


Abstract
Objectives: To assess the risk of postoperative infection associated with blood transfusion in patients who undergo primary total hip arthroplasty.
Design: A retrospective cohort study.
Setting: Victoria General Hospital, Halifax, (a tertiary-care centre).
Patients: All patients who underwent primary total hip replacement between 1990 and 1995 (N = 1206).
Interventions: Hip replacement with or without perioperative blood transfusion.
Outcome measures: The rate of postoperative infection, the number of blood transfusions, patient age and sex, duration of surgery and the surgeon who performed the procedure. Victoria General Hospital medical records, the transfusion services record and the Dalhousie University Hip Study databases were integrated and analyzed using a standard statistical package.
Results: The incidence of infection postoperative was 9.9% overall, 8.4% in patients receiving no transfusion, and 14% in those receiving homologous transfusion (p = 0.035). There were no infections in the 11 patients who received an autologous blood transfusion. Significant predictors of postoperative infection were sex, age and duration of surgery; these were not confounding variables (χ2 multivariate analysis). Neither the operating surgeon nor the blood product transfused affected the infection rate.
Conclusions: These findings suggest an increased risk of postoperative infection in patients who undergo primary hip replacement and receive homologous blood transfusions perioperatively.
Since the 1973 report of Opelz and colleagues,1 it has been generally accepted that homologous blood transfusions exert some immunosuppressive effect. However, evidence for these effects has been controversial. It has been suggested that the immunosuppressive effect of blood transfusions can have different and serious implications, depending on the clinical scenario. These include transplant graft survival,1–3 tumour growth and recurrence2–10 and postoperative infection rates.2,3,11–15
Before the introduction of cyclosporine, it was shown that transfusion did indeed induce some immunosuppressive effect. When treated as an independent variable, transfusion-induced immunosuppression could increase a 1-year graft survival rate by as much as 20%.1,2
Results from studies on tumour growth, and recurrence and metastasis have been variable. The data are unclear — some studies have suggested an increased rate of tumour recurrence related to homologous blood transfusion whereas others have failed to show any effect on tumour growth or recurrence.2–10
Blood transfusion was shown to have a significant effect on postoperative infection rates in 3 studies done by Tartter and colleagues.11–13 In 1986, this group investigated 168 patients who had surgery for colorectal cancer.13 They found that the infection rate was significantly (p = 0.01) increased when the patients received a blood transfusion. The study was repeated by the same group of researchers in 1988 with a study population of 343 patients.11 These patients also underwent colorectal surgery for cancer and, once again, a highly significant difference was shown. In the same year they carried out a similar study on 169 patients with Crohn’s disease.12 Again, they were able to show that a blood transfusion placed the patients at a higher risk for a postoperative infection (p = 0.0004). Two similar studies were performed, on patients who underwent orthopedic elective extremity surgery, to assess the risk of postoperative infection related to a homologous blood transfusion. In 1992, Fernandez and colleagues15 reviewed 376 patients but were unable to show a significant difference in infection rates among patients who did or did not receive a blood transfusion. In 1991, Murphy and colleagues14 reported on a series of only 84 patients in which they examined the difference between homologous and autologous blood transfusions. The rate of infection was significantly (p = 0.0029) higher for homologous blood transfusion than for autologous blood transfusion. However, their study population was small and the outcome criteria were inconsistently defined.
Methods
This study was designed to examine whether homologous blood transfusion significantly increased the risk of acute and subacute postoperative infections in patients who underwent primary total hip replacement. The study population included all patients who underwent this procedure at the Victoria General Hospital in Halifax, between January 1990 and December 1995. Patients who were excluded were those having rheumatoid arthritis, psoriasis or diabetes, those requiring a revision procedure and those having a preoperative diagnosis of infection. The patient inception cohort was identified using the patient’s hospital identification number, which was used as the unique identifier and then cross-referenced to the blood transfusion services database and the medical records database. The blood transfusion and medical records databases were then scanned for all transfusions given within 14 days and 30 days, respectively, of the hip replacement operation. Additionally, operating surgeon, patient demographics and comorbidity data were collected. The protocol for these patients was early mobilization, Foley catheter use for 24 hours followed by catheterization as required and discharge in the first week if there were no complications. Transfusion threshold was a hemoglobin of 100 g/L for patients with cardiac disease or cerebrovascular disease. For other patients a cutoff of 80 g/L or positional change was used. It was impossible to verify if the treatment of all 1206 patients followed these protocols strictly. In cases of infection, the hospital chart was reviewed. Any patients who were readmitted for infection were automatically captured in the medical records database.
The information contained in the hospital medical records database is routinely encoded for all patients after discharge by medical records employees who have undergone a 2-year course to train them in established standards.
These data were then collated, using Microsoft Access (Microsoft Corp., Seattle) into spreadsheet format. The infections were grouped into the following categories: sepsis, cellulitis, pneumonia, bacterial enteritis, wound infection, infected implant and urinary tract infections. Only transfusions of packed red blood cells were included. The data were analyzed using Epi-info 6.0 statistical software (Centers for Disease Control and Prevention, Atlanta). Categorical variables were compared by the χ2 test, and continuous variables were compared by the Kruskal–Wallis test for 2 groups. When χ2 tables contained cells with less than 5, the Mantel–Haenszel correction was employed. All variables were tested for independence by multivariate analysis.
Results
The number of patients who underwent primary total hip replacement during the study period was 1415. Two hundred and nine patients were excluded, leaving a study population of 1206. Of these, 323 (26.8%) received a blood transfusion (312 homologous and 11 autologous blood).
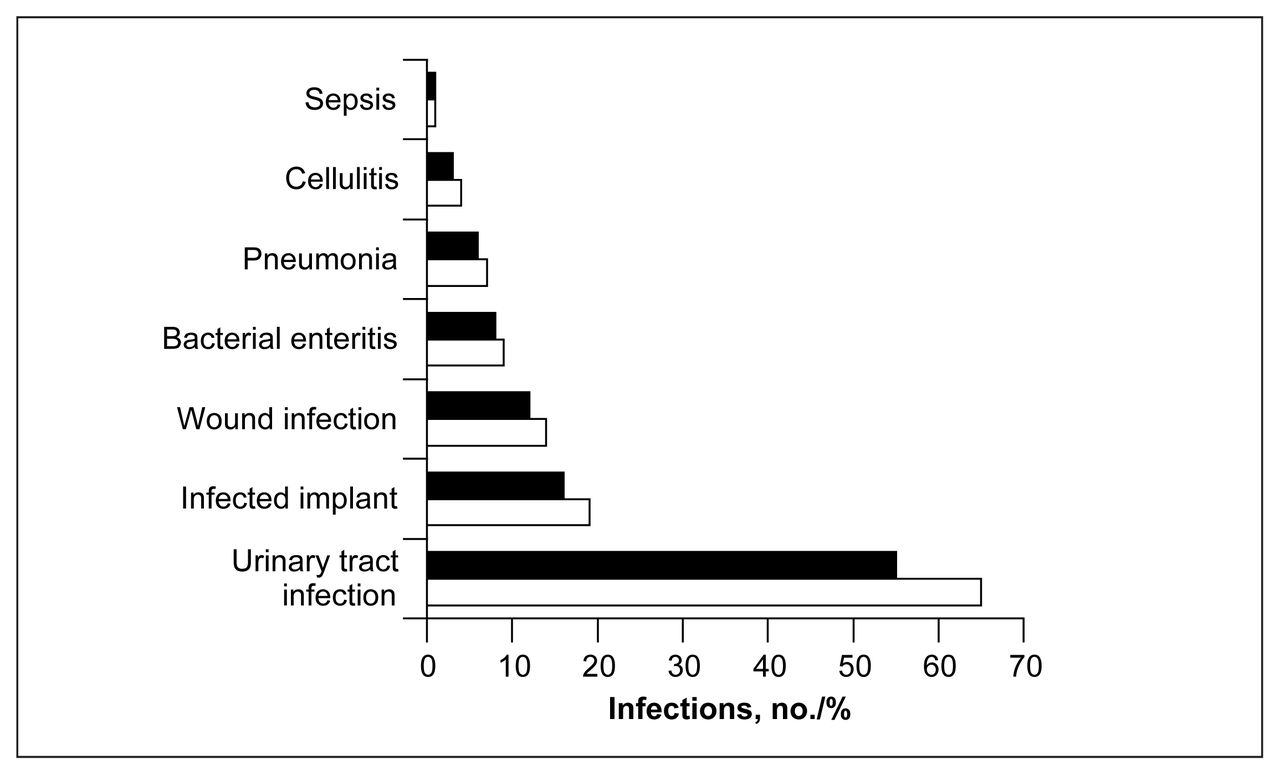
The distribution of postoperative infections is shown in Fig. 1. Urinary tract infections were overwhelmingly the commonest postoperative infection, accounting 65 of the 119 infections. When infection rates of transfused and nontransfused patients were compared, a significant difference in the incidence of infection existed (transfused patients 14%, non-transfused patients 8.4%, p = 0.0353).
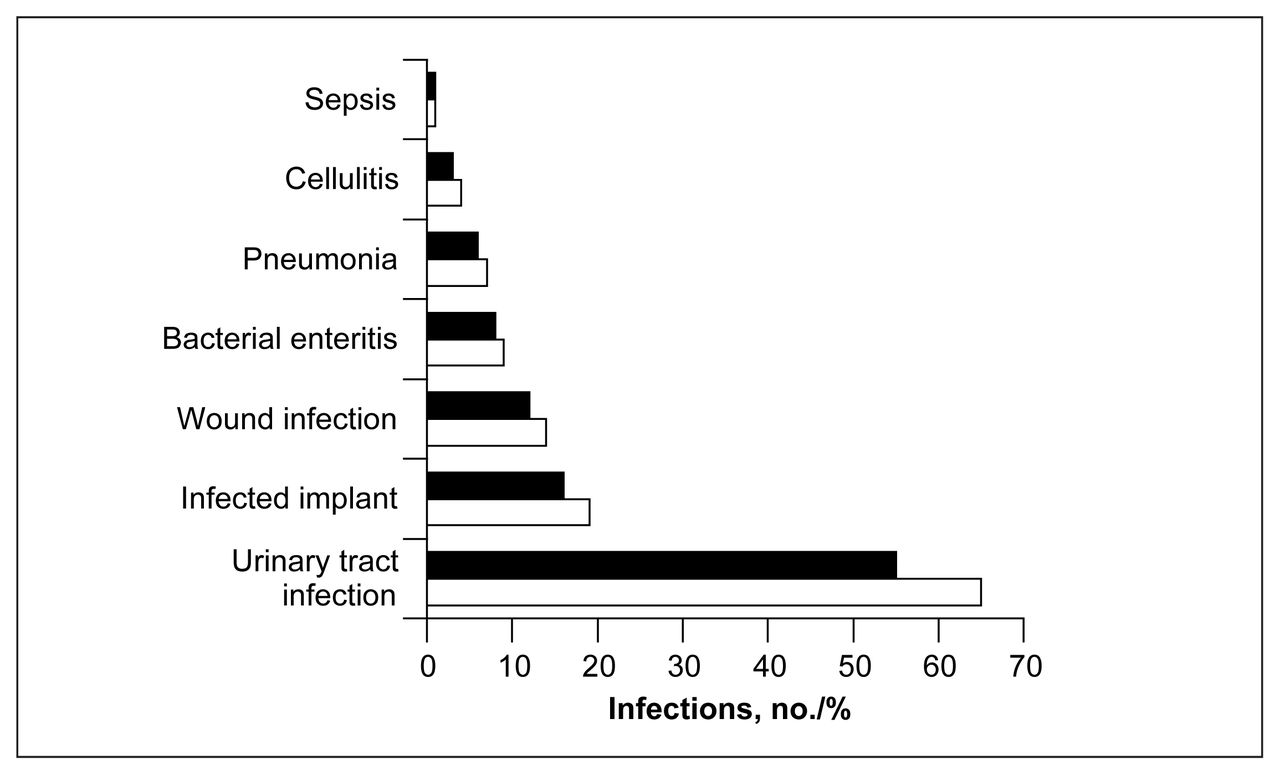
Number (white bars) and percentage of total infections (black bars) for patients who underwent primary hip replacement.
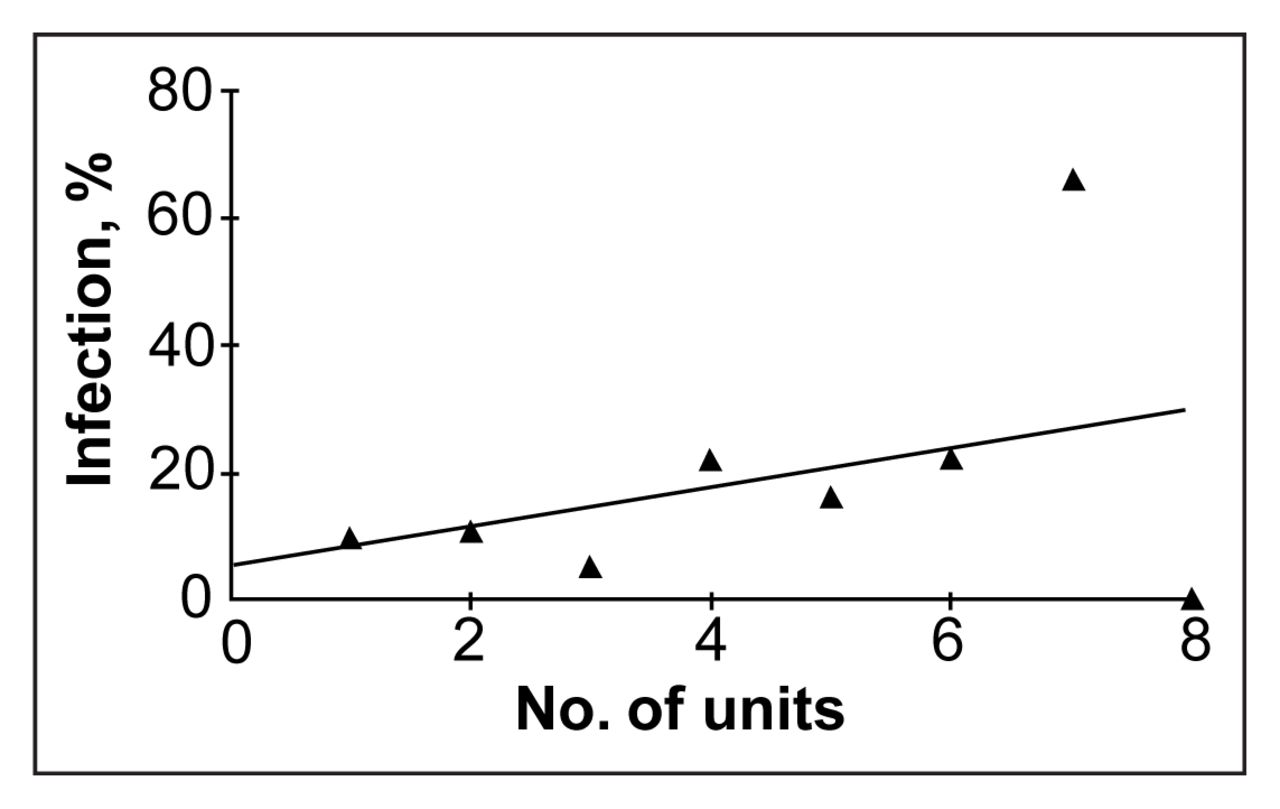
When patients were classified into those who received 2 or more units of blood and those who received 1 unit or no blood, the infection rate was significantly different (p = 0.0223). It was also shown that postoperative infection rates increased significantly with the number of units of blood transfused (p = 0.012) (Fig. 2).
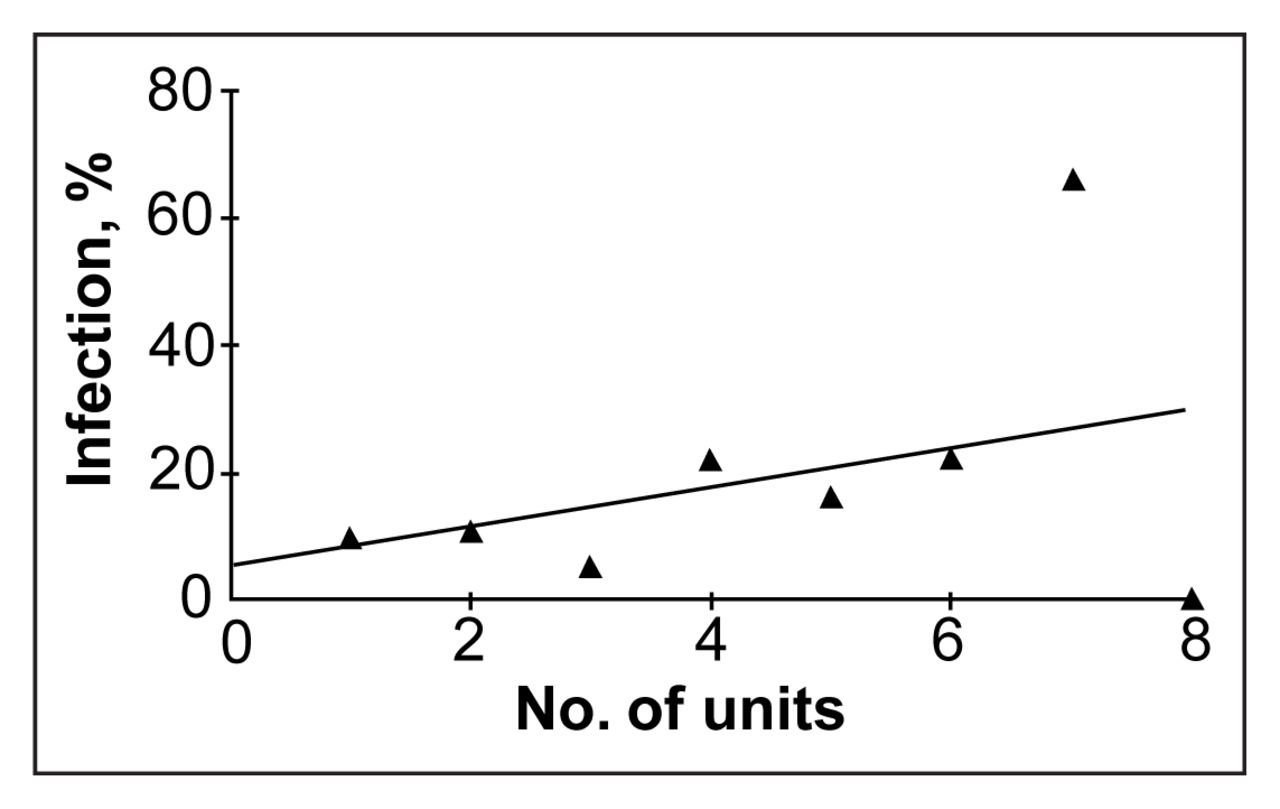
Infection rate versus units of blood transfused.
The mean number of units transfused was 2.7 and the total number of units transfused 323. Among the 11 patients receiving autologous blood, there were no postoperative infections. However, this population was too small for any statistically significant contribution to the data.
The duration of operation, the sex and age of the patient and the operating surgeon were all examined to see if they were associated with elevated rates of postoperative infection. Significant independent predictors of postoperative infection included: sex (p < 0.003) with female patients at increased risk, age (p = 0.014) with older patients at increased risk, and duration of the operation (p < 0.005) with longer operating times increasing the risk. When the transfusion rate was compared for association with the duration of operation, we found that the mean operative time was 125 minutes for transfused patients compared with 116 minutes for nontransfused patients (p < 0.005). The postoperative infection rate did not vary significantly among the 13 operating surgeons (p = 0.619).
We examined whether transfusion and operative time were continuous variables that acted independently to affect the postoperative infection rate. Partial regression analysis showed that transfusion (p < 0.005) and duration of operation (p < 0.025) act independently. Significant predictors of infection including transfusion, patient age, patient sex and duration of surgery were found to be non-confounding variables by χ2 multivariate analysis. We also found that the presence of a postoperative infection significantly (p < 0.005) prolonged patient hospitalization (mean 4.23 d).
Discussion
This study confirms previous suspicion that homologous blood transfusion is indeed a significant and independent risk factor for postoperative infection. Furthermore, this effect has been shown to be dose dependent. When other independent predictors of postoperative infection were examined we found that female, older patients and patients whose operations were longer in duration were at increased risk of postoperative infection. These factors were all shown to act independently. The individual operating surgeon did not significantly influence the risk of postoperative infection.
Numerous theories of how transfusion may induce immunomodulation are presently being considered.16–19 Most of the data concerns the altered function of macrophages. It has been shown that post-blood-transfusion macrophages have decreased migratory ability in response to chemotactic stimuli and that macrophages after transfusion have increased production of prostaglandin E2.16 This increased level of prostaglandin E2 results in decreased activity of antigen presenting cells, decreased production of interleukin 2 and decreased receptor-mediated interleukin 2 response.17 Transfusion has also been linked to decreased numbers of helper T cells, decreased numbers of monocytes, decreased activity of natural killer cells, and increased numbers and function of suppressor cells.17,18
Regardless of the specific mechanism of immunomodulation it has been shown that patients incur increased morbidity and increased length of hospital stay secondary to postoperative infections.16,19 Since we have shown that homologous transfusion is a significant contributor to this outcome, the current trend to minimize the rate of homologous blood transfusions perioperatively is appropriate. The use of autologous blood was not shown to affect the rate of infection. Perhaps with transfusion of autologous blood this immunomodulation may be minimized. Lowered costs as a result of a reduction in hospitalization time and treatment of postoperative infections may counteract the increased costs of routine autologous blood donation.
Conclusions
Homologous blood transfusion is a significant independent risk factor for postoperative infection in patients who undergo primary total hip arthroplasty. In this population patients are 1.55 times more likely to get a postoperative infection if they have received a blood transfusion. Prospective studies comparing autologous versus homologous transfusion infection rates are necessary. An analysis of the increased cost of autologous blood donation should be compared with the potential cost-savings of lower infection rates, translating into decreased postoperative length of hospitalization.
Footnotes
Presented in part at the 52nd Annual Meeting of the Canadian Orthopaedic Association, Hamilton, Ont., May 31 to June 4, 1997.
- Accepted May 7, 2001.
References
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.