


Abstract
Introduction: Three strategies are used to prevent complications in colorectal surgery: heparin and antibiotics given perioperatively and abdominal drains placed intraoperatively. To investigate the appropriate and inappropriate use of these prophylactic techniques and to assess the costs associated with their inappropriate use, we studied patients who underwent elective colorectal procedures.
Methods: We reviewed the charts of 103 patients operated on between April and December 1999 at a 519-bed tertiary care, teaching hospital in Edmonton, Alta. The procedures carried out were elective sigmoid resection, low anterior resection, left hemicolectomy, right hemicolectomy and total or subtotal colectomy for benign or malignant conditions. The data collected included patient age and sex, diagnosis, the operating surgeon, and the housestaff or surgeon writing the pre- and postoperative orders. Patients who required emergency colorectal surgery were excluded from the study. Antibiotic, heparin and drain prophylaxis was assessed and considered appropriate if prescribed according to the evidence or inappropriate if prescribed when not recommended.
Results: Thirty-six of 98 patients had inappropriate heparin prophylaxis (5 of the 103 were excluded because they were already receiving heparin). Only 5 of 96 patients were treated appropriately with antibiotics preoperatively without postoperative doses (7 of the 103 were excluded due to intraoperative spillage with fecal contamination or an intra-abdominal abscess found intraoperatively); 95% of patients were inappropriately treated with antibiotics postoperatively. Half of all the patients had a drain inserted inappropriately for prophylaxis. On average, drains inserted inappropriately cost $30.40 per patient, inappropriate antibiotic use cost $62.42 per patient and inappropriate heparin use cost $89.30 per patient. Preoperative orders were usually written by the staff surgeon, whereas postoperative orders were usually written by the resident or intern.
Conclusions: We observed considerable inappropriate use of heparin, antibiotic and drain prophylaxis. Considering the number of elective colorectal procedures performed annually, these inappropriately used strategies represent a substantial cost to the health care system. Improved education of surgeons and residents is needed to change to evidence-based practice habits.
Management of patients who undergo elective colorectal surgery includes the prevention and early detection of postoperative complications, according to 3 strategies: heparin given perioperatively, antibiotics given perioperatively and abdominal drains inserted intraoperatively for prophylaxis. These strategies have been well studied, and level I evidence is available to guide surgeons in their proper and effective use. Unfractionated heparin is recommended, 5000 U subcutaneously given 2 hours preoperatively, followed by heparin 5000 U subcutaneously 2 or 3 times daily postoperatively until the patient is ambulatory.1–3 In uncomplicated elective cases, antibiotics with activity against anaerobic and aerobic organisms are beneficial when given preoperatively only.4,5 For prophylactic drains, there is a lack of evidence supporting their use in uncomplicated elective colorectal surgery,6–8 and they may even be associated with perioperative complications.7
In this study we assess the correct versus the incorrect use of these 3 common prophylactic strategies, based on level I evidence in elective colorectal surgery patients at our institution, and the costs associated with their incorrect use.
Patients and methods
We reviewed the charts of 103 consecutive patients treated between April 1999 and December 1999 at a 519-bed tertiary care, teaching hospital in Edmonton. The operative procedures included elective sigmoid resection, low anterior resection, left hemicolectomy or right hemicolectomy, and total or subtotal colectomy. Patients who underwent emergency colorectal surgery were excluded. Data collection included age, sex, surgeon, diagnosis and the housestaff or surgeon writing the pre- and postoperative orders.
For assessment of the use of heparin perioperatively, additional data were collected regarding heparin usage preand postoperatively, including number of doses administered. In this study, the correct prophylactic use of heparin was defined as a preoperative 5000 U subcutaneous dose followed by 2 or 3 doses per day postoperatively. This was compared to the incorrect use of heparin, defined as no heparin or postoperative heparin administration without a preoperative dose.
Data collected for assessment of the perioperative use of antibiotics included use of preoperative bowel preparation, type of antibiotic used as well as number of doses preand postoperatively, intraoperative spillage of intraluminal contents and intra-abdominal abscess. Correct use of antibiotics was defined as the administration of antibiotics preoperatively without postoperative doses in clean-contaminated cases. This was compared with their incorrect use, defined as no antibiotics preoperatively or their use postoperatively in clean-contaminated cases.
Regarding the prophylactic use of drains, data were collected as to whether a drain was inserted, the presence of intra-abdominal abscess, postoperative complications, and drain-related complications. The prophylactic use of a drain was defined as incorrect when used in an uncomplicated case of colorectal surgery. Such drain usage was then compared to no drain use, which was considered correct.
Monetary costs for the use of heparin, antibiotics and drains were determined by the cost of each product to our institution and the cost to prepare, administer and manage the various treatment strategies. The cost of management was estimated by including the nursing time at an average hourly wage of $28.00.
The significance of differences in proportions was calculated with the χ2 test or Fisher’s exact test where appropriate. A p value of less than 0.05 indicated a significant difference.
Results
Patient demographics
The sex distribution was almost equal (Table 1), but the age range was wide (21–90 yr), with the majority of patients being between 50 and 70 years old. The diagnosis in 69% of the patients was cancer, which includes both carcinoma and adenoma. Thirty-five percent of the patients underwent right hemicolectomy, and 36% underwent sigmoid resection. Thirteen general surgeons were practising at the hospital during the study period.
Demographic Data for 103 Patients Who Underwent Elective Colorectal Surgery Between April and December 1999
Heparin prophylaxis
Five patients were excluded from the analysis of heparin prophylaxis because they were already on anticoagulation for pre-existing conditions. Of the remaining 98 patients, 36 were treated incorrectly (Table 2). Thirty-three patients received heparin postoperatively without a preoperative dose, and 3 patients received no heparin at all. The charts of patients who did not receive heparin were reviewed. Heparin had not been ordered for these patients, and no alternative prophylactic strategy had been used (i.e., no low molecular weight heparin or intermittent pneumatic compression stockings). All patients received heparin when ordered by the physician. There was no significant difference in the treatment given to men or women. When the various colorectal procedures and patient diagnoses were compared, we found no significant difference between the percentage of patients treated correctly and incorrectly. There were no cases of clinical deep vein thrombosis (DVT) or pulmonary embolism (PE).
Demographic Data for 98 Patients Who Received Heparin Prophylaxis Correctly or Incorrectly
The cost of heparin use in our institution was determined to be $4.70 per dose: heparin (5000 U subcutaneously) $0.70 per dose and nursing labour costs to prepare and administer the drug $4.00 per dose. The cost per patient was derived by multiplying the number of heparin doses the patient received by $4.70. The cost of incorrect heparin use ranged from $18.80–$470.00 per patient (mean $89.30 per patient). The use of heparin in a few patients was prolonged because postoperative complications preventing ambulation led to a long hospital stay.
Antibiotic prophylaxis
Seven cases were excluded from analysis of antibiotic prophylaxis because they had intraoperative spillage with fecal contamination due to inadequate bowel preparation or an intra-abdominal abscess was noted at the time of surgery. These patients were considered to be receiving antibiotics therapeutically rather than prophylactically. Of the remaining 96 patients, only 5 received antibiotics as prophylaxis correctly, according to the evidence, with a single preoperative administration and no subsequent doses postoperatively (Table 3). Thus, 91 patients received antibiotics incorrectly, and 2 of them received no antibiotics at all. Most patients received intravenous cefazolin and metronidazole for prophylaxis; however, 4 patients with allergies were given clindamycin and gentamicin. Antibiotics were given orally before operation to 57 of the patients; all of them had also received antibiotics systemically.
Demographic Data for 96 Patients Who Received Antibiotic Prophylaxis Correctly or Incorrectly
The cost of the antibiotics (cefazolin 1 g intravenously every 8 h and metronidazole 500 mg intravenously every 12 h) plus the intravenous tubing was determined to be $10.00/d. Nursing costs to prepare and administer the drugs was calculated as $16.33/d. Most patients received 1, 2 or 3 days of antibiotics postoperatively as prophylaxis. The average cost was $62.42 per patient.
Abdominal drains
Five patients were excluded from the analysis of drain insertion because an intra-abdominal abscess was found at the time of the surgical procedure, and a drain was placed therapeutically. Of the remaining 98 patients, 48 were managed correctly without unnecessary prophylactic insertion of drains (Table 4). Therefore, 50 patients who underwent elective colorectal surgery were drained incorrectly. Drain insertion did not appear to be sex-dependent. Significantly (p < 0.001) fewer patients having a right hemicolectomy had a drain placed, and significantly (p < 0.001) more patients with a sigmoid resection had a drain inserted. The only diagnosis that appeared to influence incorrect drain use was diverticulitis for which significantly (p = 0.031) more patients had a drain placed. There was 1 anastomotic leak in a patient with no drain present. Four complications occurred in patients who had drains inserted; in 3 of these, the anastomotic leak or abscess complication was noted after the drain had been removed. There were 2 drain-related complications: serous fluid leakage at the drain site after removal and abdominal wall hemorrhage during drain insertion, which required transfixion of the inferior epigastric artery.
Demographic Data for 98 Patients in Whom Drains Were Inserted Correctly or Incorrectly
The cost of a 7-mm Jackson-Pratt Silastic drain ($14.50) in addition to the nursing care to manage the drain estimated at $3.00/d translated into a cost range of $20.50–$59.50 per patient. The drains are reprimed every 8 hours and more frequently when required. The range in cost was due to the variability in the length of time before the drain was removed. The average cost was $30.40 per patient.
Practice patterns
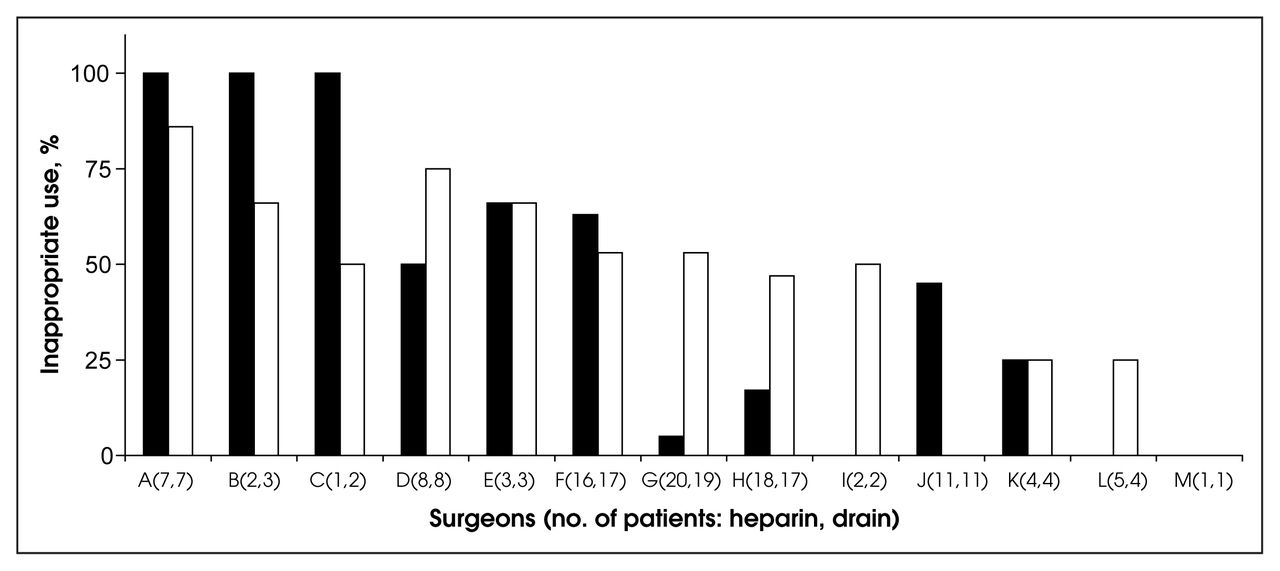
Fig. 1 shows the practice patterns of individual surgeons at our institution for heparin and abdominal drain use. There appears to be considerable variability among the surgeons. In contrast, incorrect antibiotic use was widespread. Preoperative orders were written by the staff surgeon, whereas postoperative orders were signed by the resident or intern in all but 2 cases.

The percentage of patients treated inappropriately by the 13 surgeons in the study. Bracketed numbers indicate the number of patients treated with heparin [black column) and having drains inserted (white column), respectively, for each surgeon. The discrepancy in patient numbers for some surgeons is due to the different exclusions applied for each strategy.
Discussion
The high risk of postoperative complications has led to various prophylactic strategies for elective colorectal surgery. Three commonly used interventions are DVT prevention with heparin, antibiotic prophylaxis to reduce postoperative infection and the prophylactic use of abdominal drains to detect anastomotic leak, hemorrhage or abscess.
PE and DVT are major causes of postoperative morbidity and mortality. 1 Prophylactic strategies for DVT have been well studied.1–3 DVT occurs because there is a triggering of the coagulation cascade at the time of tissue damage in addition to prolonged immobilization during the surgical procedures. In 1969, Flanc and associates9 noted that the rate of DVT, clinical and subclinical, postoperatively was 35%. In subsequent trials for DVT prophylaxis medication was initiated preoperatively and continued postoperatively. The 4th, 5th and 6th American College of Chest Physicians (ACCP) consensus conferences recommended the prophylactic use of heparin perioperatively for patients undergoing major abdominal surgery (which includes colorectal surgery), based on level I evidence.1–3 Heparin has been used for prophylaxis because it is non-toxic, has a limited duration of action, does not affect wound healing, does not interfere with conventional medications and is inexpensive. When heparin is contraindicated, intermittent pneumatic compression stockings can be used as an alternative. The recommended regimen with unfractionated heparin is 5000 U subcutaneously, initiated 2 hours preoperatively, followed by heparin 5000 U subcutaneously 2 or 3 times daily until the patient is ambulating. The use of low molecular weight heparin is also advocated but was not used by general surgeons at our institution during this study. The risk of DVT in patients who undergo colorectal surgery is up to 44% without prophylaxis3,10 but is reduced to 12.5% with the use of heparin.10 The risk of PE has been reduced from 1.6% to 0.54% with perioperative heparin prophylaxis.3,11
Stratton and colleagues12 examined the practices of preventing venous thromboembolism in high-risk patients and adherence to the 4th ACCP guidelines. They found that in general surgery 50% of patients received incorrect prophylaxis (this included 25% who received no prophylaxis at all). In comparison, general surgeons at our institution fared somewhat better, with 5% of patients receiving incorrect DVT prophylaxis.
Although most of our study patients did receive heparin postoperatively, the preoperative dose was not ordered in over one-third of these patients. Incorrect heparin use at our institution appears to be surgeon-dependent since the preoperative orders were written primarily by the staff surgeon. This may reflect a lack of knowledge of available evidence or concerns surrounding the risk of perioperative hemorrhage. However, studies demonstrated no increase in the rate of hemorrhagic complications due to preoperatively administered heparin.3 Postoperative heparin administration was primarily dependent on the resident or intern writing the orders. At our institution, housestaff are trained to order heparin postoperatively as standard for elective colorectal surgery. The question of whether there is adequate DVT prophylaxis with the administration of postoperative doses alone has never been studied. The well-recognized early evidence of DVT beginning at the time of surgery poses an ethical difficulty in allowing a randomized study without the preoperative use of heparin.
Wound infection is a common complication after colorectal surgery. Baum and associates13 reviewed clinical studies from 1965 to 1980. They found that infection rates were increased in patients who received bowel preparation alone compared with those who also received antibiotics. The perioperative use of antibiotics has reduced the infection rate from 40% to 11%–22%.4,5,14 Trials have been conducted with various parenteral antibiotic regimens, oral absorbable and nonabsorbable antibiotics, and topical antibiotics. Controversy remains regarding the most effective regimen; however, in a recent meta-analysis, Lewis15 concluded that a combination of antibiotics given orally and systemically may be superior for preventing surgical site infections. Systemically administered antibiotics were given preoperatively at our institution, with additional orally administered antibiotics given preoperatively to just over half of these patients. Most Canadian institutions have stopped using oral antibiotics preoperatively since neomycin in the oral form is no longer available. Antibiotics should be started 30–60 minutes preoperatively, so that the tissue concentrations are high at the time of bacterial contamination.16 Although there is no consensus as to the specific antibiotic of choice, it has been shown that coverage for both aerobic and anaerobic bacteria is required. 4 In our study, the most commonly used antibiotics for perioperative administration were cefazolin and metronidazole, but clindamycin and gentamicin were appropriately used in patients who had penicillin allergies. The need for antibiotics postoperatively in uncomplicated colorectal surgery cases was evaluated by Song and colleagues,5 who reviewed 17 randomized controlled trials between 1984 and 1995 and failed to show any benefit of multiple-dose prophylaxis over a single-dose prophylaxis.
Based on the evidence from our study, antibiotics are incorrectly ordered by almost all surgeons (or their housestaff) in our institution. Most patients received multiple doses of antibiotics postoperatively in addition to the preoperative doses, but 2 patients did not receive any prophylaxis. Postoperative orders were almost exclusively written by residents or interns. They likely prescribe antibiotics as prophylaxis because they have been misinformed or taught to do so. The discrepancy between evidence and practice by surgeons is further illustrated by Zmora and colleagues17 who conducted a survey of the members of the American Society of Colon and Rectal Surgeons in 2000 and found that most surgeons use 2 doses of intravenous prophylaxis in elective cases.
Abdominal drains are used to aid in the detection of bleeding, abscess and anastomotic dehiscence. Opponents believe drains stimulate serous fluid production, impede anastomostic healing and introduce infection. 7 Studies from 1987 to 1999 have failed to demonstrate a reduction in morbidity, length of stay or mortality from the prophylactic use of drains in nonemergent colorectal surgery.6–8 With respect to morbidity and mortality, a meta-analysis of 4 randomized control trials showed no significant difference for drain versus no drain insertion. 6 Sagar and colleagues18 noted that in 95% of cases, drains failed to allow the egress of pus or feces when dehiscence occurred. This lack of benefit remains when rectal or coloanal anastomoses are studied separate from colonic anastomoses.7,8 Merad and colleagues8 noted a 2% complication rate with drain use. In our study, half of all patients had drains inserted incorrectly, the majority for sigmoid resections for diverticular disease. Of note, 4 patients with drains had complications postoperatively, and 3 of these were complications noted after the drain was removed. In addition, we noted 2 possible complications with drain insertion: serous fluid leakage from drain site and inferior epigastric artery hemorrhage during insertion. The highly variable use of drains is surgeon-dependent. A drain may have been inserted as a precaution in patients with diverticular disease even though no active disease was present. These surgeons may not be aware of the evidence or they may resist change.
The cost of incorrect prophylactic strategies is important. On average, incorrect drain use cost $30.40 per patient, antibiotic use $62.42 per patient and heparin use $89.30 per patient. Thus, the direct costs for a single patient who received all 3 prophylactic strategies incorrectly is estimated at $200, which would translate into $15 000/yr for our institution. However, it is the hidden costs (complications associated with the incorrect prophylaxis, such as long-term drain-related complications, antibiotic resistance, Clostridium difficile colitis, progression of initial subclinical DVT or PE) that are underestimated in this study because of a lack of follow-up after patient discharge.
Although there has been considerable growth in evidence-based medicine (clinical practice guidelines, consensus conferences and the Cochrane database), this has been less prevalent in the surgical disciplines, probably owing to the lack of level I evidence and the difficulties associated with conducting randomized studies in surgical patients.19 Our study illustrates that even when strong evidence exists, surgeons are reluctant to adopt recommendations. It is possible that our own surgeons are poorly apprised of the facts, although given the academic environment with the constant stream of medical students and residents, this seems unlikely. More likely is the common observation that prior training and personal experience has a greater impact on surgical decision-making than published data, however strong the evidence.20 Further study evaluating surgeon practice and opinion after presenting the results of studies such as this one may help elucidate the barriers preventing evidence-based practice in surgery.
Footnotes
A portion of this work was presented at the annual meeting of the Canadian Association of General Surgeons in Edmonton, Alta., October 2000.
Competing interests: None declared.
- Accepted February 11, 2003.
References
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.