternum was closed with steel wires, and an additional wire was used to fix the superior and inferior portions of the transverse sternal incision.
In all patients, aortic and right atrial cardiopulmonary bypass cannulas and left ventricular vents were inserted through the right superior pulmonary vein via the ministernotomy incision. Thirty-four patients had successful placement of a retrograde cardioplegia cannula.
Results
Mean (and standard deviation) cardiopulmonary bypass and aortic cross-clamp times were 100 (29) minutes and 70 (14) minutes respectively. All patients underwent aortic surgery through a ministernotomy approach. Two patients underwent full sternotomy in the immediate postoperative period, during re-exploration for bleeding. One of these patients had ventricular fibrillation during transport to the intensive care unit, with immediate reoperation for a periprosthetic leak, which was identified at transoesophageal echocardiography. This was the only patient with a periprosthetic leak at postoperative echocardiography.
Two patients (4%) died, one after sudden ventricular arrhythmia secondary to malfunction of an external pacemaker 4 days after uncomplicated aortic valve replacement and another from left ventricular failure with severe ventricular dysfunction and preoperative clinical class IV (New York Heart Association classification) before surgery.
Two patients (4%) with tamponade underwent drainage of a pericardial effusion in the immediate postoperative period. Six patients (12%) had serum creatine kinase-MB isoenzyme levels higher than 100 IU 24 to 48 hours after surgery without new Q waves on electrocardiography. One episode of transient ischemic attack and a stroke occurred with the onset of atrial fibrillation 5 days after surgery. Another patient suffered a hemorrhagic stroke of the left thalamus 4 days postoperatively. Hospital stay averaged 8 (5) days (median 7 days).
The mean (and standard deviation) actuarial survival 24 months after valve replacement was 91% (4%). Preoperatively, 22 patients (43%) were in NYHA functional class III and 23 (45%) patients were in class II, and of the survivors at 16 (9) months’ follow-up, 28 (61%) were in class I and 17 (37%) were in class II.
Discussion
The early clinical results with ministernotomy for aortic valve surgery suggest that this approach is technically safe. Cardiopulmonary bypass and aortic cross-clamp times were similar to those reported by conventional techniques at both institutions. Although these patients were among our initial experience with the technique, hospital mortality and morbidity remain related to well-recognized risk factors for aortic surgery. Moreover, some changes in the ministernotomy approach were beneficial to decrease early morbidity. The sternal incision is now extended to the fourth intercostal space with a J curve to the right sternum, which greatly facilitate exposure of the right atrium and retrograde cannulation of the coronary sinus. The pericardium is drained with standard chest tubes to eliminate early pericardial effusion and tamponade, complications that did not occur with the use of sump drains.
Of utmost importance is the monitoring of left ventricular “de-airing” by transesophageal echocardiography and a vent in the ascending aorta, the use of cutaneous defibrillator paddles and careful cannulation of the coronary sinus for retrograde blood cardioplegia. In some difficult cases, preoperative insertion of the retrograde catheter under fluoroscopic or echocardiographic guidance could also be considered.
By extending the sternal opening to the fourth or even the fifth intercostal space it appears possible to add coronary artery bypass grafting to the aortic valve surgery. In the present study, 3 patients had coronary artery bypass grafting with saphenous vein grafts to the right coronary and the left anterior descending arteries.
Several authors1,4–6 have proposed new and innovative approaches to valve surgery. Cosgrove and associates1 suggested first a right parasternal incision and then favoured a ministernotomy. Gundry and associates4 advocated the use of a ministernotomy in all valve operations in adult patients. Although they used an inverted-T ministernotomy, a J-shape sternal incision toward the right fourth or fifth intercostal space gives a better exposure of the right atrium and the possibility of access to the right coronary artery for coronary artery bypass grafting if needed.5,6
The advantages of a ministernotomy for aortic valve surgery are access to all great vessels for cannulation and surgery through the minimal incision and the use of surgical techniques and instrumentation that are familiar to all cardiac surgeons. Although we have shown that the technique is safe and reliable, benefits in terms of pain reduction, shorter hospital stay and faster recovery time for patients remain to be documented.
- Accepted March 2, 1999.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.