


Abstract
Scoliosis is not simply a lateral deviation of the spine but is a complex deformity of the entire trunk. Recent advances in 3-dimensional (3-D) imaging have improved our understanding of the 3-D nature of adolescent idiopathic scoliosis (AIS) and have resulted in the development of a new generation of spinal instrumentation. Stereophotogrammetry, computed tomography, magnetic resonance imaging and surface topography all have their specific 3-D applications and relevance in the clinical management of AIS. In the near future, novel 3-D imaging applications will provide tools to guide the surgeon in the planning, performance and evaluation of increasingly sophisticated and less invasive surgical procedures, thus improving the outcome of surgical treatment for AIS.
Although it is now well recognized that scoliosis is a complex 3-dimensional (3-D) deformity of the spine, the rib cage and the pelvis, it still is defined in some textbooks as a lateral deviation of the spine. Current classification systems as well as routine radiographic clinical evaluation of adolescent idiopathic scoliosis (AIS) are still based on posteroanterior (PA) radiographic projections. Although this conventional imaging approach has proved valuable to document and follow-up surgical treatment, it only provides a 2-dimensional (2-D) representation of this 3-D deformity.
Over the last 2 decades, several new spinal instrumentations have been proposed, all claiming to achieve a true 3-D correction of scoliotic curves. However, because conventional imaging approaches fail to adequately evaluate the 3-D aspects of this deformity and its correction, new imaging approaches have been developed to help preoperative planning, intraoperative guidance and postoperative assessment of the surgical correction.
The purpose of this paper is to review recent developments in 3-D imaging techniques and to illustrate their clinical usefulness for the understanding of the 3-D nature of AIS as well as for the outcome of its surgical treatment.
Three-dimensional imaging modalities of scoliotic deformities
Stereophotogrammetry
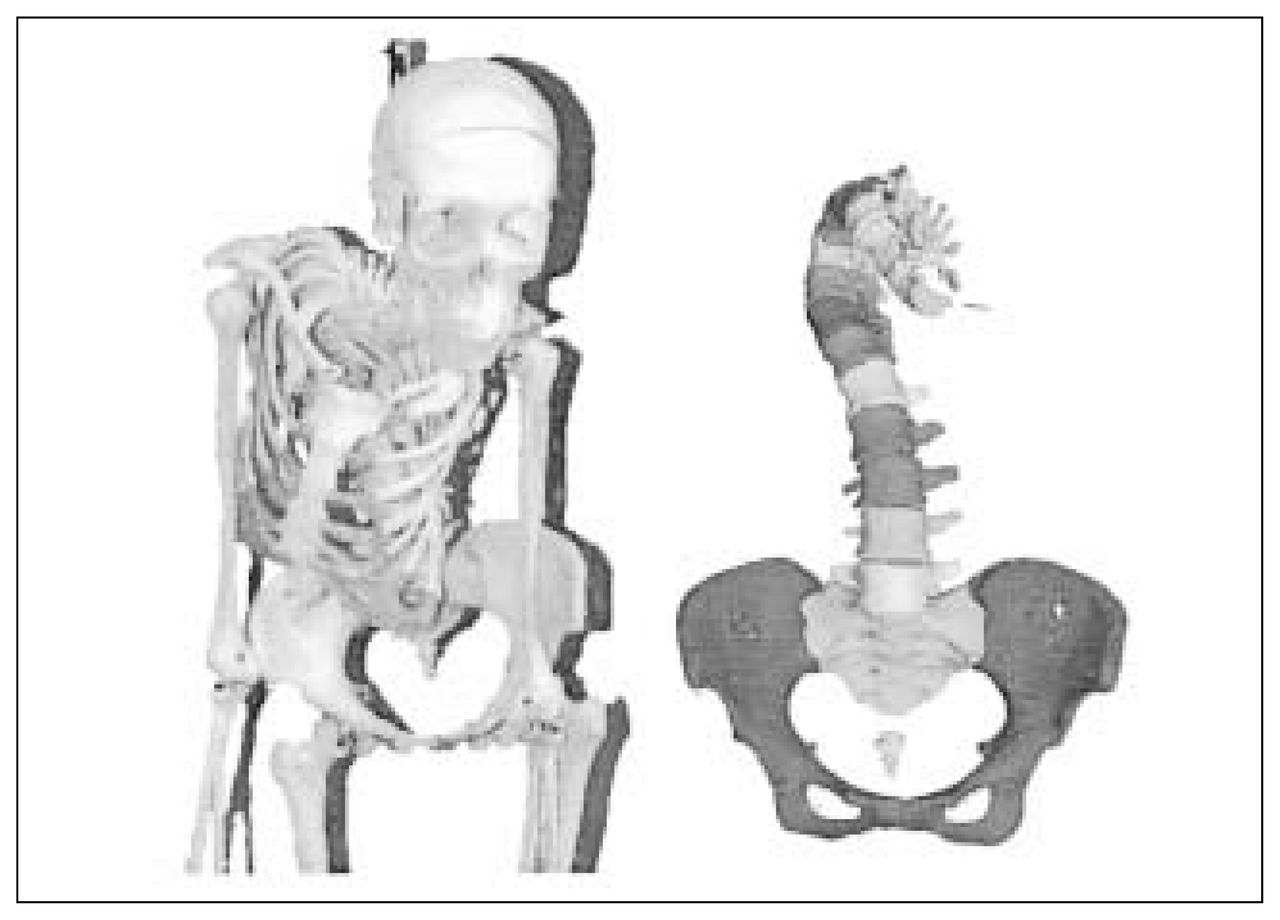
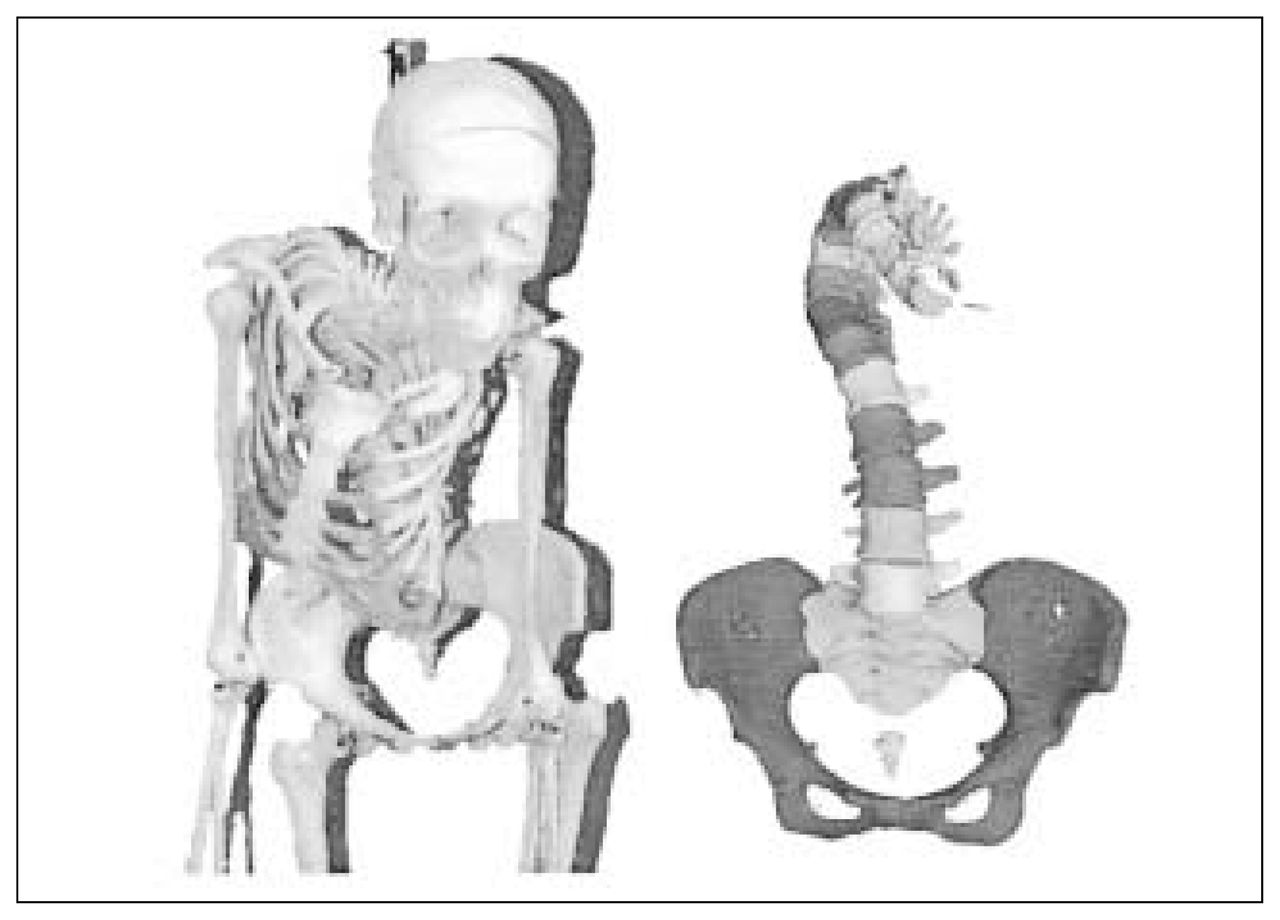
One of the most widely used imaging techniques for clinical evaluation is stereoradiography or 3-D radiographic reconstruction. This modality is a natural extension of conventional radiology since it is based on the standard PA and lateral radiographs used in clinical practice, and occasionally on additional radiographs taken from a slightly different plane. This approach generally requires an object of known dimensions, the calibration object, to be located in the 3-D space where the patient stands when radiographs are taken. Once all calibrated radiographic images have been obtained, the 2-D image coordinates of the calibration object and of various pertinent anatomic landmarks or bony contours are identified on every image. This is often done using a digitization table or computer software, providing image enhancement and analysis to semiautomatically detect image features. The relation between image coordinates and 3-D spatial coordinates of the calibration object is then defined using stereophotogrammetric algorithms such as the Direct Linear Transformation (DLT)1–9 or other nonlinear algorithms. 10,11 This relationship then defines the 2-D to 3-D projection equations used to determine the 3-D coordinates of all identified anatomic landmarks (Fig. 1 left). Stereophotogrammetry has also been applied to photographs,7,8 using similar algorithms to obtain a peroperative 3-D representation of the exposed spine. Geometric modelling techniques2 can also be useful to extrapolate several other points allowing us to refine geometric models and to enhance the visual realism of the 3-D representation of anatomical structures (Fig. 1 right). Stereophotogrammetry has several advantages. It is fairly easy to integrate in a clinical environment since it uses an imaging modality familiar to all clinicians and needs only a few adaptations. It provides a detailed geometric representation of internal bony structures that is adequate for clinical assessment of regional and global 3-D scoliotic deformities. For these reasons, it has been widely used to assess pre-, per-and postoperative changes in the shape of a scoliotic curve after surgical correction.3,4,7,8,12–14 However, this approach is less useful for documenting the complex local intrinsic deformities involved in scoliotic vertebrae. Although it has been used for the evaluation of vertebral wedging,2,9 the large number of anatomical landmarks needing identification on radiographic images is time-consuming and not accurate enough to assess other local deformities (pedicles, spinous process, and so on). Furthermore, the size of the calibration object may influence patient positioning, and is difficult to use in situations such as side bending, traction or intraoperative radiographs. Newer robust 3-D reconstruction algorithms are presently under development, aimed at reducing the size or eliminating the need for a calibration object10,11 but have not yet been implemented in clinical practice. Ethical considerations also limit this approach since the level of radiation exposure is high, and the number of calibrated radiographic images needs to be kept to a minimum, even with the introduction of digital radiography, which can significantly reduce radiation exposure. As for stereophotography, this imaging modality has the advantage of being noninvasive while its accuracy is similar to stereoradiographic techniques. It can also provide an accurate description of the 3-D shape of the scoliotic trunk but cannot be used to model internal bony structures.

Three-dimensional representation of the spine, the rib cage and the pelvis of a scoliotic patient. Left: wire-frame representation. Right: surface representation of the refined 3-D geometric model.
Surface topography
The first sign most commonly noticed by a scoliotic patient is asymmetry of the back caused by a rib prominence. The goal of treatment is to prevent progression of this visible deformity as well as of the underlying skeletal one. The purpose of surface topography is to quantify 3-D surface deformities of the scoliotic trunk. Recent imaging devices make it possible to obtain a 3-D reconstruction of surface shape from scanned light15,16 or stereophotography, 17 creating detailed and realistic 3-D surface representations of the trunk (Fig. 2) and allowing 3-D study of external scoliotic trunk deformities. Thus, this modality is complementary to radiographic techniques and may correlate more closely with the patient’s perception of deformity. More specifically, it allows us to quantify right–left asymmetry of the trunk and rotational prominences produced by the rib cage. Surface topography also has the advantage of reducing patient exposure to radiation by avoiding the use of radiographs during clinical examinations. 17 Because surgeons are so familiar with Cobb angle measurements on radiographs, the introduction of new surface shape measures whose meaning may not be readily apparent to clinicians has been difficult. Furthermore, any measure inferred about the bony spine is indirect, and the exact relation between the surface shape of the trunk and the spinal scoliotic deformity still needs to be clarified.

Three-dimensional representation of the back of a scoliotic patient obtained by surface topography. Left: surface representation. Right: with texture.
Computed tomography and magnetic resonance imaging
Computed tomography (CT) and magnetic resonance imaging (MRI) are of great interest for imaging specific types of scoliotic deformities. Since both modalities produce a series of detailed images of the bony anatomy (CT) and soft tissues (MRI), they are widely used to assess the presence of a congenital anomaly or a spinal dysraphism, when a congenital or neurologic abnormality is suspected. Because of the detailed information provided by these techniques, they are also ideal for quantifying intrinsic deformities involved in AIS18,19 (Fig. 3). However, they are not as suitable for visualizing the global change in shape of the entire spine. The natural profile of AIS is difficult to obtain since images are produced with the patient in the supine position. MRI is time-consuming, and the presence of metallic implants, once surgery has been performed, produces artifacts and creates suboptimal images. CT allows adequate pre- and postoperative images but can be used only for short spinal segments owing to the high radiation exposure involved. These drawbacks limit the use of CT and MRI for applications where refined imaging of localized deformities is needed.
Analysis of intrinsic deformities of a scoliotic specimen. Left: photographic representation. Right: geometric representation of the spine obtained from three-dimensional analysis of the computed tomographic scans.
Clinical relevance of three-dimensional scoliotic models
All these 3-D imaging modalities have allowed researchers and clinicians to better understand the 3-D nature of AIS and the complex deformities involved. Asher and Burton, 1 Poncet and colleagues20 and Tredwell and colleagues8 have shown that scoliosis induces a geometric torsion of the spine. The plane of maximum curvature has been recognized as a useful and simple 3-D index to describe the rotation in the transverse plane of the scoliotic curve.3,4,6,8,14 Other studies have also characterized the intrinsic deformities involved in AIS such as wedging of the vertebral body,2,9,18 asymmetry of pedicles19 and articular facet joints and deviation of the spinous process from the midline of vertebrae. These studies have clearly shown the 3-D nature of AIS and have proven the importance of 3-D imaging to fully describe scoliotic deformities and adequately evaluate surgical treatment.
The concept of AIS as a 3-D deformity directly related to the early use of 3-D imaging by Dubousset21 led to the development of a new generation of multisegmental spinal instrumentation designed to provide 3-D correction. Cotrel–Dubousset instrumentation (Sofamor-Danek, Mississauga, Ont.) was the first of these. It introduced the concept of the “rod rotation manoeuvre” to produce axial derotation of the apical vertebra. Further 3-D clinical evaluations4,8 have shown that this procedure effectively achieves 3-D correction but by a change in orientation of the plane of maximum curvature rather than by axial derotation of the apical vertebra. Subsequently, several other 3-D spinal instrumentation systems such as Colorado (Sofamor-Danek), Universal Spine System (Synthes Spine Company, Paoli, Penn.) or Isola (DePuy Acromed, Raynham, Mass) have appeared on the market, claiming to be more versatile and user-friendly, and providing better 3-D correction. Introduction of these new systems forced a confrontation between 2 principles of correction: rod rotation and segmental translation. Delorme and associates3,14 have recently shown that the Colorado instrumentation system has achieved a slightly better correction in the frontal plane than the Cotrel–Dubousset system, but that both have achieved similar changes in orientation of the plane of maximum curvature. They attributed this difference to the significantly greater proportion of pedicle screws used in the Colorado instrumentation system. Sawatsky and colleagues7 found that increasing the number of hooks enhanced the correction of scoliotic deformities, supporting the findings of Delorme and associates3,14 but also suggesting that 3-D assessment of surgical correction may influence surgical strategies. Wemyss-Holden and colleagues16 confirmed that Cotrel–Dubousset instrumentation achieves a good, stable correction of the Cobb angle and the segmental vertebral tilt but provides limited vertebral derotation. However, they also reported that the surface shape of the back expressed by segmental measures of the angle of trunk inclination (ATI) continues to progress at 1 year follow-up and suggests that deforming forces in AIS continue to act on the rib cage after surgery. This observation also indicates that all aspects of scoliotic deformities (3-D skeletal deformity as well as surface deformity and imbalance of the trunk) should be evaluated during the planning of scoliosis treatment and the follow-up. Older instrumentation systems such as the Harrington system are associated with the “flat-back” syndrome,22,23 but recent 3-D clinical evaluations3,4,7,12,14 have reported a good recovery of the natural curves in the sagittal plane after the surgery suggesting that the incidence of flat-back syndrome may be reduced in long-term follow-up. This requires further study because the use of 3-D systems is fairly recent, and confirmation that they can improve the long-term functional outcome is not yet available.
Three-dimensional imaging modalities provide greater information to clinicians than the standard methods but are more difficult to understand. Traditional terminology and classification systems are based on 2-D imaging techniques, which do not adequately describe the 3-D nature of scoliotic deformities. Therefore, the Scoliosis Research Society has struck a committee to establish a 3-D terminology of spinal deformity.24 Attempts have been made to develop a 3-D classification of AIS,1,20 but so far none has been generally accepted.
Emerging applications of three-dimensional imaging in scoliosis treatment
Three-dimensional imaging has definitely influenced the way surgeons perceive scoliotic deformities and the manner in which they plan and evaluate the treatment of AIS. This also applies to surgical procedures, which are becoming increasingly computerized. Image-guided surgery, also known as computer-aided surgery or frameless stereotaxis, provides an intraoperative view of anatomic structures located beneath the exposed part of the spine.
Placement of pedicle screws was the first application of image-guided scoliosis surgery. Preoperative CT scans or MRI images are the basic input to computer-aided surgery. In most of the proposed approaches,25,26 these images are used to compute a refined 3-D representation of the vertebrae where screws are to be inserted. During surgery, optoelectronic26,27 or electromagnetic25 3-D position sensors are used to first register the virtual model and the real vertebra (i.e., to correlate the virtual model with the intraoperative position of the vertebra). Other applications correlate the radiographic images to monitor the movement of the tool projected on selected radiographic27 or fluoroscopic28 images. Once this has been done, movements of the instrumented vertebra and of the instrumentation tools are monitored in real-time. These operations allow direct visualization of the drilling tool and the screw entering the pedicle. Recent clinical studies25–27 have shown that computer-assisted insertion of a pedicle screw is more accurate and safe than conventional techniques, even in the high thoracic area. Amiot and associates25 and Laine and colleagues27 have shown that computer-assisted insertion of pedicle screws significantly reduces the risk of neurologic injury.29 However, in its current stage of development, this technology is not user-friendly and appears most useful when the anatomy is unusual or complex. Several improvements are underway to eliminate the need for CT scans and decrease the time needed for registration, so computer-aided surgery will likely continue to gain popularity and new applications for scoliosis surgery will be developed. By adding 3-D position sensors on selected vertebrae and anatomical landmarks on the trunk in addition to surgical instruments, this technology has the potential to become a sophisticated and powerful method to monitor intraoperatively the change in shape of the scoliotic curve30 as well as the overall shape and balance of the trunk,31 providing the surgeon with real-time feedback. This should give the surgeon a better idea of the overall correction achieved and may improve the final outcome.
Minimally invasive surgery is another potential area for the application of 3-D imaging techniques. Surgical procedures by an anterior approach for AIS (discectomy and anterior fusion) are usually achieved by open thoracotomy. Video-assisted thoracoscopic surgery (VATS) has been widely used for nonspinal conditions but is a more recent introduction for spinal deformities.29,32,33 Despite some concerns about its use in very small children and for severe scoliotic deformities, the indications for VATS in the treatment of AIS are similar to those for open thoracotomy surgery,33,34 with the advantages of smaller incisions and decreased morbidity.32 Although the learning curve for VATS is high, it is a safe and effective alternative to open thoracotomy, and it is likely that imaging techniques will help to enhance the surgeon’s 3-D visualization of anterior spinal structures.
Finally, with the emergence of novel multisegmental spinal instrumentations for the treatment of AIS, surgical procedures are becoming increasingly complex, requiring that many parameters be determined pre-and intraoperatively. Despite a large number of clinical publications, there is no consensus on the optimal selection and placement of implants, and the outcome of surgery may differ accordingly. Biomechanical models (Fig. 4) are powerful tools to simulate the effect of various surgical strategies and procedures on the outcome of the surgical treatment. They avoid the need for in-vivo testing on patients or animals. For example, using such a tool, the surgeon could test several surgical strategies for a particular patient during his preoperative planning process to reduce the number of instrumented levels while obtaining a good biomechanical balance both in frontal and sagittal planes. 3-D imaging has an important role in the development of accurate, reliable biomechanical predictive models for spinal surgery. For such models patient-specific geometry and mechanical properties are important, and patient-specific information for recent models has been obtained through 3-D imaging.2,6 However, the mechanical properties of these models are generally obtained from in-vitro experiments on cadaver specimens and do not adequately represent patient-specific mechanical properties. Lateral bending or traction radiographs are commonly used in the planning of surgical treatment for AIS to predict the degree of surgical correction required and to determine levels of instrumentation. With novel 3-D imaging techniques, these tests will likely evolve to provide 3-D information on the mobility of the spine5 in relation to external loads applied. Such information will allow surgeons to improve the planning of surgery with a biomechanical simulation tool better suited to the 3-D nature of the deformity and of new segmental instrumentation techniques.

Biomechanical simulation of Cotrel–Dubousset instrumentation, with simulation at 3 stages of the surgical procedure. Left: placement of the hooks and screws. Centre: rod insertion (translation). Right: rod rotation manoeuvre.
Conclusions
Recent advances in imaging have provided a better understanding of the 3-D nature of AIS. Stereophotogrammetry, surface topography, CT and MRI are being used more frequently to generate accurate 3-D virtual images and to quantify scoliotic deformities that have improved the 3-D assessment of AIS surgical correction. New emerging 3-D imaging applications will soon provide sophisticated tools to guide the surgeon in the planning, performance and evaluation of surgical treatment. The appropriate management of AIS still relies on the clinical expertise of surgeons, but novel 3-D imaging techniques are a natural extension of the surgeon’s eyes and hands, allowing the surgeon to perform sophisticated, less invasive surgical procedures and eventually to improve the outcome of surgical treatment.
Acknowledgements
We acknowledge the support of the Canadian Foundation for Innovation and the Canadian Institutes of Health Research.
- Accepted October 17, 2001.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.