


Re-expansion pulmonary edema (RPE) is a well-defined complication of lung re-expansion in the management of a pneumothorax or large pleural effusion. Repair of a large and longstanding traumatic diaphragmatic hernia may present a very similar physiologic situation. If the hernia is small or is promptly repaired, reduction of abdominal contents should result in lung re-expansion thus improving cardiorespiratory function. We report the case of a large, missed traumatic diaphragmatic hernia that when repaired resulted in rapid re-expansion of the lung and RPE. This required individual lung ventilation in the intensive care unit. RPE is a direct consequence of increased capillary permeability, the common endpoint of multiple physiological stressors. RPE ranges in extent from being clinically undetectable to causing respiratory failure. Severity is related to the extent and duration of the lung compression. This case serves to illustrate the phenomenon of RPE, which may occur in select cases of diaphragmatic hernia.
Case report
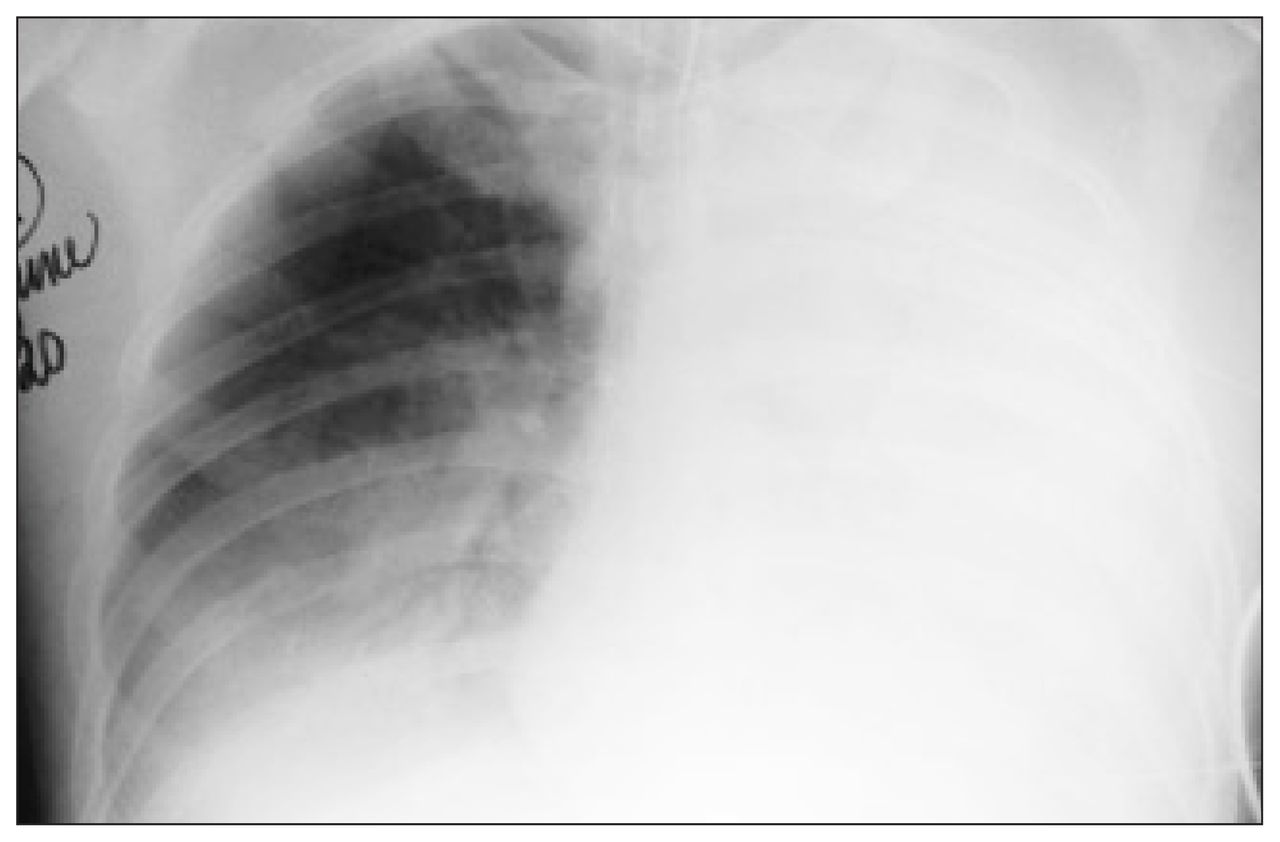
A 27-year-old congenitally deaf and mute man who was otherwise healthy with no surgical history was the belted passenger in a single car rollover. No airbag was deployed, and he was found alert, oriented and walking at the accident scene (Glasgow Coma Scale score of 15). He was brought to a local hospital for assessment. Initial investigations included chest radiography, which was read as normal (Fig. 1). In retrospect, the initial chest film shows significant elevation of the left hemidiaphragm with atelectasis of the left base and fractures of the left fifth, sixth and seventh ribs posterolaterally. Injuries diagnosed at the initial presentation were summarized as follows: fractured left ribs and contusion of the left elbow. He was discharged home the same day.

Posteroanterior radiograph obtained directly after the accident. There is notable elevation of the left hemidiaphragm with atelectasis and fractured ribs.
He continued to suffer from chest pain over area of the rib fractures and from shortness of breath, which was increased by activity and by lifting heavy objects. Five days after the collision, the shortness of breath became markedly worse, especially with eating, lasting several hours postprandially. This was associated with new-onset vomiting, postprandially, of gastric contents. The morning of admission, 6 days after the accident, he took a 3-hour flight in a pressurized aircraft. During the flight he felt very short of breath and upon arrival at his destination he went to his general practitioner who referred him immediately to the London Health Sciences Centre.
During the initial resuscitation he was found to have an oxygen saturation of 60% on room air, respiratory rate 27 respirations/min, a heart rate of 130 beats/min, a blood pressure of 170/112 mm Hg and a body temperature of 37.9 °C. The administration of 100% oxygen by mask resulted in an oxygen saturation of 95% to 99%. On examination there was good air entry on the right side. On the left there was minimal air entry with audible bowel sounds from base to apex. The trachea was midline. Centrally placed heart sounds were audible. There was tenderness over the posterolateral chest area with no open wounds or subcutaneous air. The abdomen was slightly distended but otherwise soft and non-tender. Blood gases on 100% oxygen showed a pH 7.39, partial pressure of oxygen 237 mm Hg and partial pressure of carbon dioxide 29 mm Hg, bicarbonate 18 mmol/L and oxygen saturation 99%. An electrocardiogram showed sinus tachycardia. Another chest radiograph obtained showed the left hemithorax filled with distended loops of small bowel and a mediastinal shift (Fig. 2).

Portable chest radiograph obtained 6 days after the accident. Bowel loops can be seen in the left hemithorax and a shift of the mediastinum to the right.
The patient was brought emergently to the operating room and a midline laparotomy was performed. A tear of the diaphragm just anterior to the left crus was seen. Viable stomach, small and large bowel and omentum had herniated into the chest. No other injuries were apparent. On reducing the abdominal contents the left lung was felt to re-expand. Immediately, the patient’s oxygen saturation dropped to 30% to 40% with an associated increase in heart rate to above 140 beats/min and a drop in systolic blood pressure to 70 to 80 mm Hg. Copious amounts of pink froth were noted in the endotracheal tube. Suction was applied and oxygen administered to a saturation of 80% to 90%. The exploratory laparotomy was completed, the diaphragm repaired, a chest tube inserted on the left side and the patient returned to the intensive care unit. The postoperative chest radiograph (Fig. 3) showed RPE. Because of difficulty in achieving adequate ventilation, a double-lumen endotracheal tube was inserted and the lungs were independently ventilated. During a 3-week stay in the intensive care unit complicated by pneumonia, the patient was gradually weaned onto room air and was discharged home 4 weeks postoperatively. At 9 months’ follow-up the patient was well with no residual respiratory deficits.

Portable chest radiograph obtained immediately after operation shows reexpansion pulmonary edema.
Discussion
Reviews of diaphragmatic herniation resulting from blunt trauma have documented a missed diagnosis rate of 12% to 33%.1–4 These authors recommended acute awareness of the condition in patients with blunt thoracoabdominal trauma, especially those with multiple injuries. In patients who undergo laparotomy or thoracotomy, inspection of the diaphragm is mandatory. In those patients who do not undergo operative intervention, initial chest radiography is the most sensitive diagnostic modality for finding disruption and should be screened for pathognomonic signs of gas bubbles, nasogastric tube content or oral contrast material in the chest and more subtle signs such as irregularity of the diaphragmatic outline, elevated hemidiaphragm, mediastinal shift without pulmonary or intrapleural cause and compression atelectasis of the lower lobe.3 In patients without a clear indication for laparotomy and a normal or equivocal chest radiograph with clinical suspicion, repeat chest radiography with a nasogastric tube in place or an upper gastrointestinal contrast study is recommended. Whereas the most patients at risk for this injury have had abdominal computed tomography, a normal scan does not rule out diaphragmatic injury as CT has an inconsistent success rate, ranging from 0 to 100%.1 Although of limited value in the initial evaluation of the trauma patient, further study into the role of ultrasonography, magnetic resonance imaging and radionuclide scanning may prove that these investigations are useful adjuncts. In our case the initial chest radiograph in retrospect was suggestive of an injury, and the repeat radiograph obtained for new-onset symptoms of respiratory distress was diagnostic.
Unilateral RPE is a rare but well-defined complication of treatment for pneumothorax and pulmonary effusion. It is a rapid process, developing within 1 hour of re-expansion in two-thirds of cases and within 24 hours in the remainder. 5 Most cases occur within the ipsilateral collapsed lung, although ROPE has been seen bilaterally in up to 6.7%.6,7 Clinical severity ranges from asymptomatic radiologic abnormalities to severe cardiopulmonary insufficiency and death, with one clinical study reporting a death rate of 20%.5 Increased mortality is associated with bilaterality and sudden onset.5,7 The clinical presentation consists of tachypnea, tachycardia, hypotension, cyanosis, pink frothy sputum production, cough, dyspnea and chest pain with decreased air entry and audible rales over the affected lung.5,8
Our current understanding of the pathophysiology of RPE is that it is likely a multifactorial process with the edema resulting from increased capillary permeability due to hypoxic and mechanical damage to the alveolar capillary membrane during lung compression. This is exacerbated by increased blood flow to the pulmonary vasculature after reexpansion and a relative negative perivascular pressure further drawing fluid into the lung tissue. It has been shown that there is decreased blood flow to the compressed lung,9 and this is thought to cause hypoxic damage to the endothelium of the capillary walls, leading to increased vascular permeability. Analysis of the edema fluid has shown a high ratio of protein to serum, as would be expected with increased permeability as opposed to hydrostatic edema. This is also supported by a study showing that in lungs with both aerated and compressed segments, it is preferentially the compressed segment that manifests pulmonary edema.6 In addition to this, current research into ischemia and reperfusion injury of the lung demonstrates that in RPE a local inflammatory reaction occurs. Local imbalances in nitric oxide levels and an influx of neutrophils and their degranulation products potentiate the capillary damage.10,11 This common endpoint of increased endothelial permeability is also thought to be exacerbated by increased pulmonary flow occurring after re-expansion.7 In addition to this the decrease in perivascular interstitial lung tissue pressure that occurs with re-expansion will result in increased extravasation of fluid, which may also be an important factor contributing to pulmonary edema.5,7
Clinically evident RPE associated with diaphragmatic hernia has not been reported in the English literature. The literature on RPE pathophysiology in the setting of pneumothorax and pleural effusion shows that for RPE to occur, the lung compression must be sufficiently large and long-standing. Unlike the hernia in our case, most large traumatic diaphragmatic hernias will be recognized and repaired before any damage to the compressed lung, so RPE will not be seen. Not only must sufficient lung mass be compressed, but studies have shown that as the duration of lung collapse increases, the rate of RPE also increases.5,6,12 In one series 83% of the cases of RPE occurred only after more than 3 days of collapse (average 9 days, range from 0 to 81 days).5,6 This has been confirmed in animal studies.12
In preventing RPE, it has been advocated but not proved that the rate of reexpansion is important in decreasing the extent of the pulmonary edema,5,8,13 but this is difficult to control intraoperatively. In patients who undergo repair for large missed diaphragmatic hernias, the use of a double-lumen endotracheal tube from the outset and, if the patient is not extubated postoperatively, up to 24 hours after re-expansion when it is most likely to occur, may protect the contralateral lung and major airways. Also this can increase the efficiency of ventilation to the contralateral lung and allow suctioning of the affected lung should pulmonary edema occur intraoperatively. In addition, research into the role of local inflammatory mediators in RPE has led to the untested suggestion that the prostaglandin analog misoprostol and anti-inflammatory drugs such as ibuprofen or indomethacin may be useful in shortening its course.7 Finally, at one time, it was postulated that the negative intrathoracic pressures associated with pleural drainage systems contributed to RPE. There is evidence however, that RPE can occur with very low levels of negative pressure, straight underwater seals and needle aspiration. Thus, the use of a chest tube postoperatively to drain the accumulations in the pleural space likely will not contribute to RPE.5,6,13 RPE is a rare complication seen in the sudden re-expansion of a compressed lung. This can occur intraoperatively and therefore needs to be considered in the management of large, missed traumatic diaphragmatic hernias.
- Accepted March 2, 2000.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.