


Colonic gallstone ileus
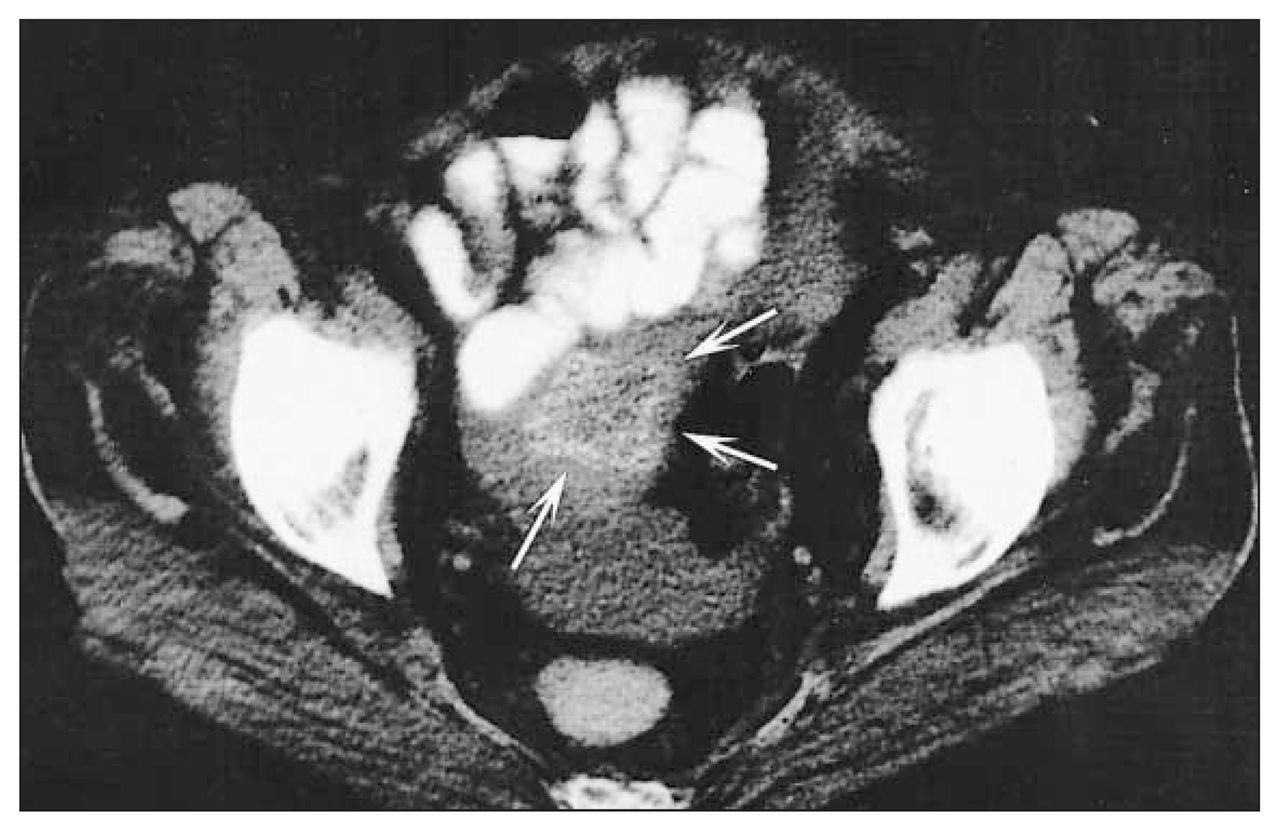
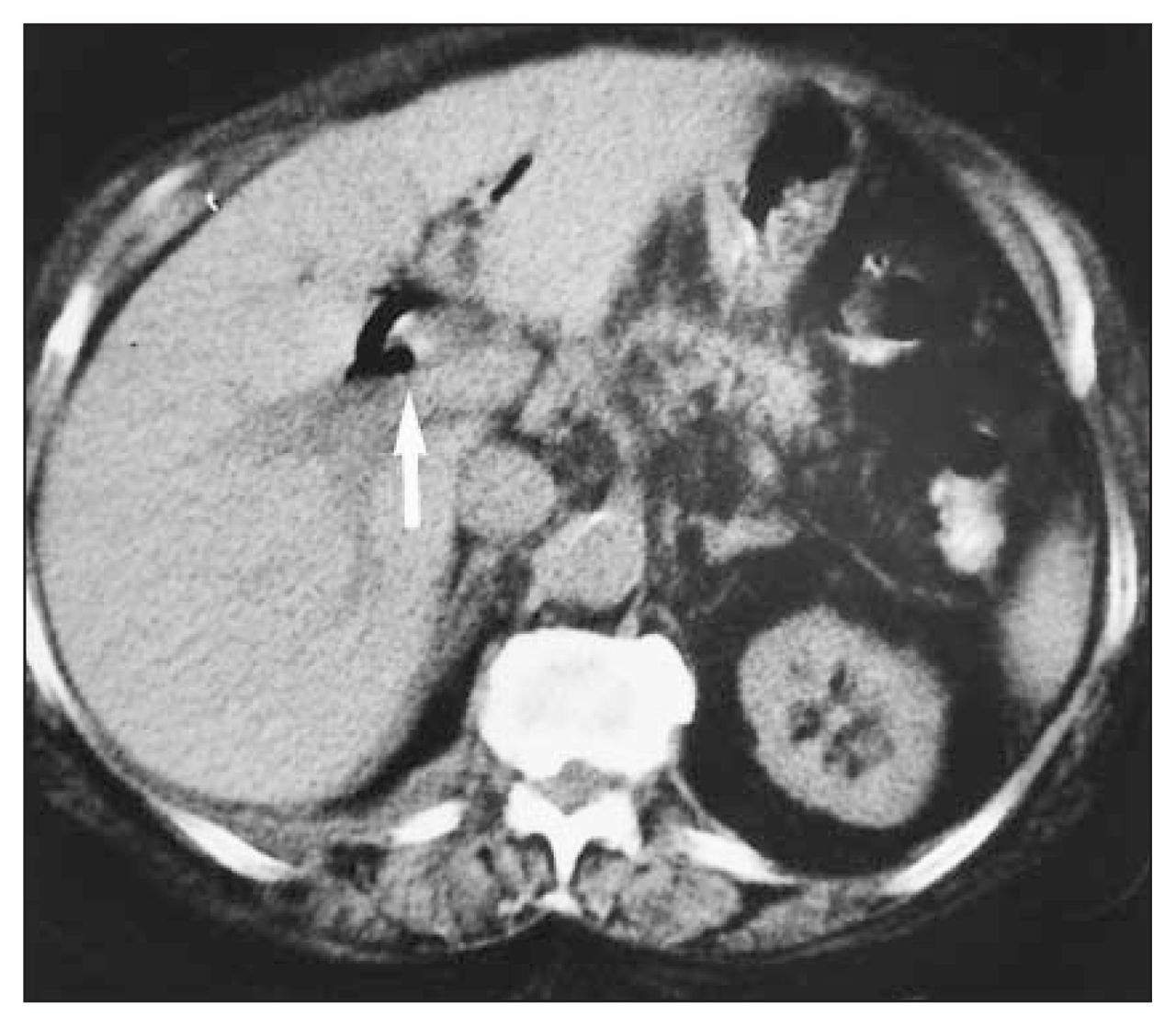
The preoperative computed tomography scan demonstrated a gallstone within the sigmoid colon (Fig. 2, arrows). The patient underwent a Hartmann resection, with subsequent confirmation of a gallstone, measuring 3.0 × 3.0 × 3.0 cm, impacted in a diverticular stricture of the sigmoid colon. One year earlier she had undergone computed tomography of the abdomen during an episode of acute diverticulitis. The scan showed a large gallstone within the gallbladder (Fig. 3, arrow). Air was also seen within the gallbladder and biliary tree. Subsequent endoscopic retrograde cholangiopancreatography demonstated persistence of a cholecystoduodenal fistula but no gallstones. Eight months later the gallstone resurfaced, presenting in the form of large-bowel obstruction.


Gallstone ileus accounts for 1%–3% of cases of mechanical intestinal obstruction. Gallstones gain access to the gastrointestinal tract most commonly by the formation of a fistula from the gallbladder to the duodenum, with fistulas to the colon and stomach being less frequent.1 The site of obstruction is most commonly the distal ileum (73%), with only 3%–8% of cases resulting in colonic obstruction.2 When colonic obstruction occurs, the blockage is usually at a stenotic site in the sigmoid colon. Impaction of the gallstone in the duodenum, resulting in gastric outlet obstruction (Bouveret’s syndrome3), in the jejunum and in the rectum have also been reported.1,2
The diagnosis of gallstone ileus is made in approximately 50% of patients at the time of presentation, more frequently when the classic triad of plain radiographic findings described by Rigler and colleagues4 are present. These include air in the biliary tree, mechanical bowel obstruction and an ectopic gallstone. With the use of additional diagnostic modalities the preoperative diagnosis increases to about 75%.2
The surgical management of gallstone ileus depends on the anatomic location of obstruction and findings at the time of surgery. For the majority of patients with gallstone ileus involving the terminal ileum, the options include a 1-stage procedure of enterolithotomy, a 1-stage procedure of enterolithotomy, cholecystectomy and repair of the fistula or a 2-stage procedure of enterolithotomy with interval cholecystectomy and repair of the fistula if it persists.5 Management of the present case was influenced by the presentation of large-bowel obstruction and the history of severe diverticular disease. A Hartmann resection of the sigmoid colon was done, with consideration being given to interval cholecystectomy.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.