


The purpose of this report is to describe an unusual case of diverticular abscess in which the physical presentation and radiographic findings were atypical.
Case report
A 73-year-old man presented with bilateral shoulder discomfort. Although the onset of his discomfort seemed to be associated with exertion, there was no chest pain. A month later, a stress test reproduced the shoulder discomfort but again without chest pain. Angiography showed significant coronary artery disease, so the patient was booked for coronary artery bypass grafting 2 months later.
Routine preoperative chest radiography showed free intra-abdominal air, so the bypass procedure was cancelled pending investigations.
The patient had no complaints of abdominal pain, fever, chills, anorexia, nausea or vomiting. His abdomen was distended and tympanitic, but there was no tenderness or palpable masses.
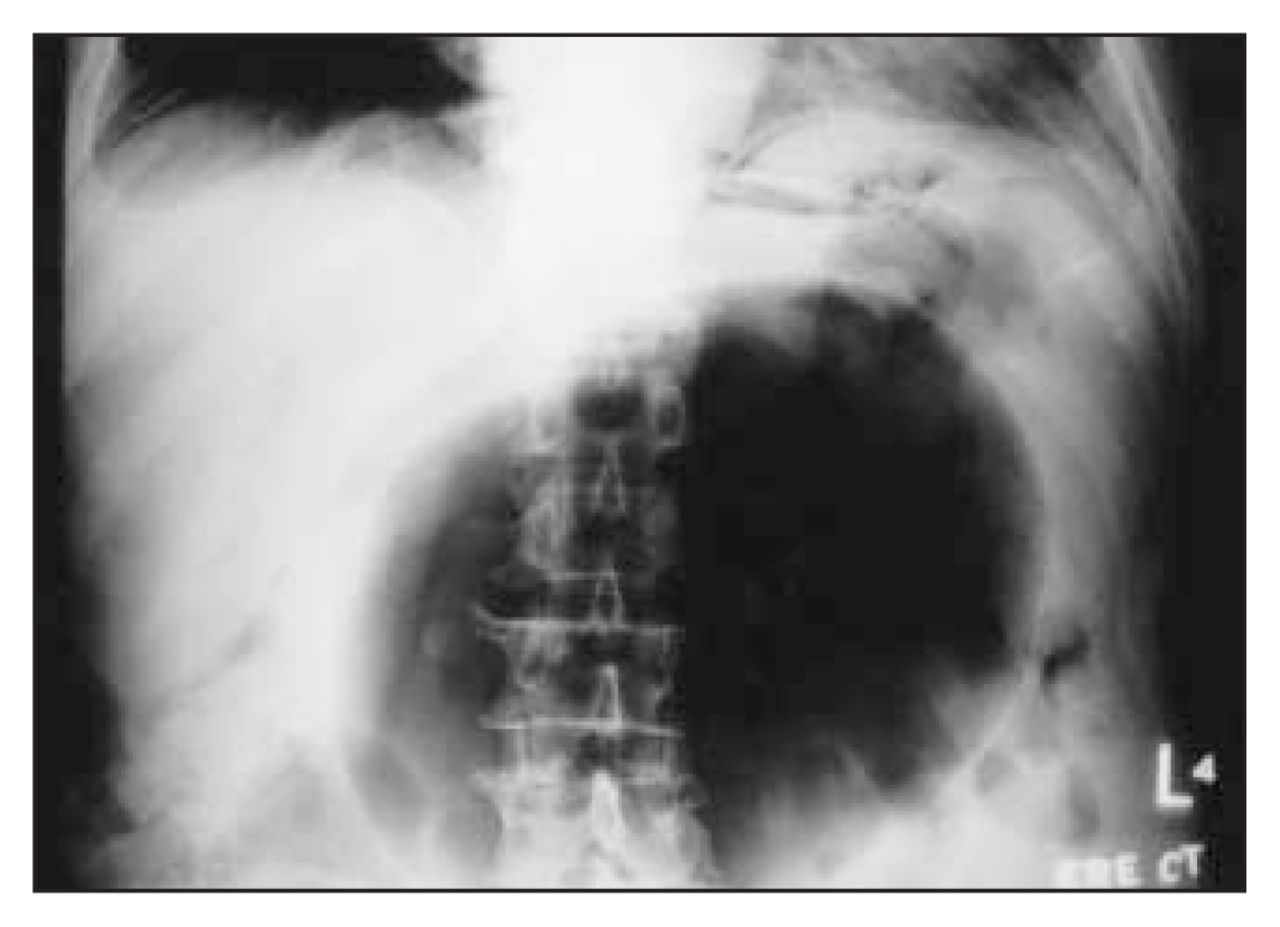
Abdominal radiography showed a large, central, gas-filled cavity occupying much of the abdomen and displacing the small bowel (Fig. 1).
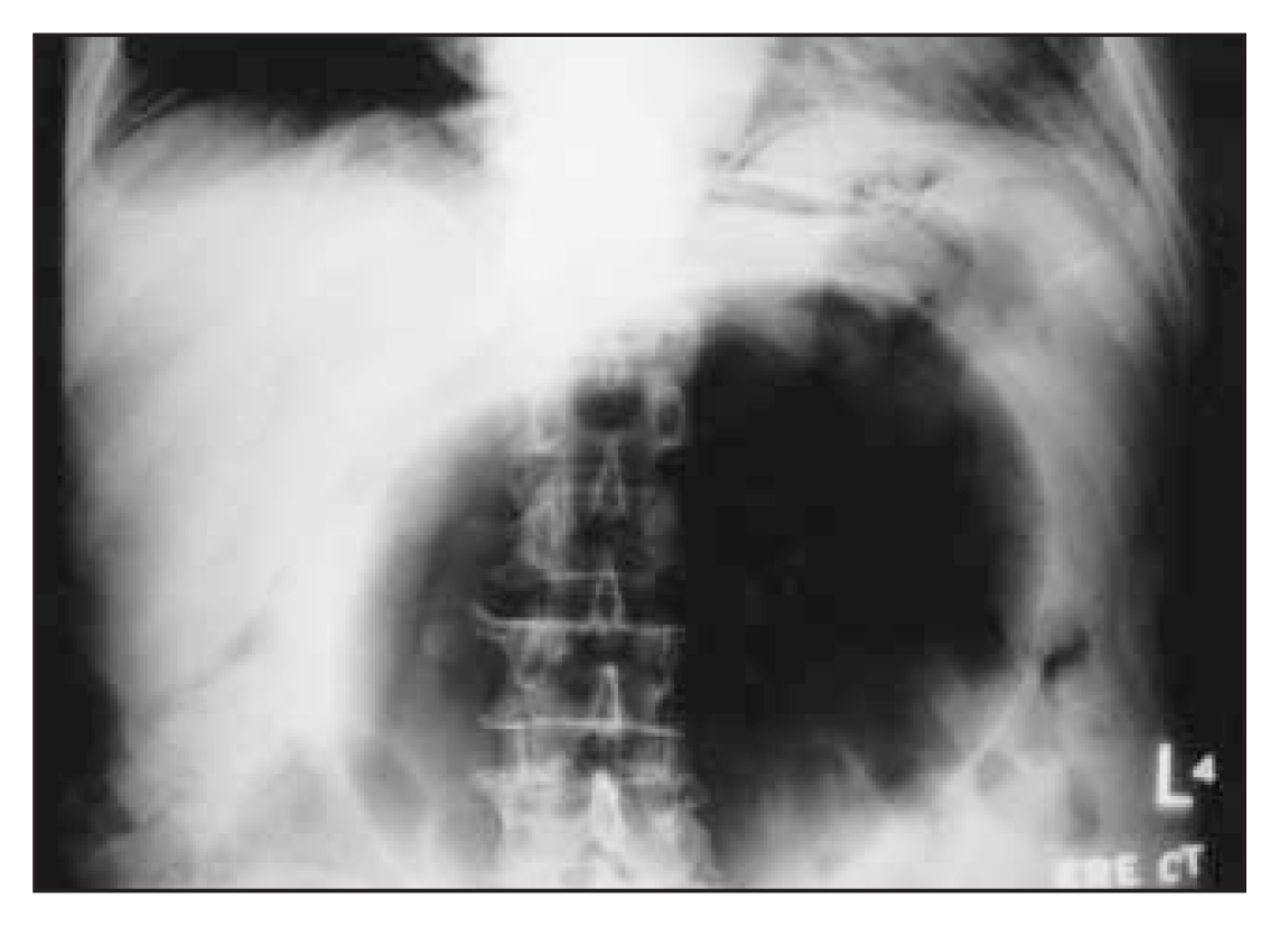
Radiograph shows a large air-filled cavity occupying much of the abdomen.
Subsequently a fever developed (body temperature 38.4°C). The leukocyte count was 17.2 × 109/L, but no organisms grew on blood culture. Antibiotics were started.
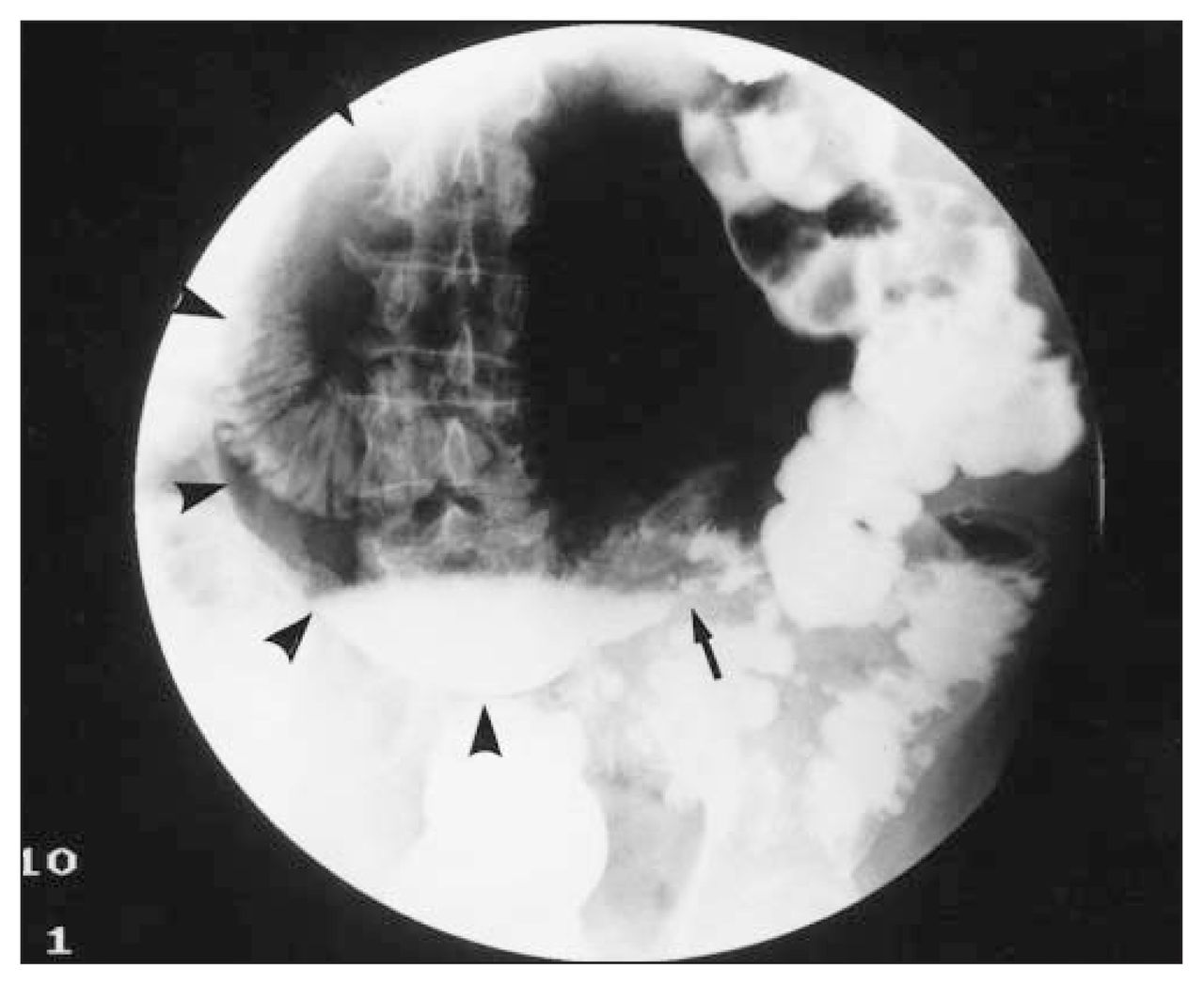
An upper gastrointestinal series with Gastrografin contrast medium appeared normal, but a large-bowel study showed sigmoid diverticular disease with contrast medium in the cavity (Fig. 2). The differential diagnosis was giant diverticulum of the colon or abscess secondary to perforated diverticulitis.
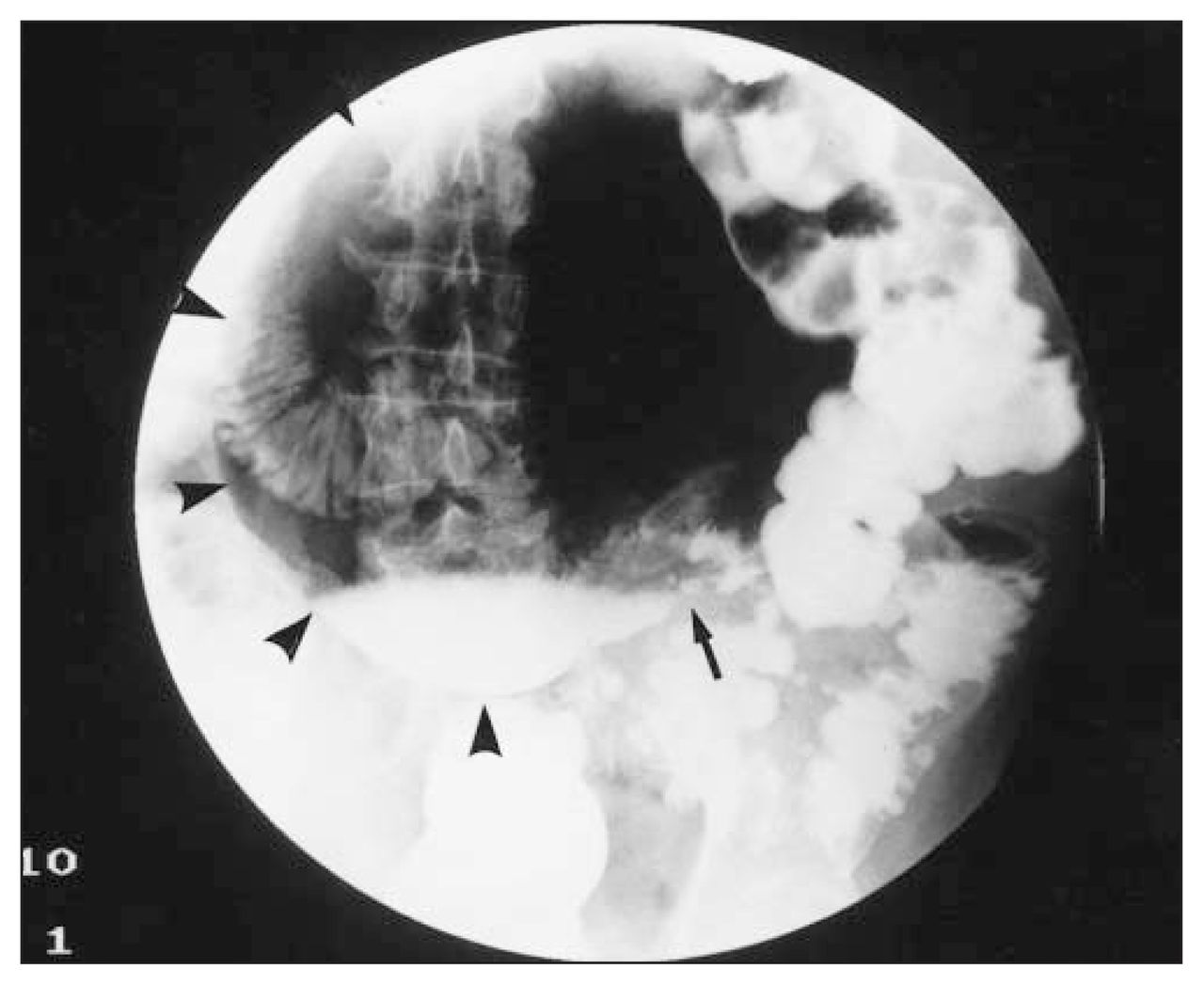
Abdominal film shows diverticular disease and a large mass (arrowheads) containing contrast medium and displacing the large bowel. The arrow indicates a possible point of communication between the cystic mass and the sigmoid colon.
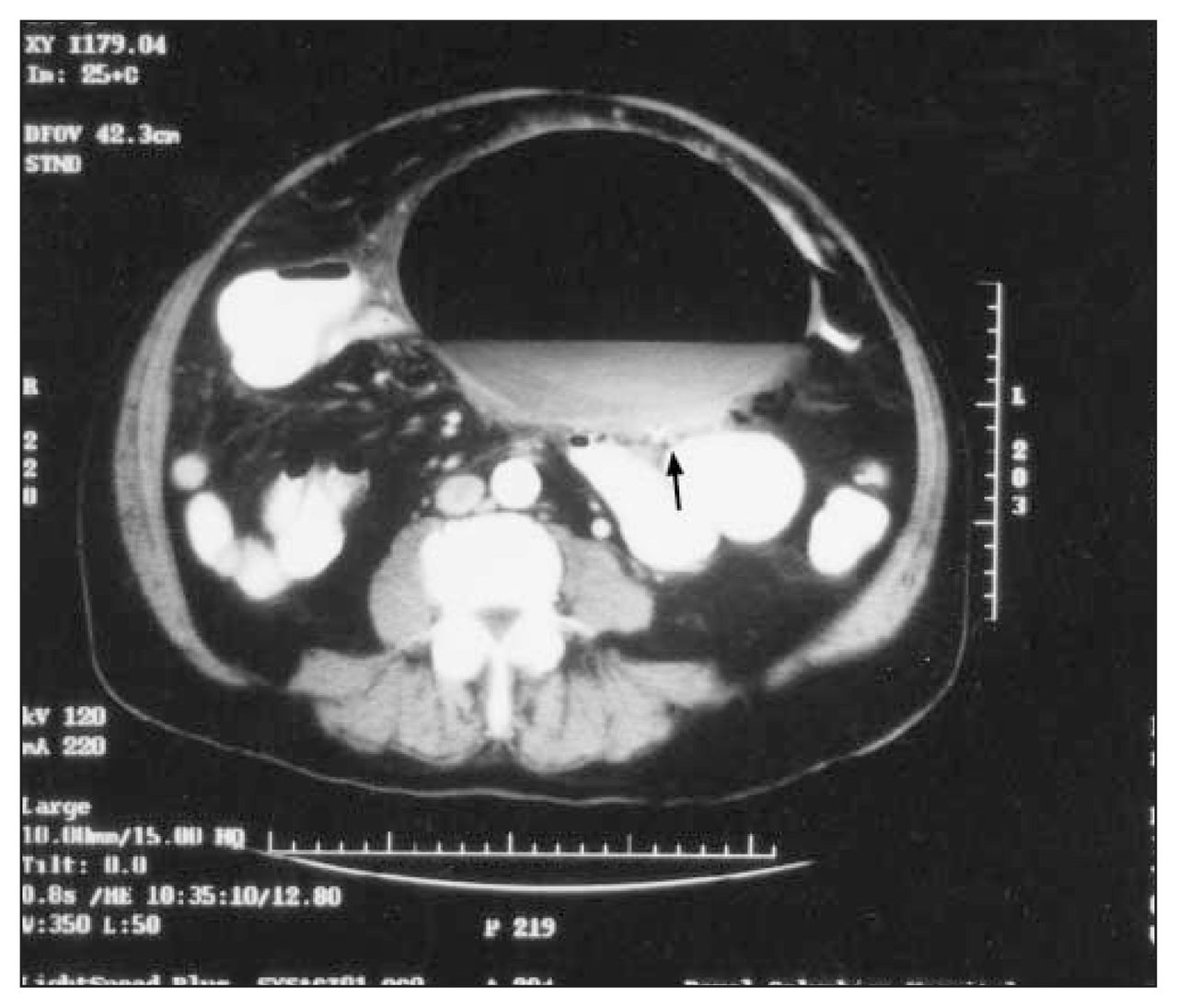
Computed tomography confirmed presence of a large, thin-walled cavity with air–fluid levels (Fig. 3) and a possible communication with the sigmoid colon.

Computed tomography shows a thin-walled cystic cavity with air–fluid levels and a possible communication with the sigmoid colon (arrow).
Laparotomy revealed a 20-cm thick-walled mass adherent to the transverse mesocolon and root of the small-bowel mesentery. It connected to the sigmoid colon and was filled with pus and air. A Hartmann resection was performed. Gram’s staining of tissue from the mass was not contributory, but coliform organisms grew on culture. Pathological examination confirmed that the cyst was an abscess cavity containing vegetable material consistent with intestinal content. The findings in the sigmoid colon were consistent with a perforated diverticulitis.
The patient’s shoulder pain on exertion diminished significantly postoperatively. In light of his improved symptoms, the coronary artery bypass procedure was postponed.
- Accepted October 22, 2002.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.