


Jefferson fracture (C1 burst fracture)
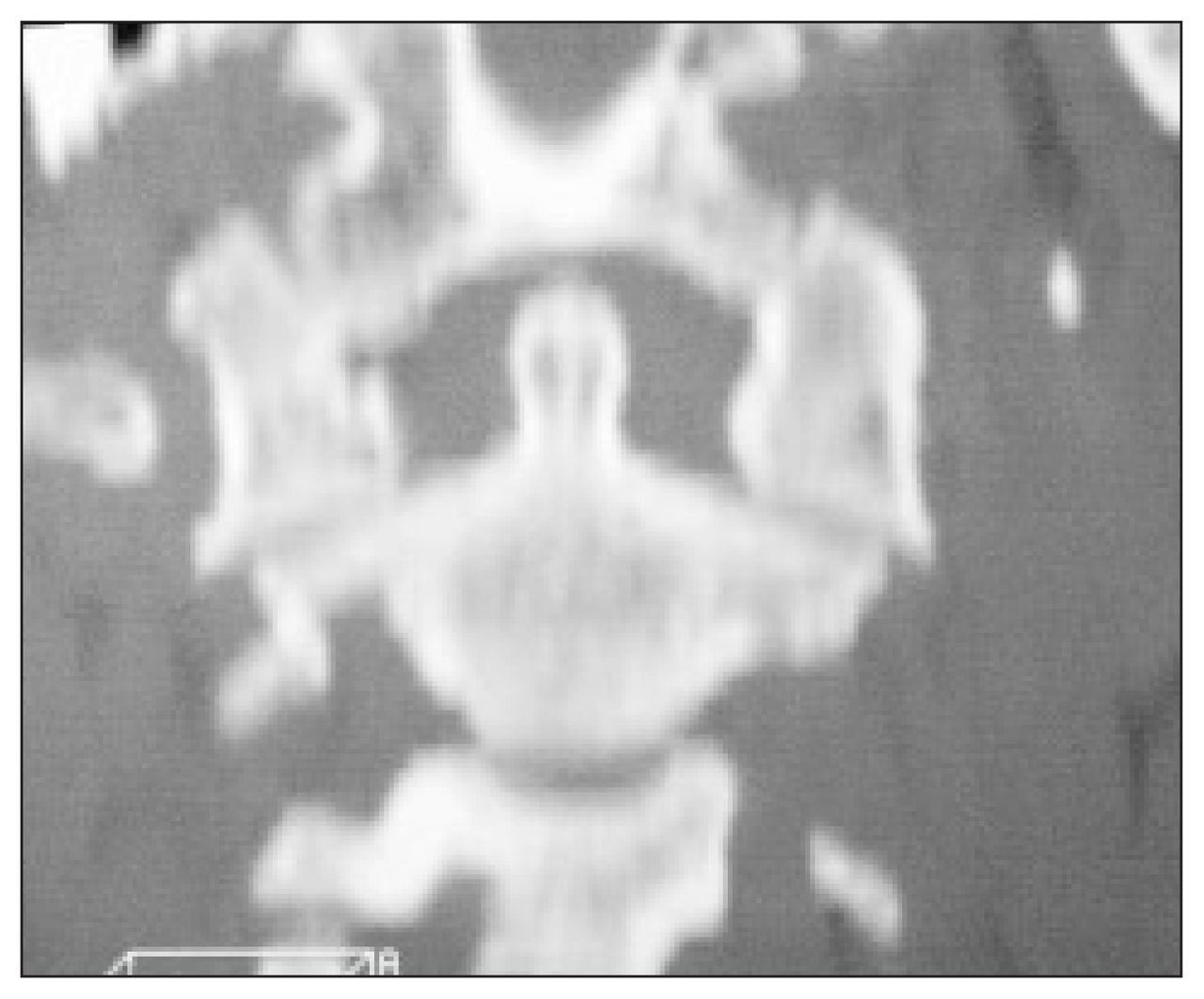
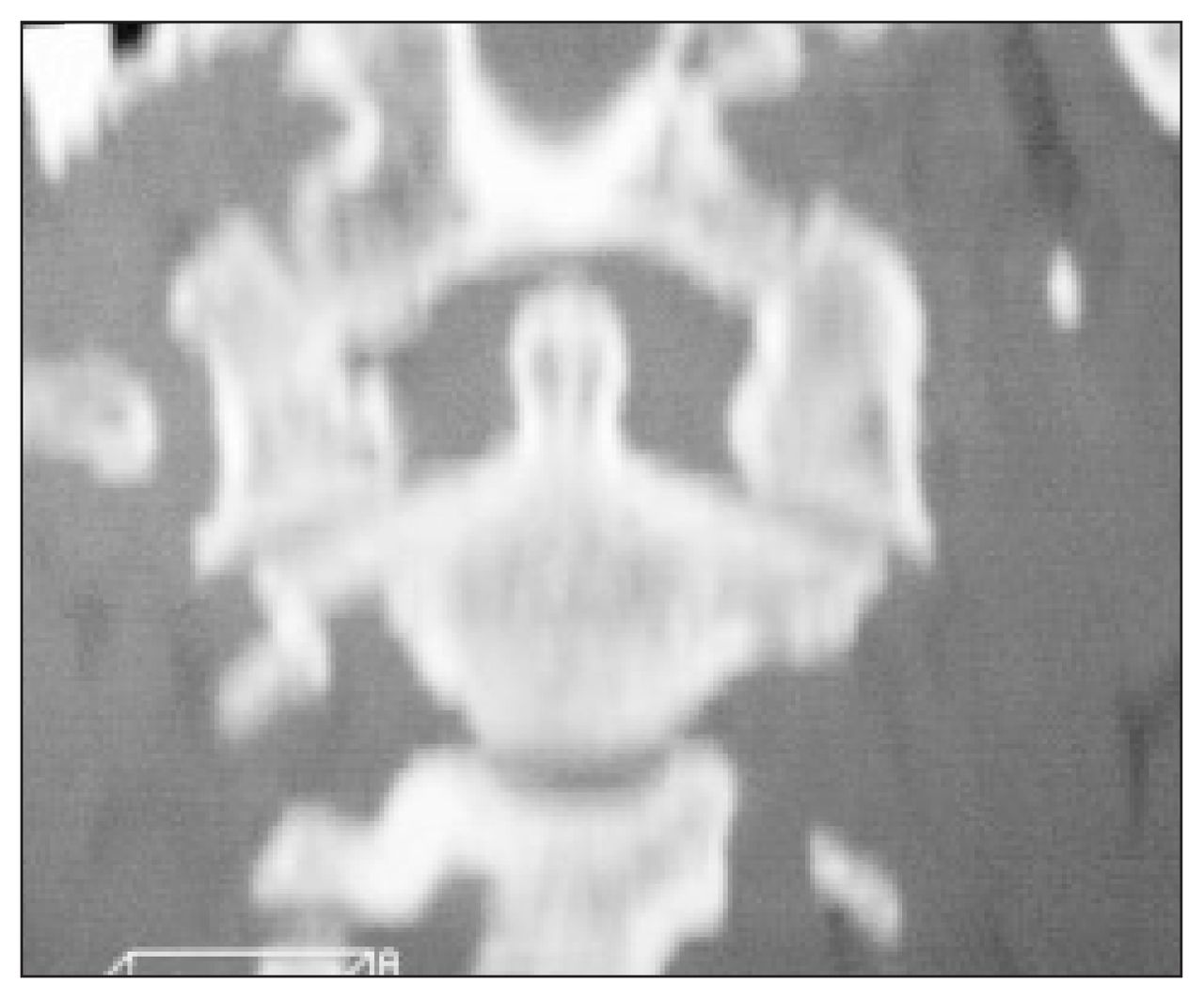
Disruption of the spinolaminar line at the C1 level with anterior movement of the posterior elements of C1 relative to the rest of the spine (arrows) is shown in Fig. 1 (see page 16). In Fig. 2 (see page 16), the open-mouth view, there is asymmetry and widening of the lateral spaces between the dens and the lateral masses of C1. In addition, there is displacement of the lateral masses of C1 relative to the superior articulating facets of C2 (arrows).
A Jefferson fracture is a burst fracture of the atlas. It was named after G. Jefferson who, in 1920, described a classification system for atlantal fractures. This fracture is usually caused by a vertical compression injury. 1 An axial force is transmitted through the occipital condyles to the superior articulations of C1, forcing them apart radially and producing either 3- or 4-part fractures. The fracture usually results from a fall or an automobile collision. Patients seldom have neurologic compromise at the time of presentation because the fractured fragments are propelled away from the spinal canal. Occasionally, this may result in vertebral artery injury.
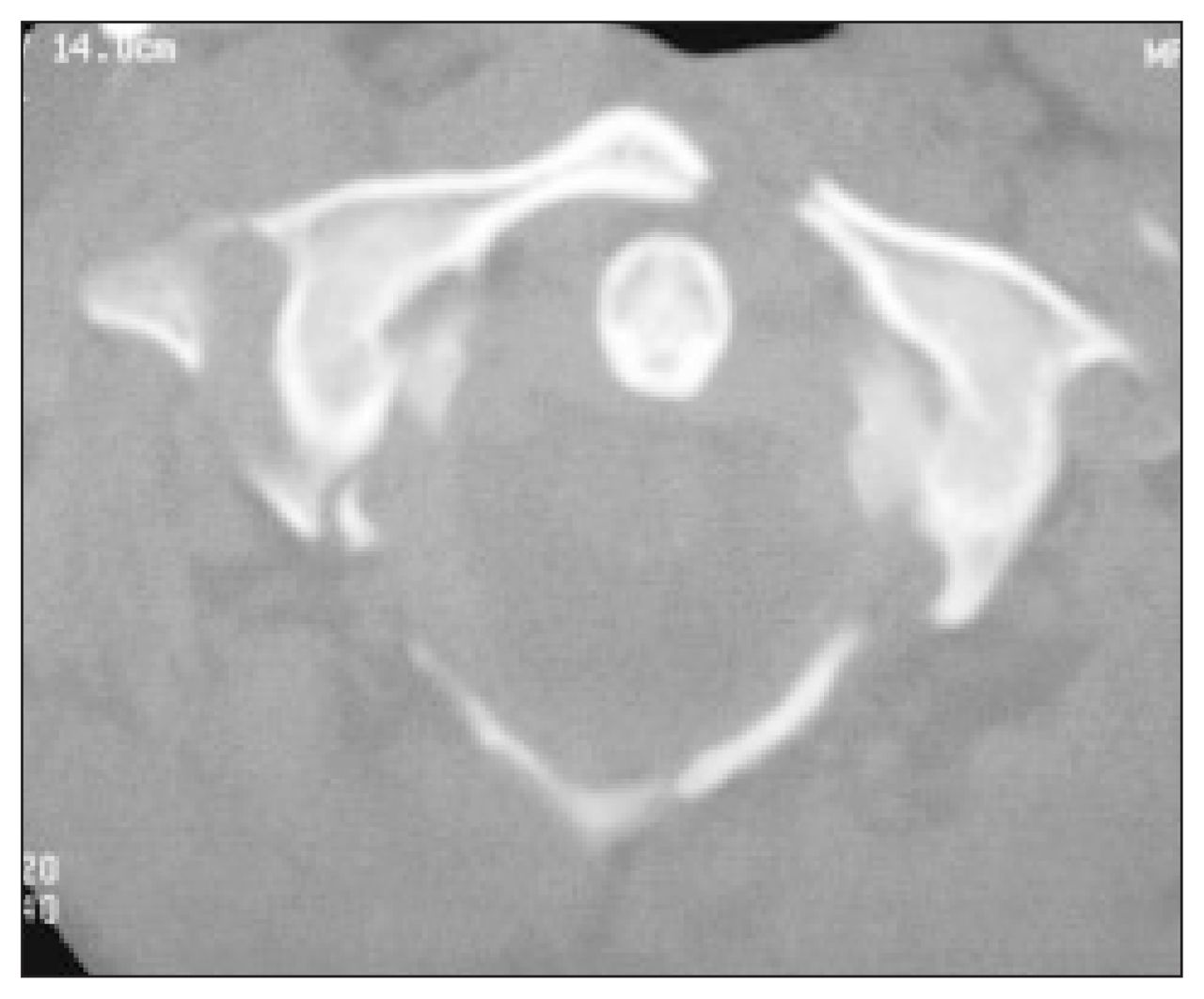
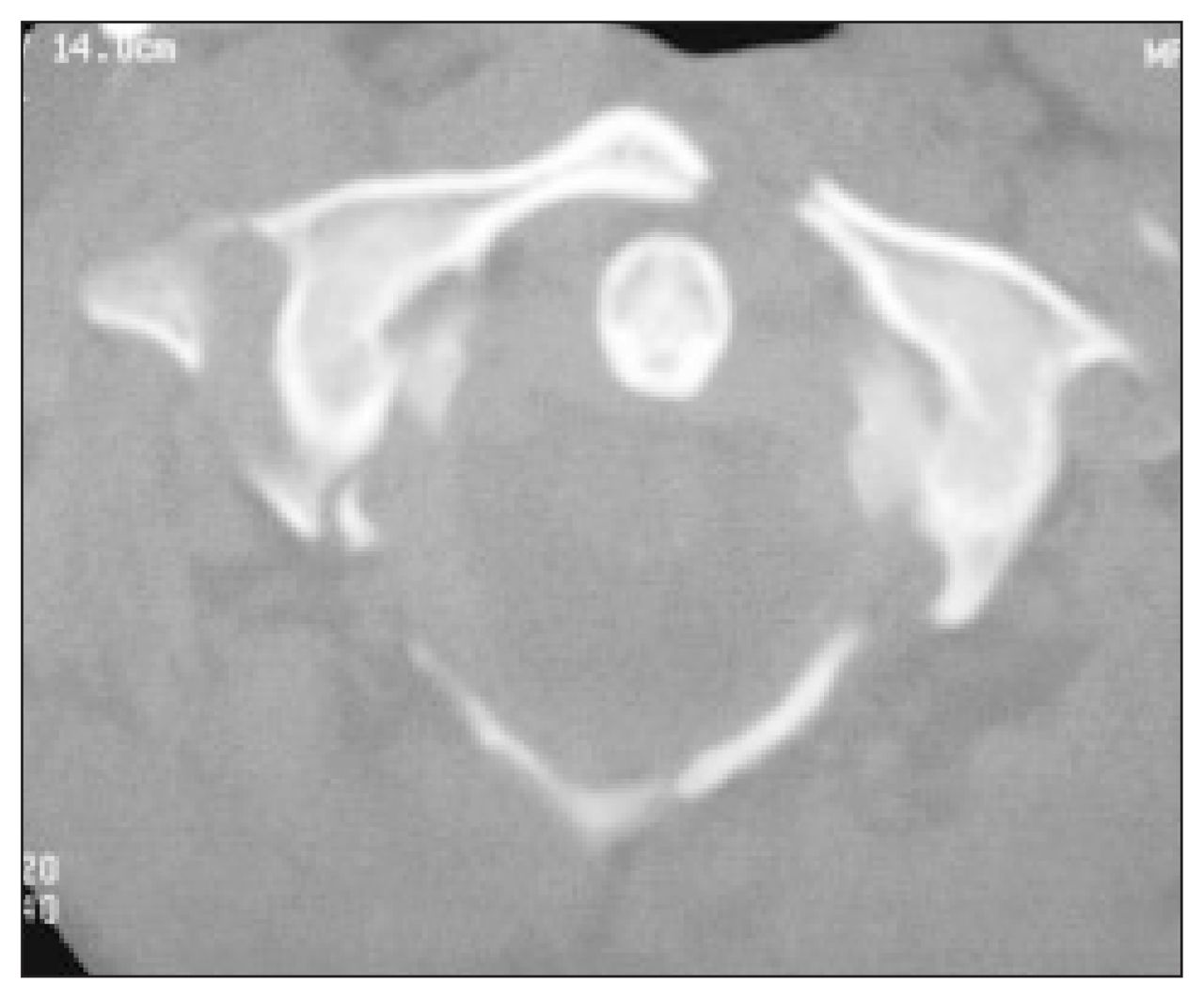
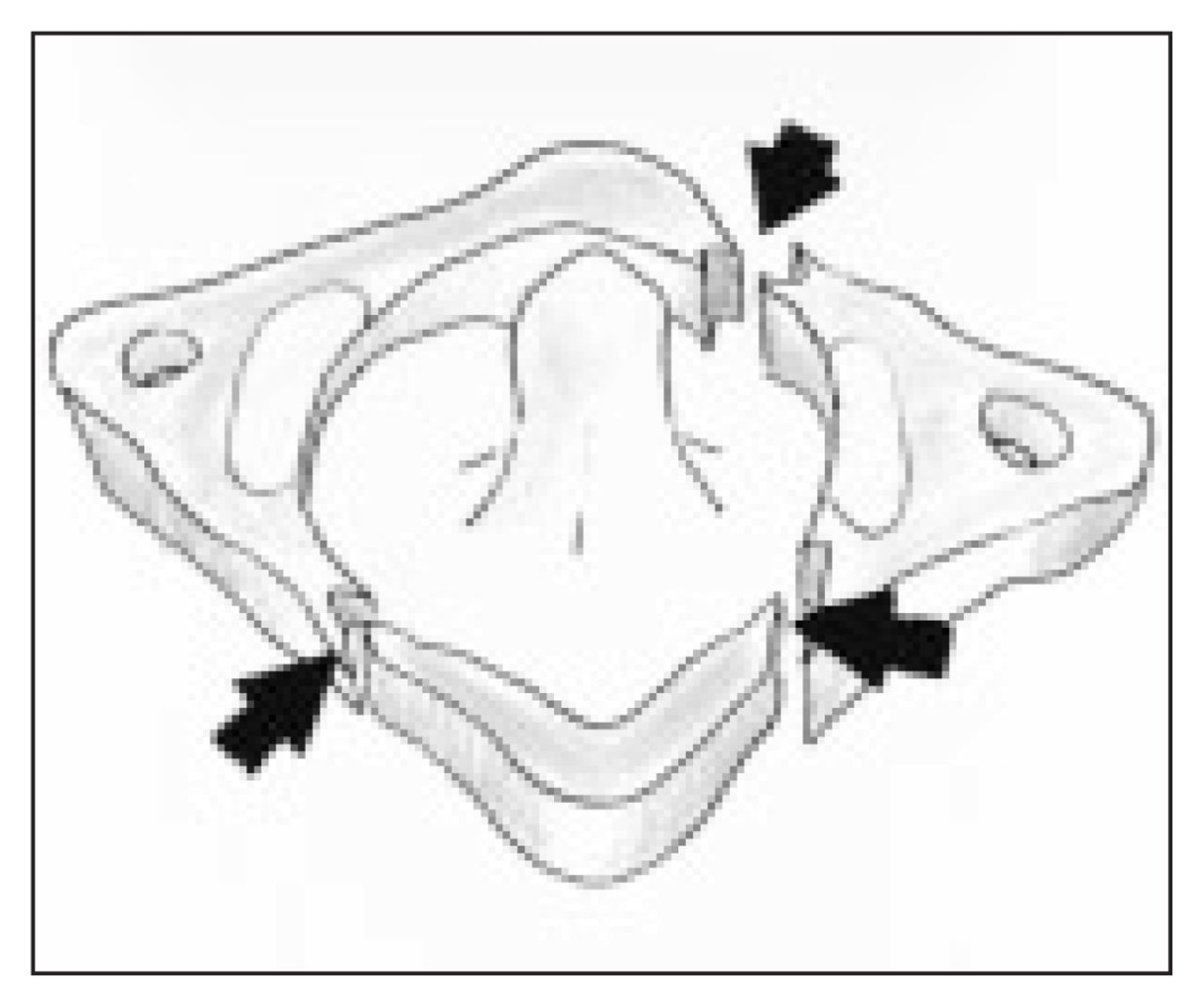
High-quality plain films of the cervical spine are essential and should always consist of 3 views: anteroposterior, lateral and openmouth (to evaluate the C1–C2 junction). Findings on plain radiographs include disruption of the spinolaminar line at C1, which is best identified on the lateral view. The anteroposterior open-mouth view is the most useful projection for detecting a Jefferson fracture. Typically, there is asymmetry and widening of the lateral spaces between the dens and the lateral masses of C1 as well as displacement of the lateral masses of C1 relative to the superior articulating facets of C2. Another sign that has been described is interposition of the basion between the anterior arch of C1 and the odontoid process as seen on a lateral radiograph.2 In a multitraumatized patient, it may be easy to miss a Jefferson fracture because of concerns about associated trauma and the general absence of neurologic signs. In addition, the open-mouth anteroposterior view, which is usually pathognomonic for the diagnosis, is often inadequate or is not obtained in such patients. If there is difficulty in visualizing the area of interest, computed tomography is recommended.3 This allows excellent detail with high spatial resolution of the osseous structures. Primary imaging is usually done in an axial (transverse) plane, and reformats are then performed in the sagittal and coronal planes. It is important to visualize the spine in all 3 planes to avoid missing a fracture. In our case, the coronal reformats precisely depicted the displacement of the articulating facets of C1 on C2 (Fig. 3). In addition, axial imaging clearly showed the fractures of the anterior and posterior elements of C1 (Fig. 4). Fig. 5 is a correlating block representation of the ring fracture of C1 identified on computed tomography in this case.

Isolated stable burst fracture of the atlas can be treated effectively with just a rigid cervical collar for 10 to 12 weeks. This is associated with good neurologic recovery and segmental stability. Unstable Jefferson fractures with concurrent unstable fracture of other cervical vertebrae, especially C2, require surgical stabilization. 4,5
Initial evaluation and management of cervical spine injuries is critically important because of the impact of early treatment and management on the prognosis.6 The devastation and cost of missing even one unstable cervical spine fracture is tremendous. A high level of clinical awareness for cervical injury should be maintained in patients sustaining injuries to the neck. In such patients appropriate imaging will usually identify the injury, leading to prompt, correct treatment, as in our patient, who had no neurologic sequelae.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.