


Abstract
As technology advances, the techniques of laparoscopic surgery are being refined and their aplication is expanding to include many disease processes and organs. The new-generation laparoscopic instruments are becoming smaller (less than 5 mm). Expected advantages include improvements in cosmesis and patient satisfaction, and decreased postoperative analgesic requirements. Non-neoplastic cysts of the spleen are rare, and their management has evolved from total open splenectomy to laparoscopic cyst decapsulation. A 22-year-old woman with a symptomatic 10-cm epithelial cyst was treated by splenic decapsulation with needlescopic instruments (3 mm or smaller). Three trocars were used: one 12-mm umbilical and two 3-mm subcostal ports. The cyst was punctured by a Veress needle, and after drainage of straw-coloured fluid, circumferential decapsulation with 5-mm laparoscopic shears through the umbilical port site was done. The patient was discharged within 24 hours, having had a single intramuscular injection of meperidine and an excellent cosmetic result.
The current trend in the management of non-neoplastic splenic lesions is toward splenic preservation,1–4 and with technologic advances, procedures are becoming less invasive.5–7 We describe the technique of needlescopic decapsulation of an epithelial splenic cyst.
Case report
A 22-year-old woman presented with sudden onset of severe left upper quadrant abdominal pain that radiated to her right and left shoulder tips. She was otherwise healthy and denied a history of splenic trauma, tropical travel or mononucleosis.
Physical examination and standard blood work gave normal results. Her weight was 48.0 kg. Computed tomography (CT) of the abdomen revealed a cystic lesion of the spleen, 6 cm in dimension, with some evidence of perisplenic inflammation and fluid. There was no calcium within the cyst capsule, and the cyst contents were homogeneous. Her symptoms were thought to be caused by an acute rupture of a splenic epidermoid cyst.
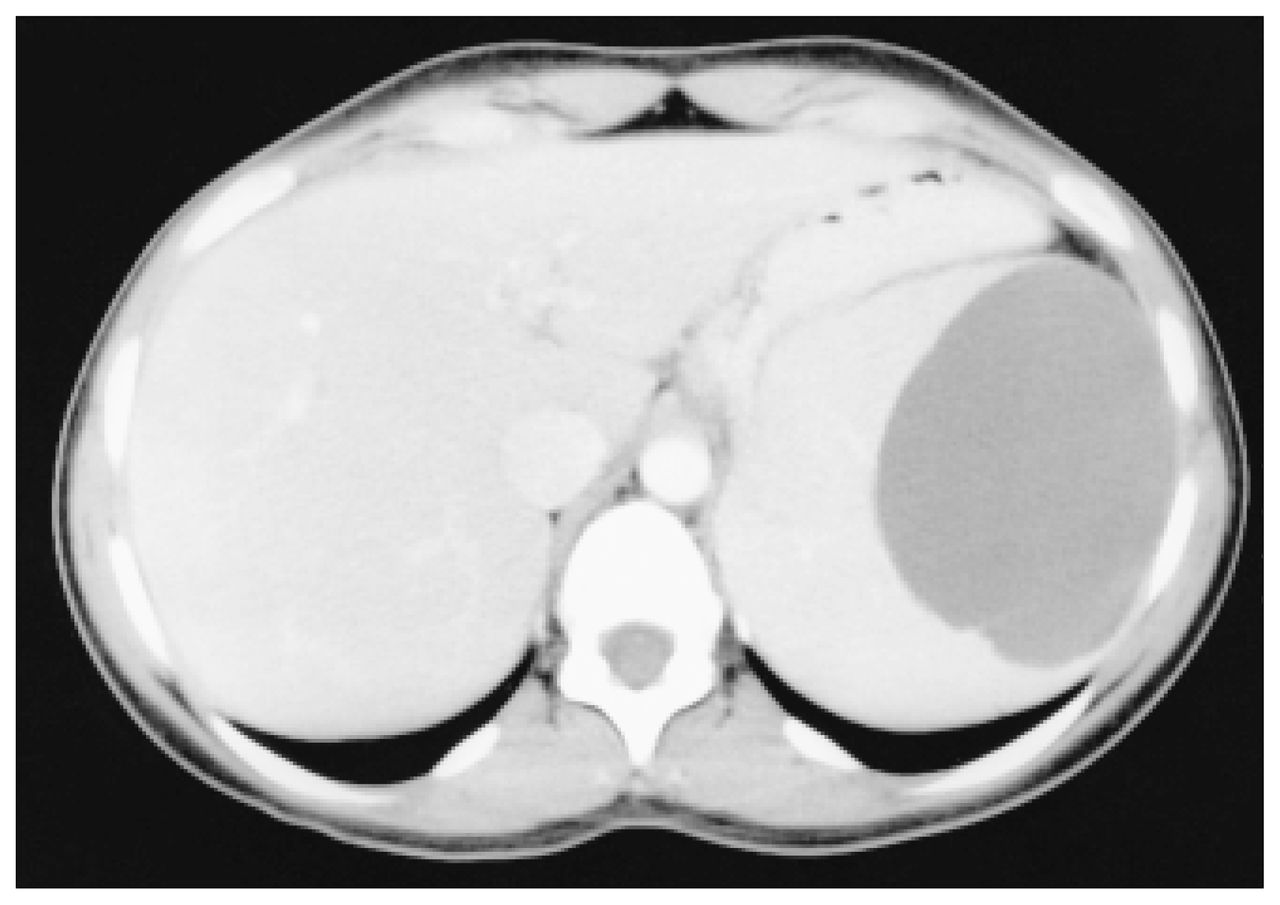
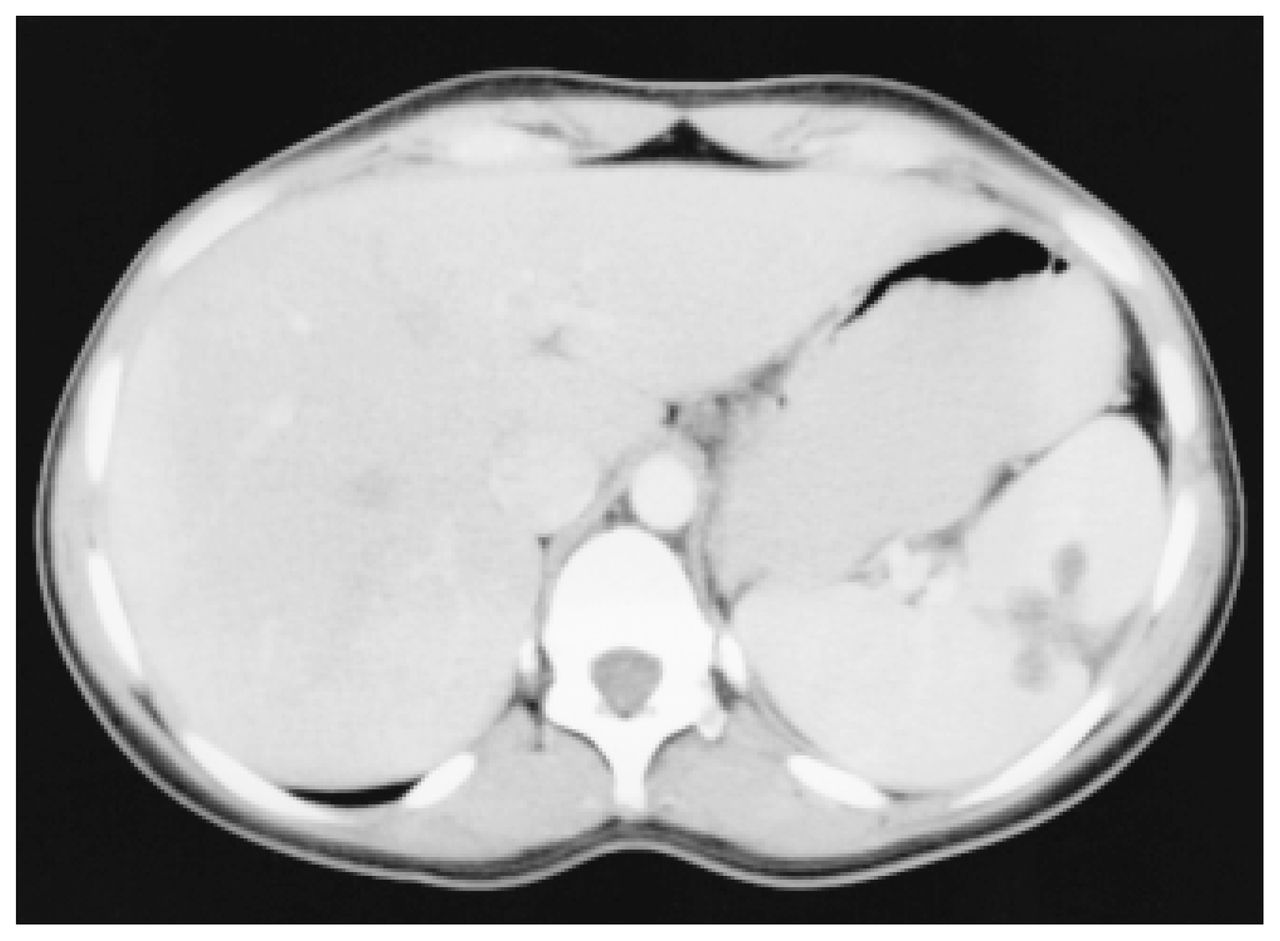
During the following 4 weeks, her pain gradually lessened, but she was left with vague abdominal discomfort in the left upper quadrant. Repeat CT scan (Fig. 1) showed resolution of perisplenic fluid; however, the cyst size had increased to 10 cm, so needlescopic partial cyst decapsulation was planned.
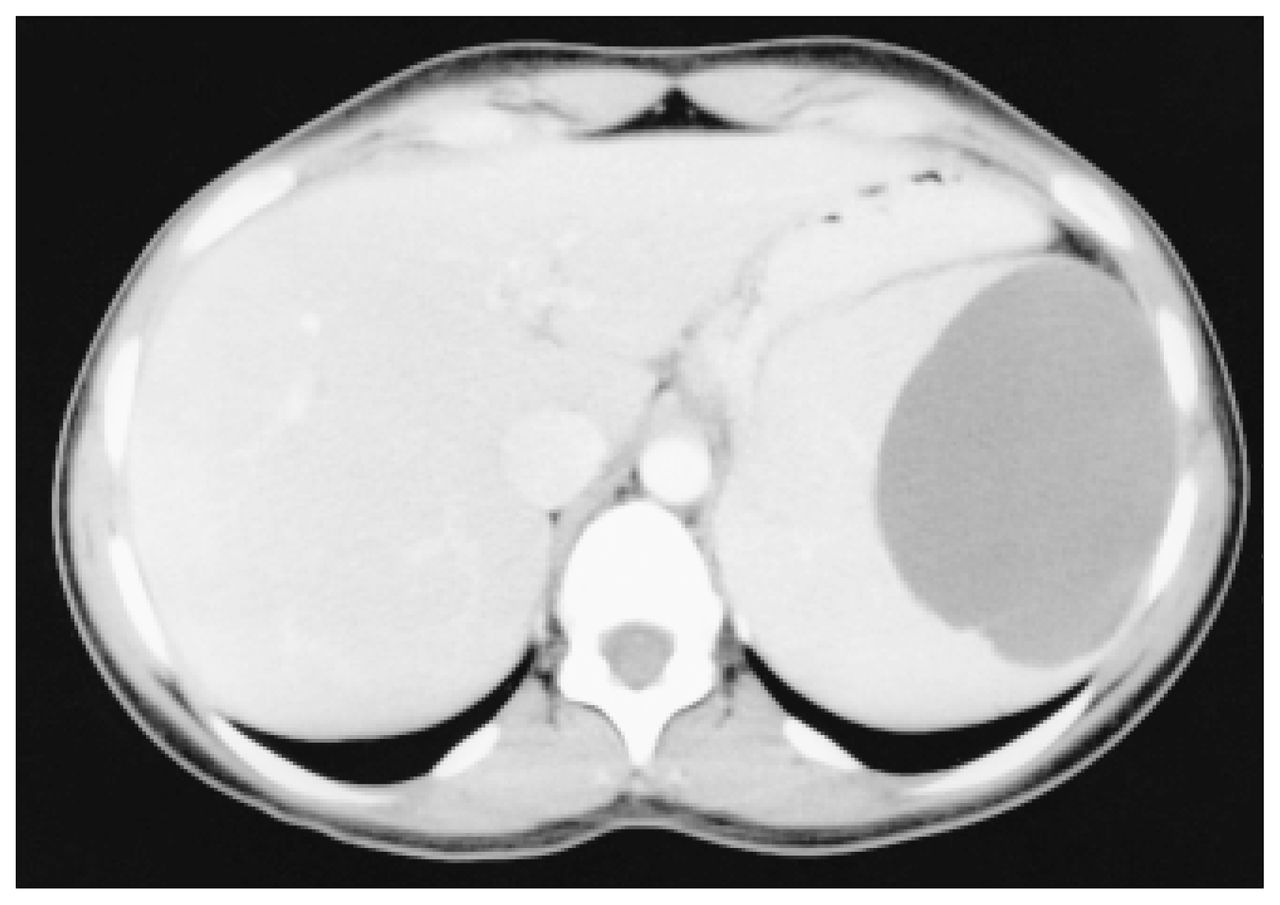
Computed tomography scan demonstrating a large homogeneous splenic cyst, 10 cm in dimension.
Technique
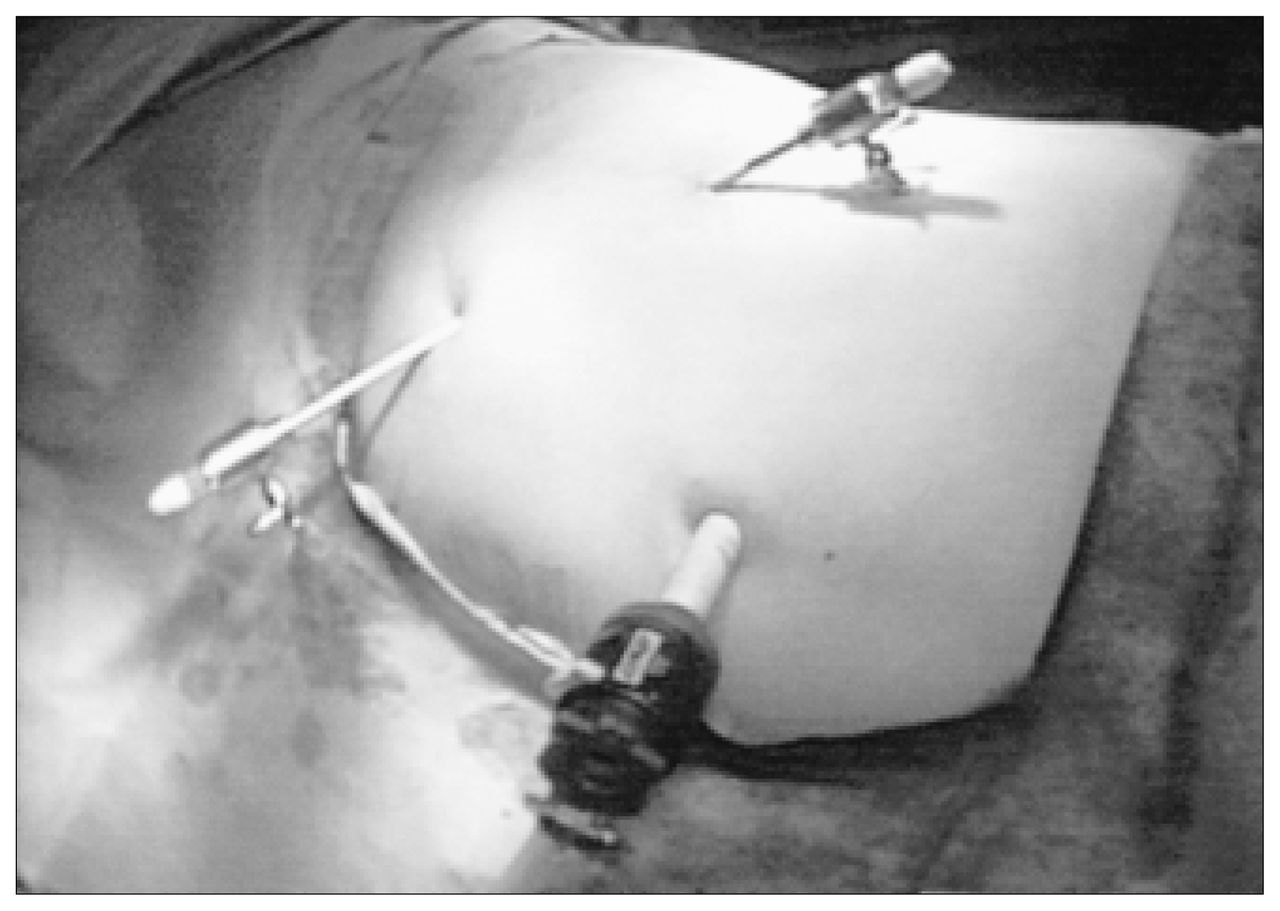
Under general anesthesia, the patient was placed in the right lateral decubitus position, with the table flexed; both the surgeon and assistant faced the front of the patient. Three trocars were used. A direct open technique was used to place a 12-mm laparoscope cannula (Diamond-port 12 mm; Snowden Pencer, Tucker, Ga.) through the base of the umbilicus. A 15 mm Hg carbon dioxide pneumoperitoneum was created, and two 3- mm trocars were installed under direct vision, one in the midclavicular line and the other in the anterior axillary line (Fig. 2).

Positioning of the laparoscopic ports.
The cyst was easily identifiable with the use of a 30°, 10-mm laparoscope and was punctured with a Veress needle and drained of straw-coloured fluid. The 10-mm umbilical laparoscope was advanced into the cyst, which showed a characteristic epithelial lining. This scope was replaced with a 3-mm needlescope, positioned through the anterior axillary port, to facilitate circumferential decapsulation by 5-mm laparoscopic shears through the umbilical port site. The cyst was completely deroofed and hemostasis was achieved with electrocautery. The total operating time was 60 minutes. Pathological confirmation of a benign epithelial cyst was obtained, and the patient was discharged within 24 hours, having had only 1 intramuscular injection of meperidine hydrochloride, 50 mg/mL. She returned to routine activity 7 days postoperatively.
A CT scan done 3 months later showed no recurrence of the cyst and evidence of a remodelling spleen (Fig. 3). Abdominal examination revealed minimally visible scars.
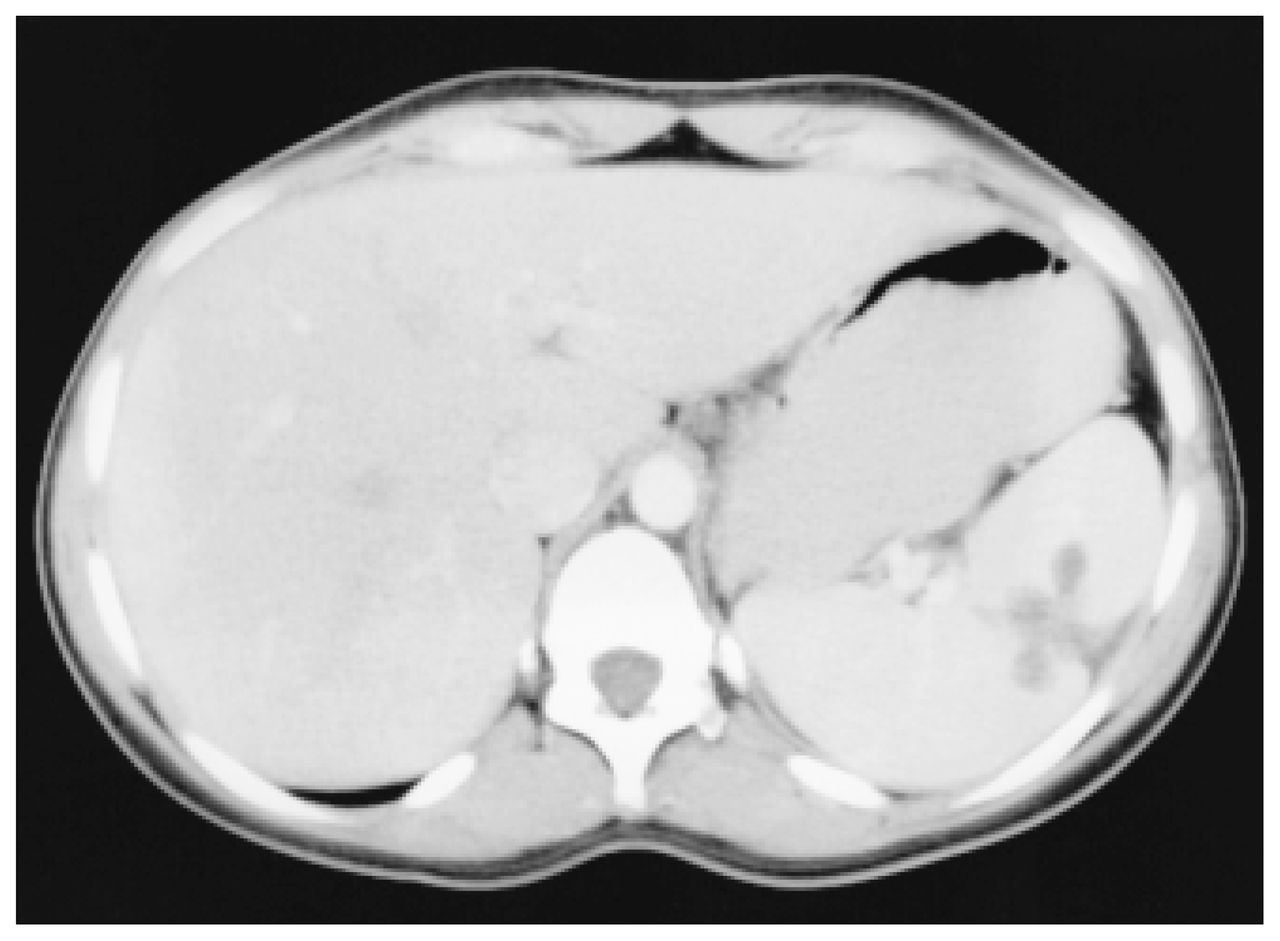
CT scan 3 months after needlescopic partial cyst decapsulation showing splenic remodelling with partial collapse of the previous cyst cavity.
Discussion
True cysts of the spleen, which are rare, have an epithelial lining.3 They can be categorized as either parasitic or nonparasitic.2 Parasitic cysts are more common worldwide but are rare in North America. Epithelial cysts constitute 25% of nonparasitic cysts and are described as epidermoid, dermoid or simple. Pseudocysts, which are false in nature, do not contain an epithelial lining. They make up approximately 75% of splenic cysts3 and usually are related to previous trauma. Congenital epidermoid cysts may be complicated by rupture, intracystic hemorrhage, infection or malignant transformation. Surgical intervention is recommended for relief of symptoms, including pain,4 and to prevent and treat complications.
Therapy for splenic cysts is evolving. Initially, total splenectomy was recommended; however, it was supplanted by a variety of preservation procedures1–4 done to minimize the risk of postsplenectomy sepsis. Splenic decapsulation has been shown to be effective, with low morbidity and recurrence rates.5–7 Technologic advances have simplified treatment by allowing cyst decapsulation to be done laparoscopically.5–7 A new generation of laparoscopic instruments having a diameter of 3 mm or smaller are defined as “needlescopic” and have been used for several abdominal procedures.8 Advantages include early patient discharge, improved cosmesis and shorter operative times because needlescopic ports do not require fascial or skin closure. With only two 3- mm trocars, other than at the umbilical site, postoperative pain seems to be reduced; however, this finding requires further scientific validation. Disadvantages include limited availability of instruments, and a decreased visual field when using a 3-mm needlescope. Consequently, we recommend a single 10- to 12-mm trocar within the umbilicus, so that initially a large laparoscope can be used to assess the peritoneal cavity properly. Use of the umbilicus for a larger cannula maintains cosmesis but also allows flexibility should the 10-mm clip appliers or linear stapler become necessary.
Conclusions
Needlescopic partial splenic cyst decapsulation is a safe, effective alternative to other methods and allows superior cosmesis. It may also produce better outcomes with regard to level of postoperative pain, length of hospital stay and return to activities of daily living.
- Accepted July 18, 1999.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.