


Cecal diverticulitis
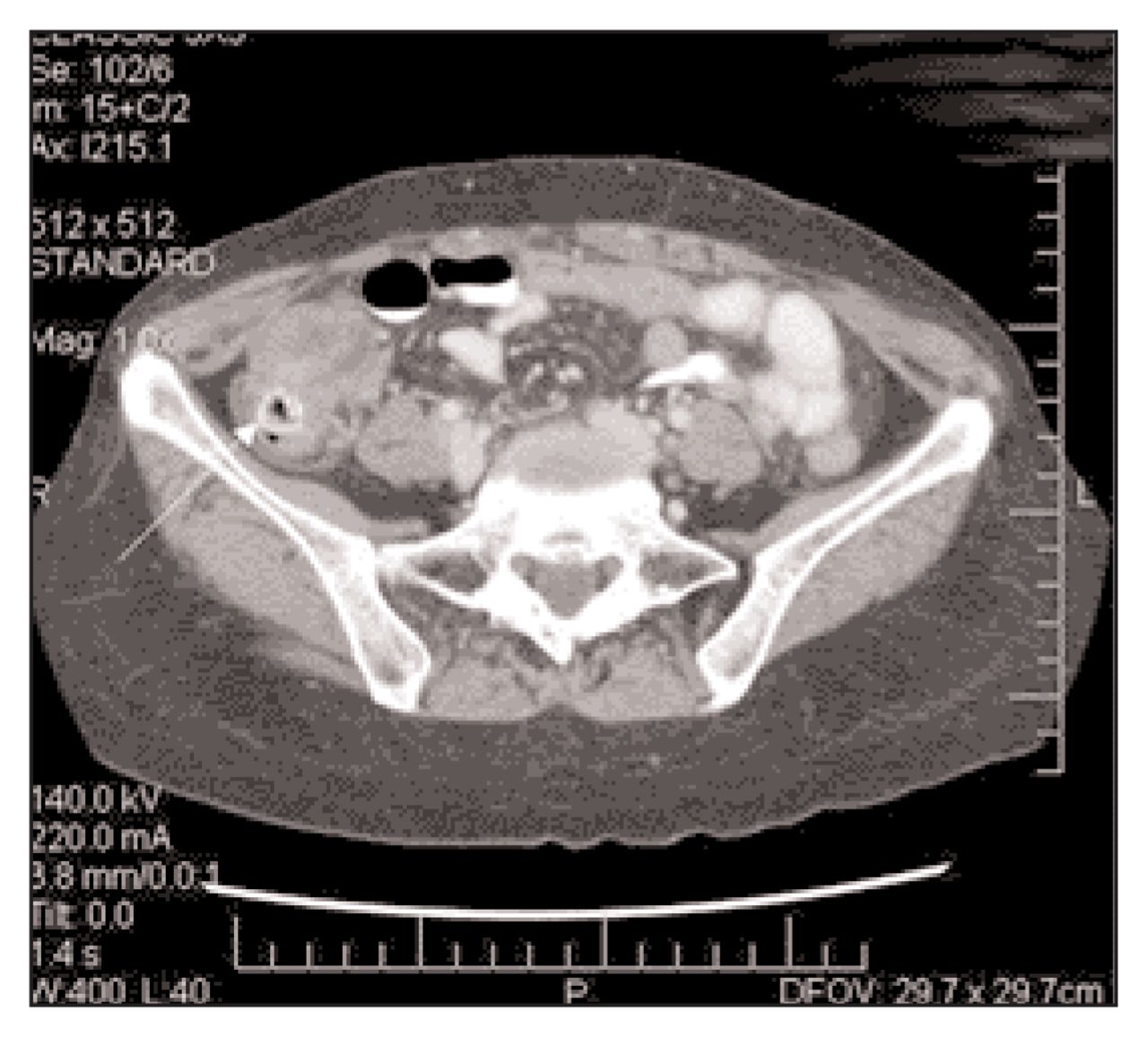
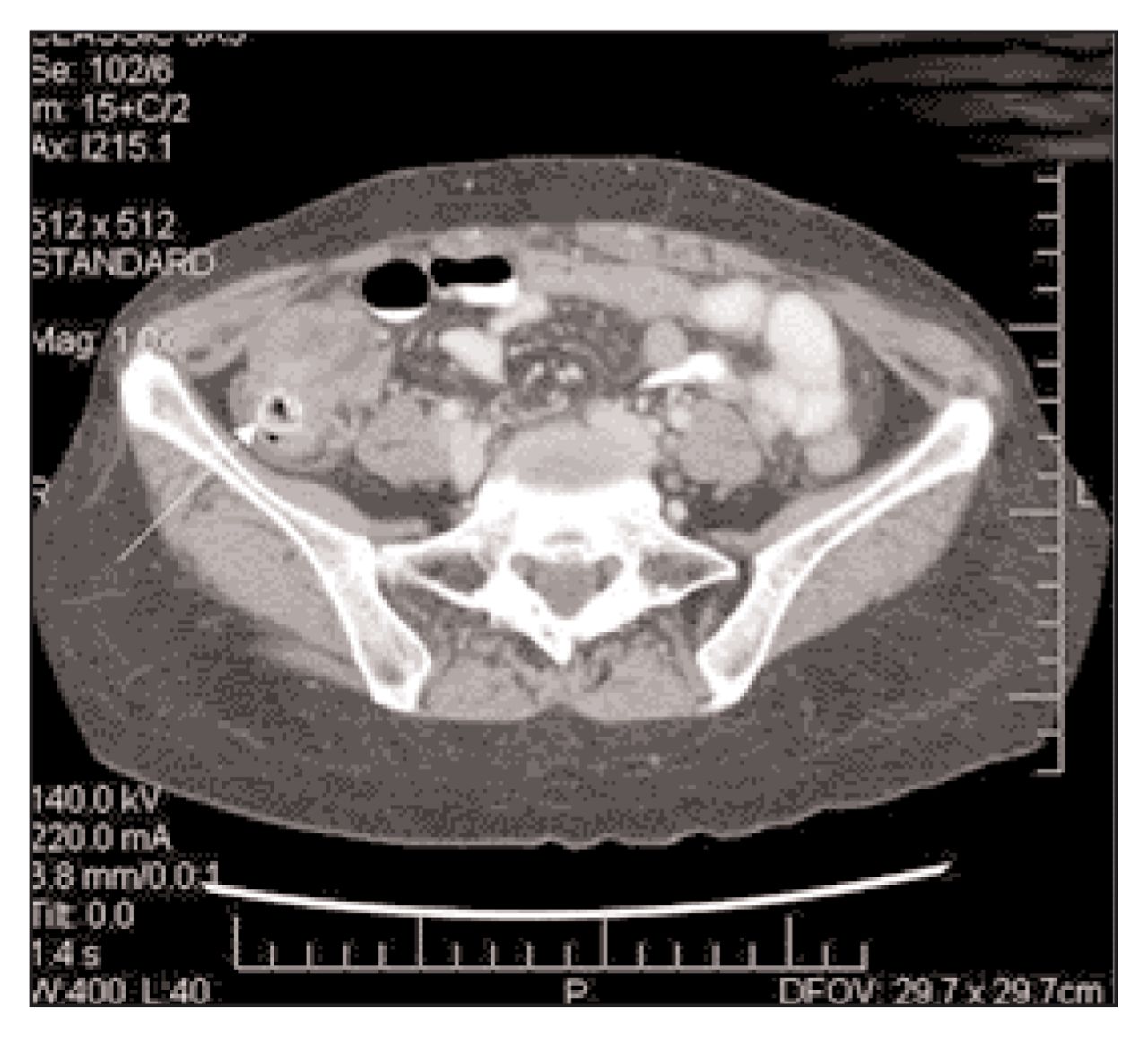
On computed tomography there was extensive soft-tissue swelling of the cecum with a calcified fecalith (Fig. 2, arrow), which suggested diverticulitis. The patient was treated conservatively with antibiotics, and a few days later underwent a water-soluble contrast enema examination to exclude malignant disease of the cecum. This examination revealed a solitary cecal diverticulum with no evidence of malignant cells. She recovered with antibiotic therapy. At follow-up computed tomography 6 weeks after discharge from the hospital her cecum appeared normal with complete resolution of the inflammation (Fig. 3).

Cecal diverticulitis, which was first described in 1912 by Poitier,1 is more common in people of Asian descent than others.2–5 In a review of more than 6000 emergency laparotomies, the incidence of cecal diverticulitis was estimated at 1 in 500 cases.6 Because of its rarity, cecal diverticulitis is more likely to be diagnosed as acute appendicitis at the time of presentation. The clinical presentations of the 2 conditions are so commonly mistaken, that a correct preoperative diagnosis is made in only 0–24% of patients.4,7
Controversy exists in the literature about the pathogenesis of right-sided diverticula. In Western populations, most cecal diverticula are solitary and therefore believed to be true or congenital diverticula (containing all 3 layers of the colonic wall).2,3,5,7,8 In Asian populations, however, right-sided diverticula are multiple and thought to be false or acquired (containing only mucosal herniations through the muscularis propria).2,3,5–7 In support of the latter theory, Sugihara and colleagues9 conducted a study that measured the intraluminal pressures of the ascending colon in patients with right-sided diverticula. They found that these patients had a greater motility index than normal subjects and suggested that diverticula of the cecum and ascending colon may be acquired in a similar fashion to left-sided diverticula.
Patients with cecal diverticulitis are commonly in their mid-40s in age, and the ratio of men to women is 2:1.5,10 Most patients present with subacute right lower quadrant pain and localized peritoneal signs. Nausea and vomiting are less frequent, and systemic symptoms are often absent. 2,4,5 Because of these nonspecific clinical findings, it is easy to confuse cecal diverticulitis with other causes of right lower quadrant pain such as acute appendicitis (most commonly), cecal carcinoma, inflammatory bowel disease, infectious colitis, appendiceal carcinoid and gynecologic disorders in women.10 It is critical to differentiate diverticulitis from a primary cecal malignant lesion preoperatively because the distinction is far from clear at operation: more than 40% of patients are reported to undergo a right hemicolectomy because of a presumed malignant lesion.5
To make a correct preoperative diagnosis, computed tomography with intravenous and oral contrast is the imaging test of choice.5,11–13 The most common findings are inflamed diverticula, usually at the level of maximum colonic wall thickening and peridiverticular inflammation with or without extraluminal air or abscess formation. The contents of the diverticula can be viscous or calcified. The latter must be differentiated from appendicoliths. If a normal appendix is identified, appendicitis can confidently be ruled out.5,12,13 Oudenhoven and associates2 attempted to classify the findings of right-sided diverticulitis: stage 0 is the presence of an inflamed diverticulum containing a fecalith, thickened colonic wall and surrounding inflamed mesentery; stage 1 is evacuation of the contents of the diverticulum either directly or via an abscess; and stage R is gradual resolution of the inflammatory changes. It is the staging of the diverticulitis at the time of presentation that guides the patient’s management.
The treatment for cecal diverticulitis has ranged from expectant medical management (similar to uncomplicated left-sided diverticulitis) to right hemicolectomy.3 Most surgeons agree that if the diagnosis is made preoperatively, a trial of conservative management with antibiotics given intravenously is warranted. However, there is considerable controversy surrounding the surgical trreatment of cecal diverticulitis found at laparotomy. Reports from Hawaii14 and Singapore, 15 where the majority of patients are of Asian descent, have favoured a conservative surgical approach, involving a prophylactic appendectomy and leaving nonperforated diverticular disease in situ. The reported complication and recurrence rates with subsequent medical therapy were low.7 A report from main-land United States recommended resection of all gross disease, with favourable results.8
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.