


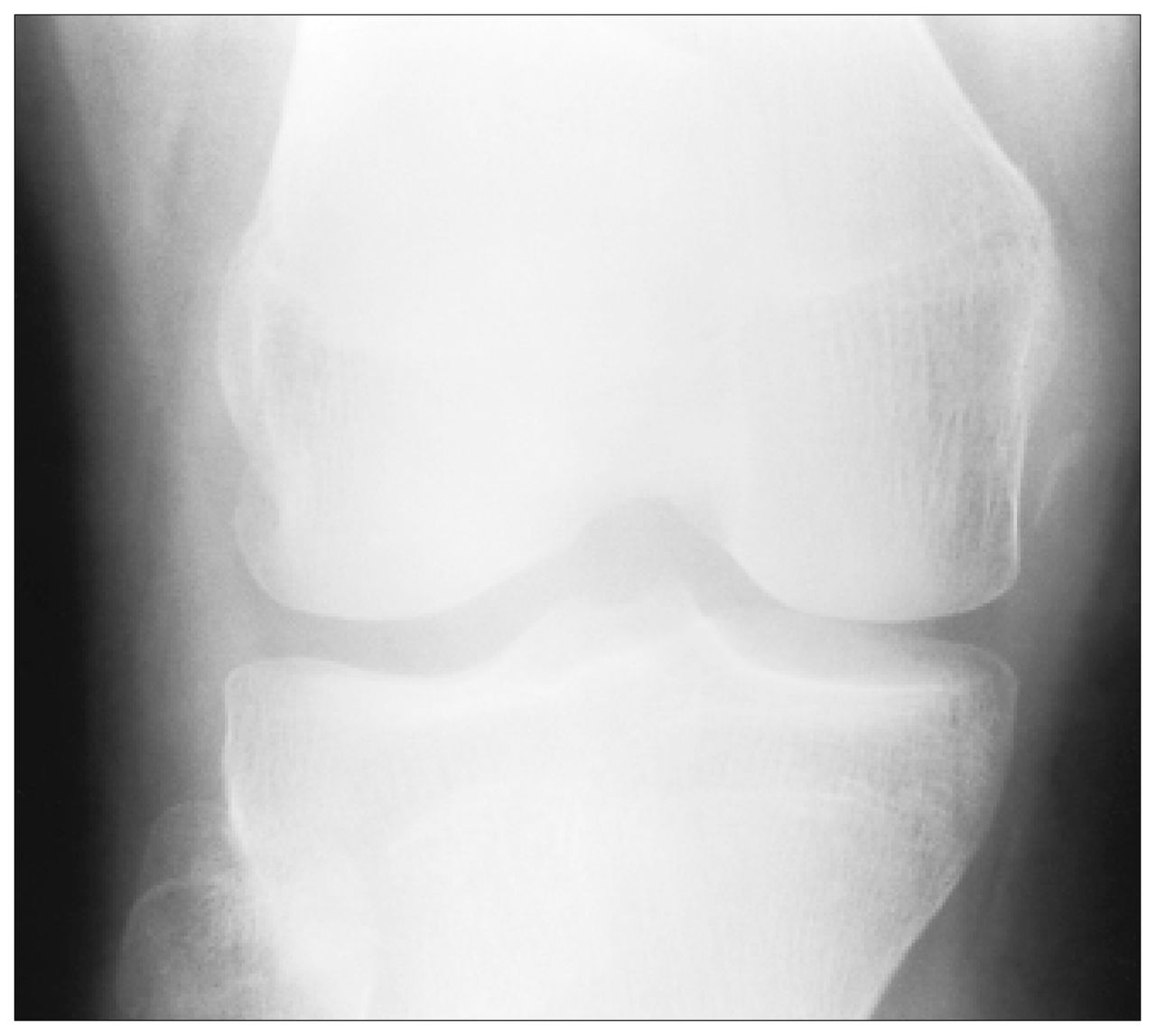
While playing volleyball, an 18-year-old man fell and twisted his right knee. The knee became acutely swollen. On examination at the hospital full clinical assessment was limited because of the swelling. A plain x-ray film confirmed the soft-tissue swelling and revealed an ossified fragment medial to the medial femoral condyle on the anteroposterior view (Fig. 1). Magnetic resonance imaging (MRI) was done to look for possible internal derangement, including disruption of the medial collateral ligament. MRI demonstrated intact menisci, cruciate ligaments and medial collateral ligament but secondary signs of patellofemoral dislocation. Axial images demonstrated lipohemarthrosis and an osteochondral defect of the medial patella, and bone bruises of the lateral femoral condyle and medial patella (Fig. 2). The medial retinaculum appeared to be intact but showed evidence of a low-grade strain (Fig. 2, arrow). An intra-articular body was seen in the medial recess of the joint and was presumed to originate from the patellar defect (Fig. 3). In view of the imaging findings, a surgical procedure was needed to excise the intra-articular body and plicate the medial retinaculum.


Acute patellofemoral dislocation usually occurs in young people during sporting activities. The commonest mechanism is thought to be medial pivoting of the knee on a planted foot, resulting in lateral patellar dislocation with impingement of the medial patella on the lateral femoral condyle and in a strain of the medial patellar retinaculum. The injury is usually transient, with spontaneous reduction occurring almost immediately, meaning that the patient is often unaware of the dislocation. These features together with the presence of hemarthrosis make clinical assessment difficult; the diagnosis remains clinically occult in over 50% of cases. Therefore, the clinical differential diagnosis is large, and, as in this case, MRI can help to determine the mechanism of injury and any sequelae that may need surgical intervention. As in this patient, urgent intervention is warranted when loose intra-articular fragments are present.
Footnotes
Section Editor: Robert S. Bell, MD
Submissions to Surgical Images, musculoskeletal section, should be sent to Dr. Robert S. Bell, University Musculoskeletal Oncology Unit, Ste. 476, 600 University Ave., Toronto ON M5G 1X5; fax 416 586-8397.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.