


Blunt thoracic aortic rupture (BTAR) is a life-threatening injury that is responsible for 15% to 23% of deaths from motor vehicle crashes.1 Most victims die at the scene from exsanguination, but 15% to 20% reach the hospital alive because the rupture is contained by the aortic adventitia and the surrounding mediastinal structures. 2 Up to 80% of patients with BTAR have concomitant injuries such as pulmonary contusion, neurologic trauma and intra-abdominal or pelvic hemorrhage.3 The accepted management of patients with BTAR comprises prompt diagnosis, evaluation and treatment of other life-threatening injuries followed by open aortic repair. Early open aortic repair in the presence of associated injuries increases operative mortality and morbidity. Death after open surgical repair of BTAR ranges from 7% to 28% with a 4% to 36% risk of paraplegia.4,5 Recently, placement of an endovascular stent-graft has been proposed as an alternative to open surgical repair for BTAR, and excellent early results have been reported.6,7 We describe our experience with 3 cases of BTAR managed with endovascular stent-grafts and discuss the indications and the management issues related to this procedure.
Cases reports
Case 1
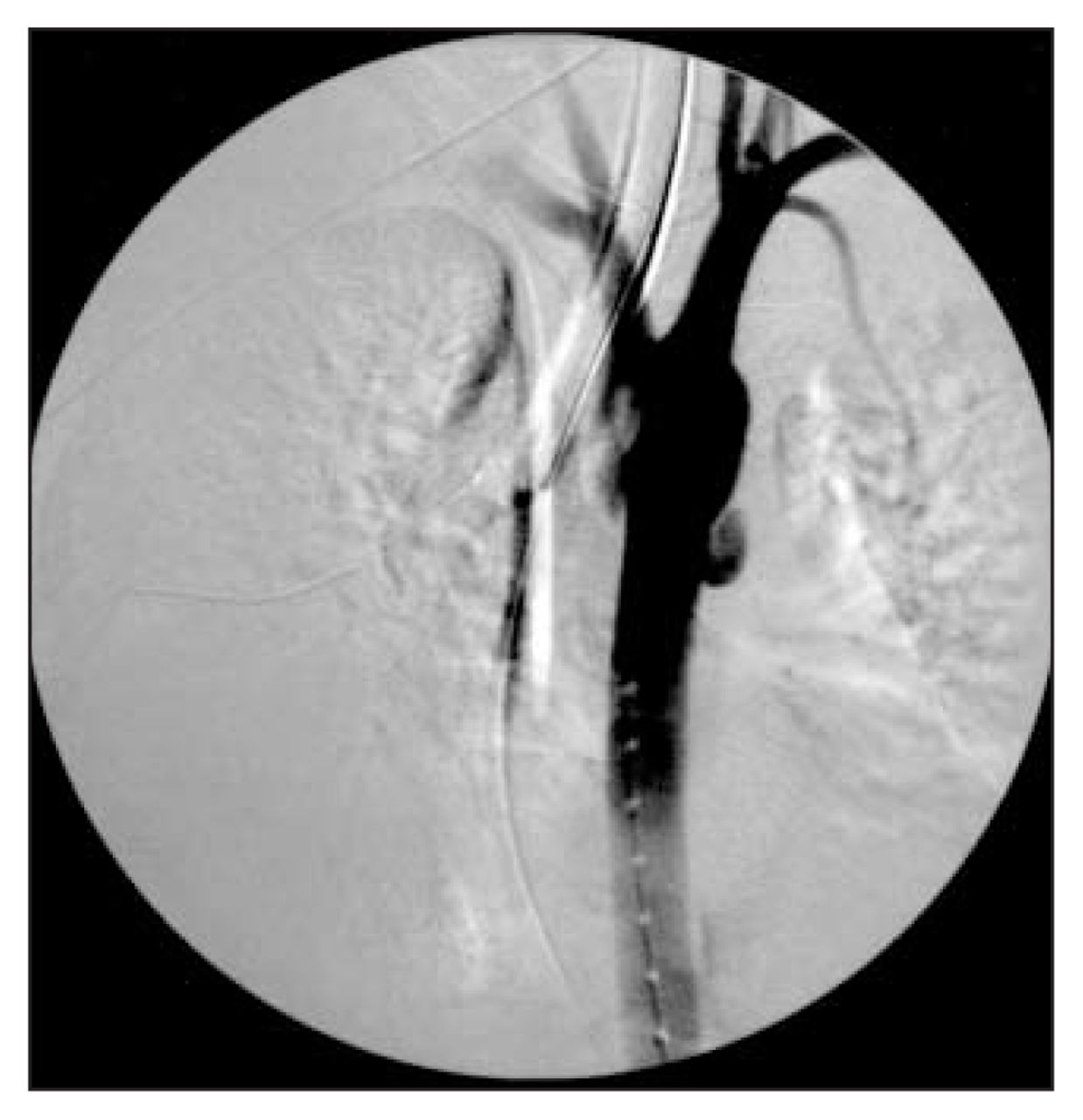
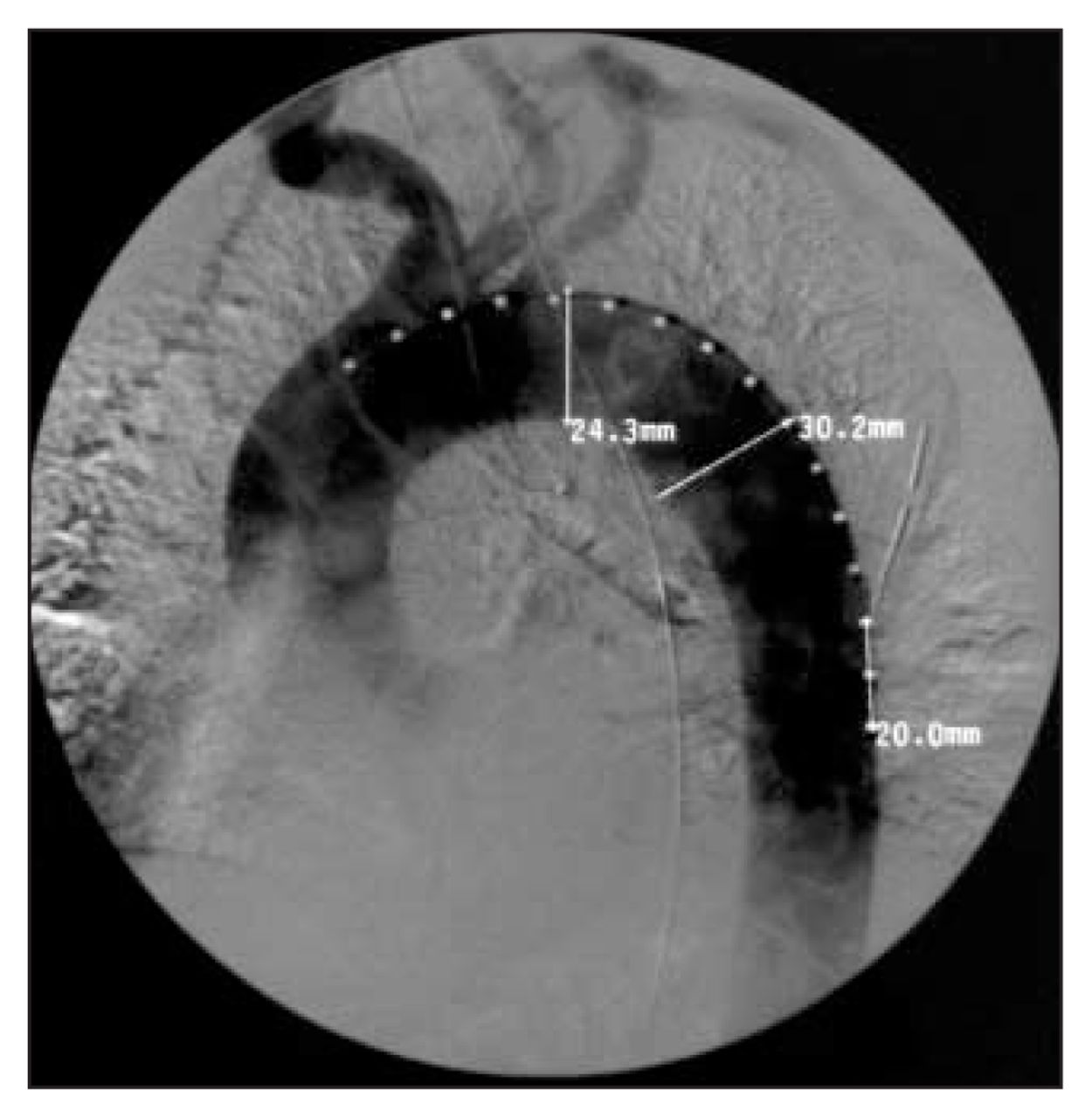
An 18-year-old woman involved in a motor vehicle crash was found at the crash site unconscious, hypotensive and tachycardic. Initial resuscitation measures included orotracheal intubation. In the Emergency Department, there was evidence of multisystem injuries. A diagnosis of hemoperitoneum necessitated a laparotomy. A splenectomy and a partial colectomy with a Hartmann procedure were performed, and chest tubes were inserted bilaterally for left and right pneumothoraces. Computed tomography demonstrated bilateral pulmonary contusions, multiple rib fractures, an unstable pelvic fracture and a possible aortic rupture at the level of the isthmus. After correction of her life-threatening injuries and multiple blood transfusions her vital signs stabilized. Aortography (Fig. 1) confirmed the aortic rupture, which was located 2.4 cm distal to the left subclavian artery. The aortic diameter measured 17 mm (inner diameter) at the level of the left subclavian artery.
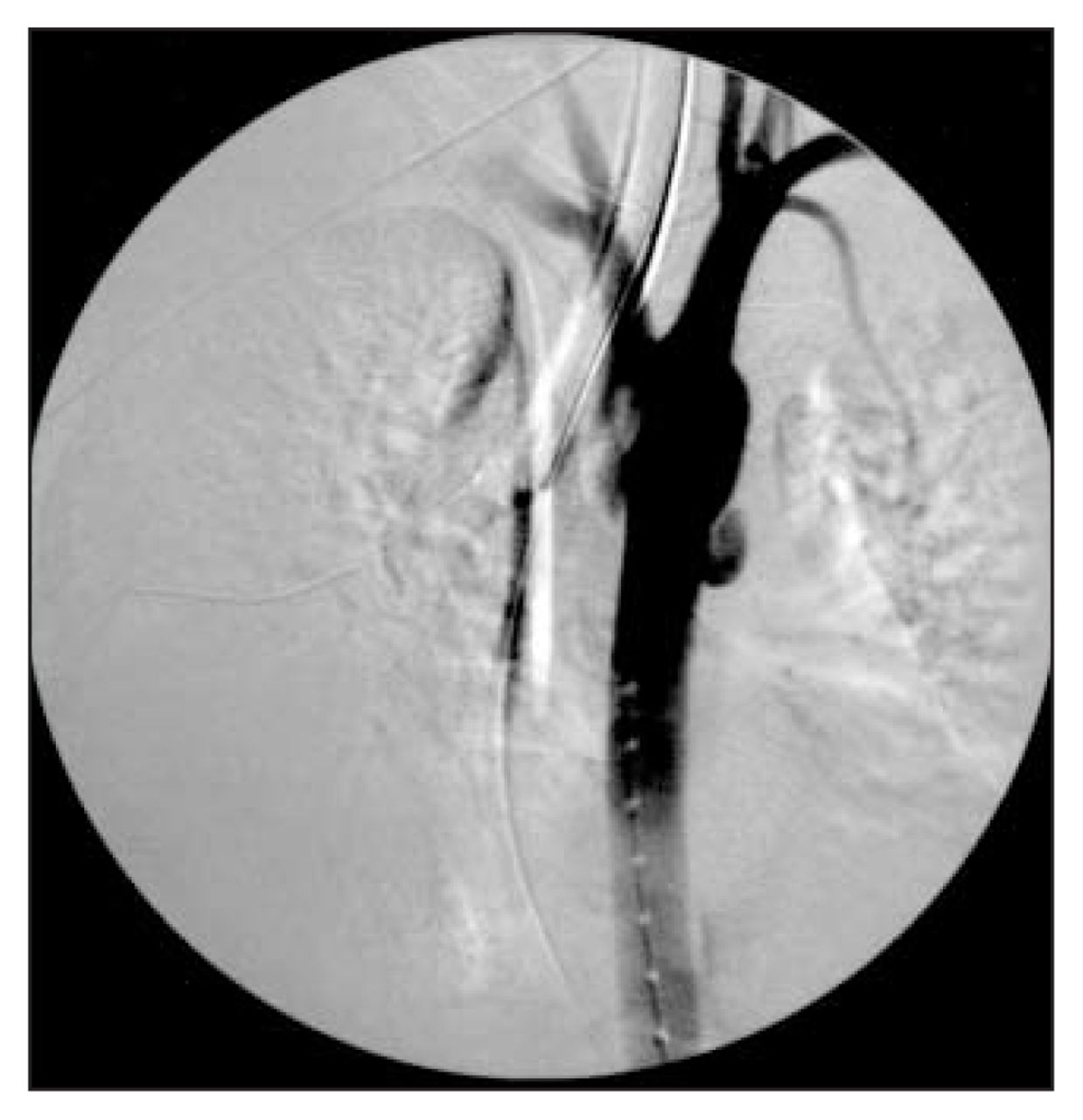
Case 1. Aortography demonstrating aortic rupture.
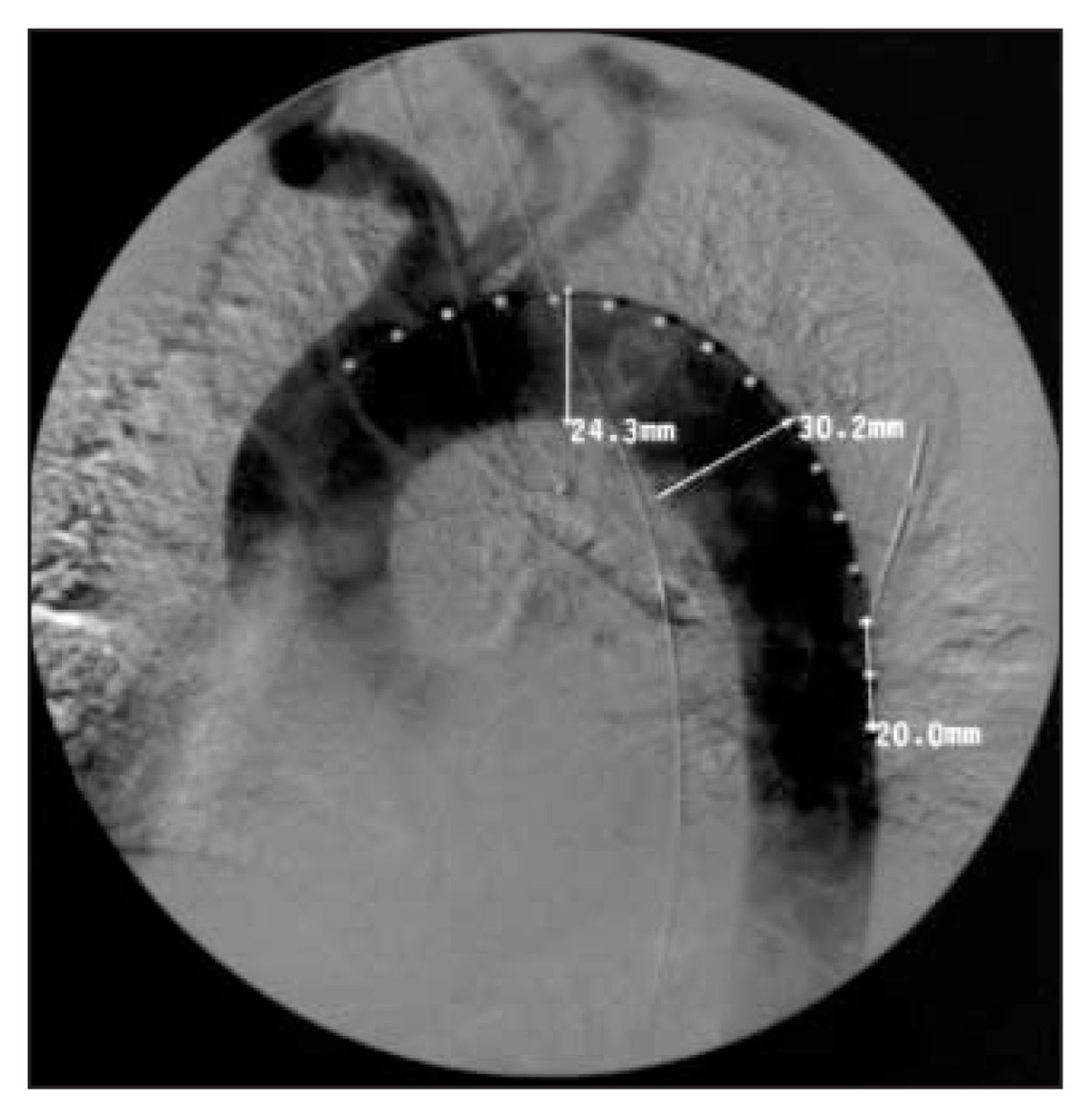
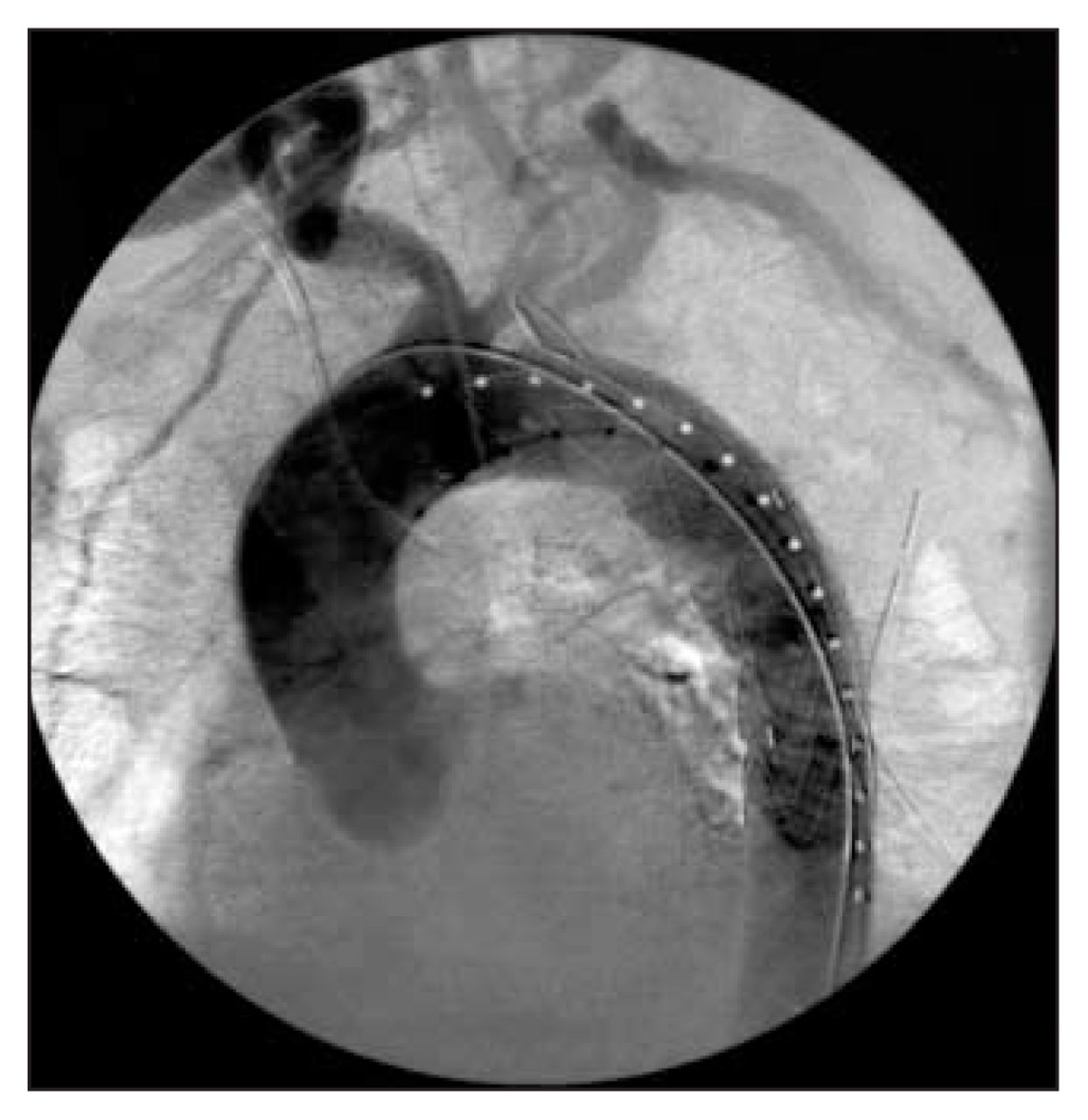
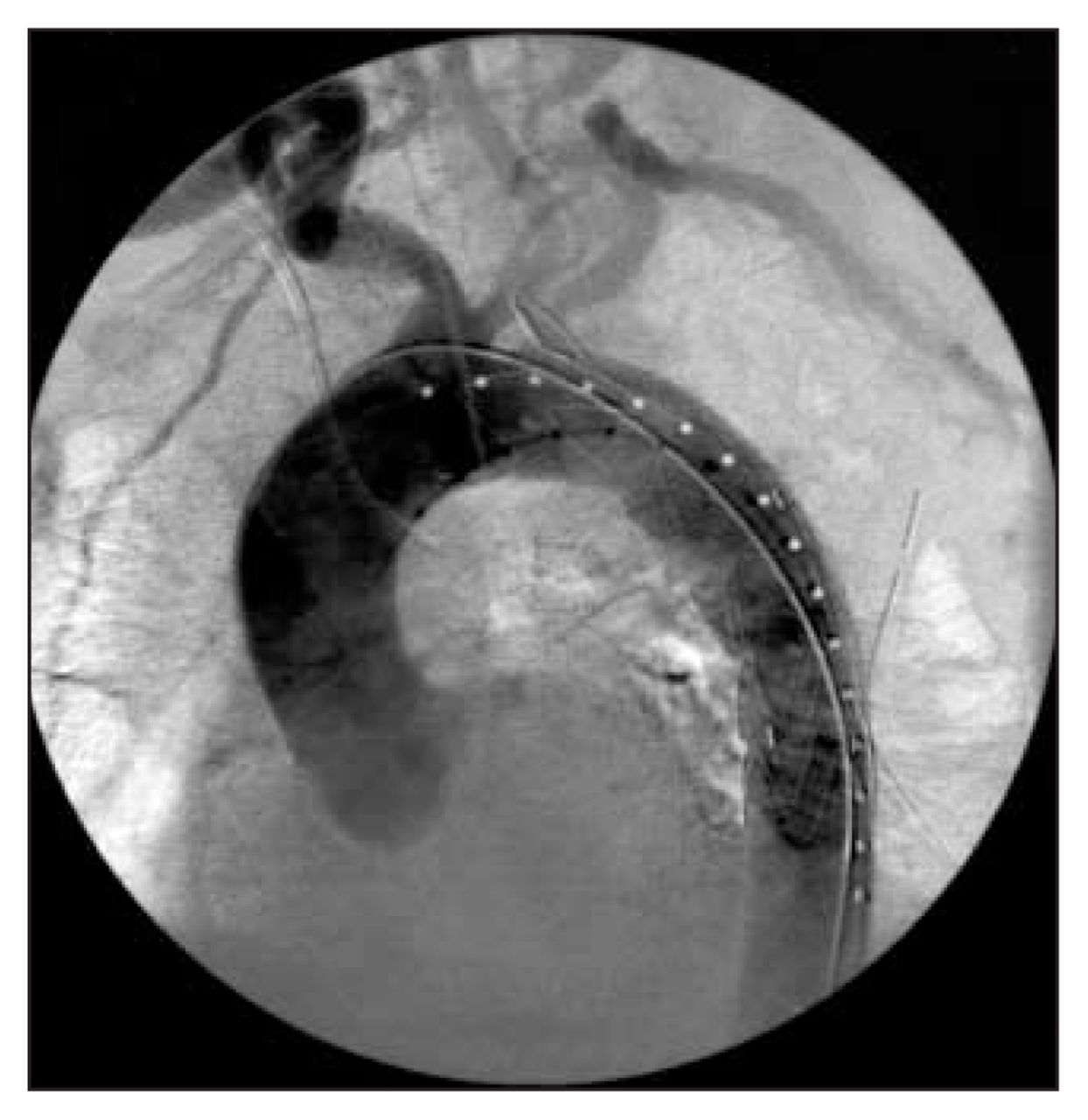
In view of her multiple injuries, open surgical repair of the aorta was deemed a high-risk procedure. An endoluminal approach was considered. However, the only rapidly available compatible stent was a graft extension (with proximal webbed flanges) measuring 24 mm proximally and 20 mm distally. Through a cut down in the right common femoral artery, the 80-mm Talent graft (Medtronic, Santa Rosa, Calif.) was deployed successfully. The proximal closed web stent-graft required coverage of the left subclavian artery to avoid a leak proximally, resulting in a left subclavian steal phenomenon (Fig. 2). Aortography performed after stent-graft placement showed no endoleak (Fig. 3).

Case 1. Delayed aortography phase showing the left subclavian steal owing to coverage of the subclavian artery by the webbed portion of the endoprosthesis.

Case 1. Post-procedural aortogram showing no endoleak.
The patient recovered and was discharged from the intensive care unit after 2 months. Three months after stent-graft insertion, chest CT showed no evidence of an endoleak or stent-graft migration. At the time of writing, the patient had no sign of vascular or neurologic deficit of the left arm.
Case 2
A 65-year-old man, involved in a motor vehicle crash, was seen at a community hospital. His medical history was relevant for high blood pressure treated with β-blocking agents and gastric surgery. He was alert and hypotensive (blood pressure 90/50 mm Hg) with a heart rate of 65 beats/min. A chest radiograph demonstrated severe left pulmonary contusion, multiple left hemithorax rib fractures and a widened mediastinum. He required orotracheal intubation for progressive respiratory distress. A left chest tube drained 300 mL of blood. Gross hematuria was noted. CT suggested an isthmic aortic rupture and a severe left renal contusion. The aortic rupture was confirmed by aortography (Fig. 4). Because of his multiple injuries an endoluminal approach was selected. Through a right femoral arteriotomy a 30-mm diameter proximal and distal open-webbed 100-mm long Talent stent-graft was placed (Fig. 5). After balloon dilatation, control aortography showed no endoleak. The patient was progressively weaned from the ventilator over the next 3 weeks. At 3-month follow- up, he had recovered fully without signs of stent-graft complication clinically or on CT.
Case 2. Aortogram demonstrating aortic rupture.
Case 2. Aortogram obtained after the procedure shows no endoleak.
Case 3
A 45-year-old man was involved in a head-on automobile collision. On arrival at a community hospital, he was unconscious with normal vital signs. An intracerebral frontal hematoma was demonstrated on CT and isthmic rupture of the aorta was considered highly likely. He was intubated and his blood pressure was controlled by medication, and he was transferred within 24 hours to our institution. An initial chest radiograph showed multiple rib fractures. Angiography confirmed the isthmic rupture (Fig. 6). Because of the intracerebral hematoma, an open repair was contraindicated. However, since the aorta measured 22 to 24 mm in diameter, no stent-grafts were readily available. A 28 to 28 mm × 100-mm long graft was shipped within 12 hours. In the meantime, the patient had complications with respect to oxygenation, hypotension and tachycardia. A chest radiograph showed a serious new hemothorax (1 L of frank blood was obtained). Concomitant with resuscitation measures, and because of impending aortic rupture, a 28 to 28 mm × 100-mm Talent endoprosthesis was placed to seal the ruptured aorta (Fig. 7). Follow-up CT 1 week and 3 months postoperatively revealed no endoleak. Patient recovered from his neurologic deficit over the next 5 months.

Case 3. Aortogram demonstrating aortic rupture.

Case 3. Aortogram obtained after the procedure shows no endoleak.
Discussion
The diagnosis of BTAR depends on acute awareness of the condition, mainly by identifying the presence of a major deceleration injury. BTAR may supervene at any level of the thoracic aorta. Patients with BTAR involving the ascending aorta usually die at the scene of the accident: 93% of patients reaching the hospital alive have a BTAR located at the level of the isthmus.8,9 The natural history of this condition was outlined more than 40 years ago by Parmley and colleagues,10 who reported that 86% of victims died at the scene of the accident or within 30 minutes of their arrival at the hospital. Of the surviving victims, 20% die within 6 hours, 30% within 24 hours and 75% within 8 days. Without treatment, only 2% survive, and they have a chronic pseudoaneurysm.
Because of its poor prognosis, BTAR has traditionally been managed with emergent surgical aortic repair. Recently, in light of appropriate pharmacologic treatment aimed at lowering systemic blood pressure, the natural history described by Parmley and colleagues has been challenged.11,12 By reducing stress on the aortic wall with short-acting β-blockers and with meticulous blood pressure control, Walker and Pate11 have proposed delayed open surgical aortic repair, especially in patients with concomitant injuries requiring lifesaving procedures such as laparotomy or embolization for pelvic artery bleeding. However, the time for safely delaying the aortic repair in the modern era of pharmacologic treatment remains unknown. Maggisano and colleagues3 have reported successful delayed treatment of BTAR in patients with severe concomitant injuries contraindicating immediate open aortic repair. On the other hand, other clinical studies indicate that in-hospital death remains an issue when treatment is delayed.1,13 Our third case illustrates the ongoing risk of rupture even with tight control of blood pressure. Fabian and associates,14 in a multicentre prospective study encompassing 274 patients with BTAR, reported a 9% rate of aortic rupture in patients who reached the hospital in a stable condition. Furthermore, 8% of patients were denied surgery for severe concomitant diseases. The overall death rate in the series was 31%. The operative mortality of patients sustaining BTAR is high, regardless of the surgical technique used; death is mainly linked to associated injuries or significant comorbidity.15,16 Furthermore, neurologic complications are significant, paraplegia being reported in up to 8% of patients who undergo open repair.17,18
Endovascular treatment for aortic disorders was initially proposed by Parodi and colleagues19 to treat abdominal aortic aneurysm. Subsequent utilization of stent-grafts for the thoracic aorta was proposed by Dake and associates.20 Recent reports have shown excellent early results of thoracic stent-grafts for the treatment of BTAR7,21,22 The 3 patients with BTAR whom we treated successfully with endoluminal stent-grafts had severe associated injuries, which we thought increased significantly the risks of open surgical repair. The advantages of an endoluminal treatment are its minimal invasiveness and its rapidity, thus decreasing the morbidity and mortality linked to associated injuries and comorbid conditions. Moreover, paraplegia after stent-graft implantation is exceedingly rare and is principally linked to extensive coverage of the thoracic aorta combined with an old or concomitant abdominal aortic procedure.23
Thoracic endograft procedures are preferably conducted under general anesthesia, and arterial and central venous pressure monitoring with an external pacemaker for backup. Insertion of a lumbar drain should be considered when a large portion of the descending aorta requires endografting especially in the presence of a previous or concomitant abdominal aortic procedure. Vascular access necessitates a calibre of artery allowing introduction of a 22 to 25 French delivery system. Access other than the common femoral artery may be required in up to 30% of cases, which increases the complexity and morbidity of the procedure. Emergent stent-grafting procedures require readily available “on the shelf” stents. Standard-sized stent-grafts are available in diameters ranging from 32 to 44 French. The need to ship the correct size from the manufacturer may delay the procedure by 24 to 48 hours. Custom-made stent-grafts may require up 6 to 8 weeks to obtain. Thus, with the present generation of stents, graft availability may be problematic, as encountered in our first and third patients in whom small aortic size contraindicated the use of standard, larger, readily available grafts. In our first case, the available graft was an extension graft with proximal webbed flanges necessitating coverage of the left subclavian artery to avoid a proximal leak. All currently available standard grafts compromise proximal and distal bare stents. Erosion of the bare stents is exceedingly rare but remains a long-term concern, especially in young people who are most of those who have BTAR. Furthermore, proximal and distal necks in most patients with BTAR are normal, so the need for bare stents to enhance fixation is questionable. To ensure precise graft deployment, especially in the vicinity of the left subclavian artery, adenosine-induced cardiac arrest is utilized. For isthmic ruptures within 2 cm of the left subclavian artery, partial or total coverage of the left subclavian artery should be considered. However, before that, the arch vessels require careful assessment by magnetic resonance imaging, angiography or noninvasive duplex scanning to exclude significant stenosis of the right common or internal carotid artery. Excluding an anomalous origin of the left vertebral artery from the aortic arch or a diseased right vertebral artery ensures an adequate posterior brain circulation. In such circumstances where the posterior cerebral circulation would be compromised, we recommend an extra-anatomic bypass to revascularize the left subclavian artery before stent-graft implantation. Otherwise, this artery may be covered with minimal risks of neurovascular compromise.24
Complications of stent-grafts may be divided into early and late. The rate of early procedural complications, such as aortic rupture and stroke, remains low with the more flexible shafts and with meticulous manipulation of the device in the vicinity of the aortic tear and the aortic arch. Early endoleaks should be rare when graft size is selected accurately. Proximal and distal “landing” sites com promise normal aorta. Stent-graft placement requires angiography with injection of contrast medium, which may result in an allergic reaction or renal failure. Use of contrast medium may be minimized by measuring graft size (aorta size + 15%–20%) on the enhanced chest CT. Mid- and long-term complications of thoracic endograft placement in patients with BTAR remain unknown. With a proximal and distal neck of normal aorta greater than 1.5 cm, the frequency of stent migration and late endoleaks, although reported with aneurysmal disease, should remain low. Stent fractures of thoracic endografts have been reported. However, erosion of graft material with late endoleak has not been reported to our knowledge. Such mid- and long-term complications necessitate a thorough, lifelong follow-up of patients treated with thoracic stent-grafts.
The place of stent-grafts in the management of patients sustaining BTAR remains unsettled. Young patients without comorbidity or significant associated injuries should be managed with open surgery using a distal perfusion technique such as a left heart bypass. Excellent operative results and long-term outcome have been reported in such patients.25 In patients with multiple blunt injuries with hemodynamic instability or injuries contraindicating an open repair, such as a severe pulmonary contusion or a severe central nervous system injury, a delayed open surgical approach or an endograft should be considered. In the presence of adequate vascular access, we favour a semiurgent endovascular approach to avoid early in-hospital rupture. The risk of this approach is difficult to quantify but is definitely present as illustrated in our third case. In addition, patients sustaining BTAR with serious comorbid conditions such as severe chronic obstructive pulmonary disease, severe heart or renal failure or shortened life expectancy (e.g., neoplasia) should be managed with stent-graft placement in the presence of adequate vascular access. Finally, special circumstances in conjunction with BTAR, such as associated contaminated thoracic wounds, major burns or established sepsis, require the use of a less invasive approach such as stent-graft insertion. Long-term follow-up of patients with BTAR treated with stent-grafts will allow us to better define the late outcome of this subgroup of patients. Only through a systematic follow-up will we be able to define the indications for stent-graft use in patients with BTAR. In the event of a favourable long-term outcome in patients with BTAR managed with stent-grafts, the endoluminal approach may prove to be the optimal treatment modality in such circumstances.
Footnotes
Competing interests: None declared.
- Accepted March 31, 2003.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.