


A 64-year-old man had been treated for carcinoma of the anal canal with a combination of chemotherapy, radiotherapy and surgery. Three years later he presented with a 5-month history of severe left hip pain and a 2-month history of severe right hip pain. He required the assistance of a cane for walking. Clinical concerns included fracture and metastatic disease.
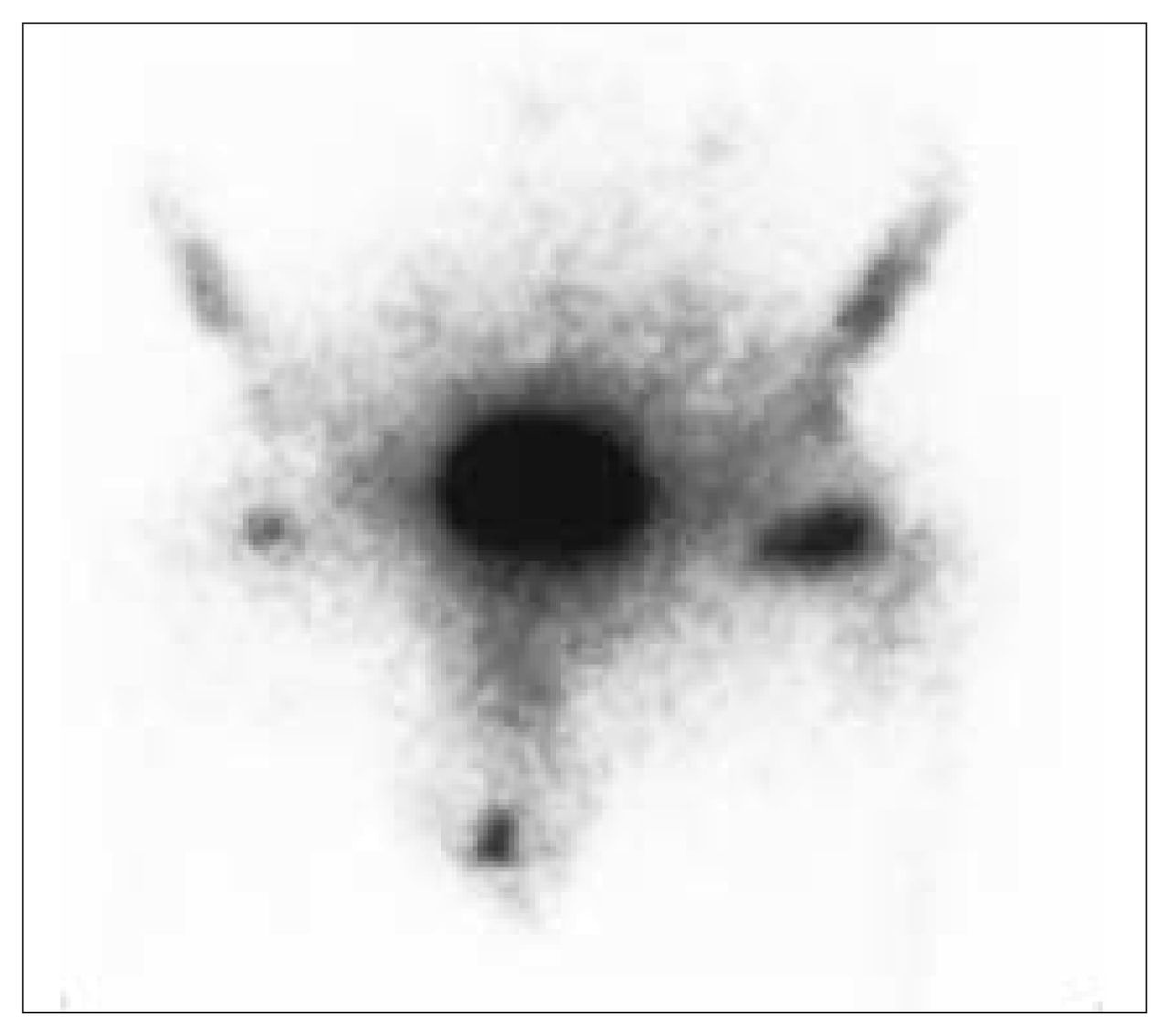
A plain film of the pelvis showed diffuse osteopenia. A technetium-99m scan showed increased uptake in both femoral necks, more so on the left side (Fig. 1). Computed tomography showed linear areas of sclerosis traversing both femoral necks, more marked on the left (Fig. 2).

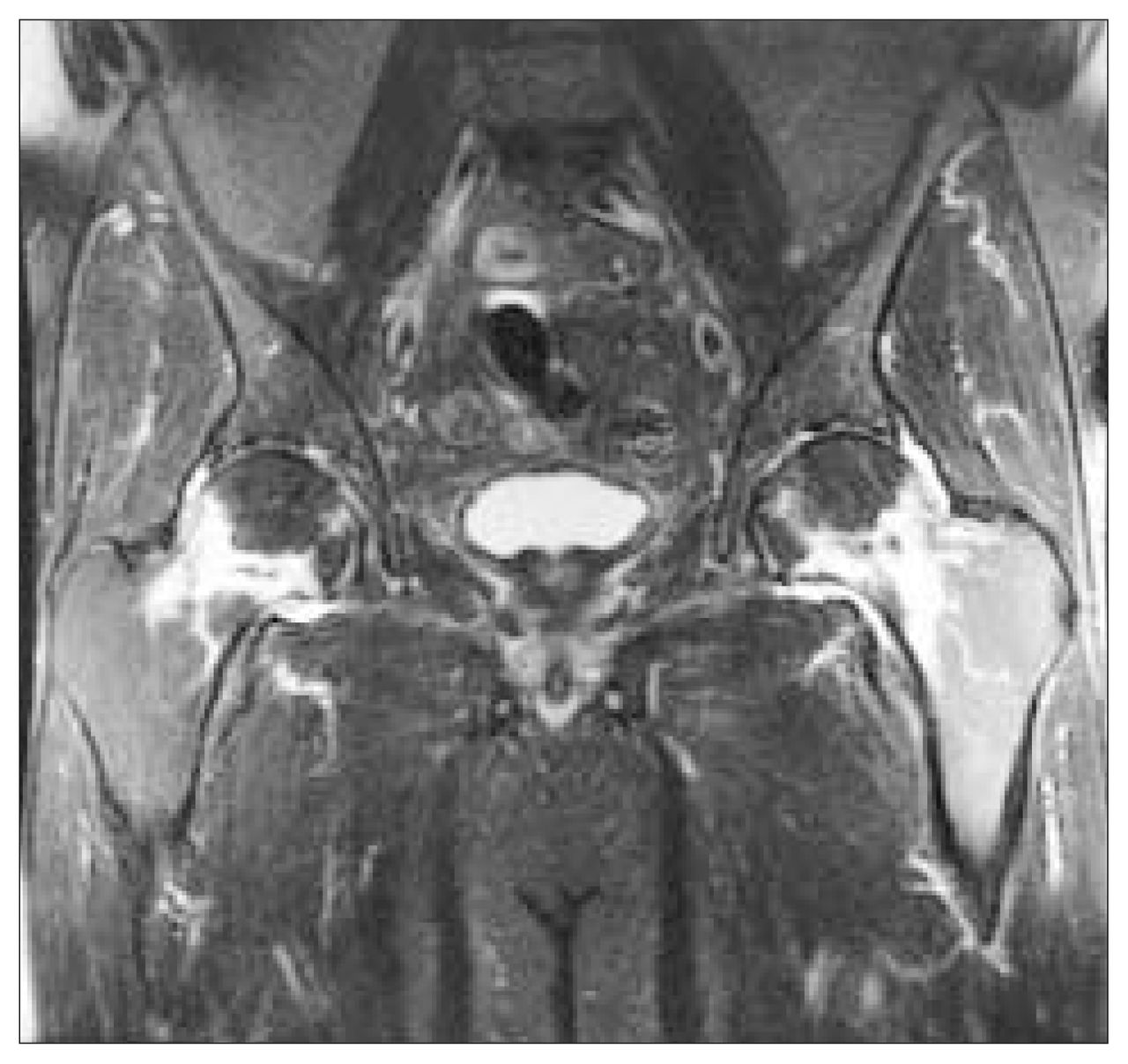
Coronal T1-weighted magnetic resonance imaging (MRI) (Fig. 3) showed low-signal intensity in both femoral necks and diffuse fatty bone marrow throughout the pelvic bones, likely due to pelvic irradiation. Coronal T2-weighted MRI (Fig. 4) showed an irregular low-signal intensity linear band traversing the femoral necks, with a large area of surrounding bony edema and small bilateral hip effusions. Findings indicated near-complete nondisplaced transverse insufficiency fractures across both femoral necks.

Stress fractures of the hip most frequently involve the medial aspect of the femoral neck. They are termed fatigue fractures in patients who have normal bone but are exposed to excessive mechanical stress, such as may be seen in athletes and army recruits, and they are termed insufficiency fractures in patients who have abnormal bone that is subjected to normal stress. Insufficiency fractures most commonly occur in osteoporotic bone but can be seen after pelvic irradiation, steroid therapy and in cases of rheumatoid arthritis and renal osteodystrophy. Typical sites of pelvic insufficiency fractures include the symphysis pubis and pubic rami, sacrum, supra-acetabular ilium and femoral neck. Patients usually present with pain aggravated by weight-bearing.
Early stress fractures may be occult on a plain film. Bone scanning is a very sensitive test for the early diagnosis of a stress fracture; however, it is nonspecific and may be positive in osteonecrosis and in neoplasms. Stress injuries are commonly detected on MRI of the pelvis, most commonly involving the sacrum and pubic rami. MRI is both sensitive and specific in the diagnosis of fractures, which, as in this case, show linear regions of low-signal intensity on both T1-weighted and T2-weighted imaging. T2-weighted images also show a variable amount of high-signal intensity bone marrow edema surrounding the fracture site.
Footnotes
Section editor: Robert S. Bell
Submissions to Surgical Images, musculoskeletal section, should be sent to Dr. Robert S. Bell, University Musculoskeletal Oncology Unit, Ste. 476, 600 University Ave., Toronto ON M5G 1X5; fax 416 586-8397.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.