


A 39-year-old man presented with a 5-year history of persistent left hip pain, which had been constant in nature over the last several months with increased severity after high activity and sitting for long periods. The pain was always present in the groin area, and would occasionally radiate to the knee. There was no history of hip disorders or other joint problems. The patient had no other significant problems or complaints.
On physical examination, the patient had a slightly antalgic gait, with no leg-length discrepancy. The range of motion for the left and right hips, respectively, were as follows: flexion 110° and 115°; abduction 40° and 40°; adduction 0° and 0°; internal rotation 0° and 10°; and external rotation 35° and 35°. The impingement test gave a positive result in the left hip (i.e., flexion, adduction and internal rotation reproducing knife-like pain in his groin). His motor power was normal, particularly about his hip girdle.
Plain x-ray films included an anteroposterior (AP) view of the left hip and a cross-table lateral view, with slight internal rotation of the left hip. On the AP view (Fig. 1), there were no signs of acetabular dysplasia or evidence of arthritis. On the lateral view (Fig. 2), the femoral head–neck offset was measured at 0.095 (approximate normal measurement should be > 0.191). Magnetic resonance imaging (MRI) arthrography with gadolinium enhancement revealed an acetabular labral tear with associated cartilage delamination (Fig. 3). The technique for MRI was as follows. Through an anterior approach, and with sterile technique and fluoroscopic guidance to localize the femoral neck, 3 mL of nonionic iodinated contrast material was injected to confirm intra-articular needle position. This was followed by instillation of 10 to 20 mL of gadolinium saline at a dilution of 1:100. The MRI was performed on the Siemens (Ehlangen Germany) 1.5 T Symphony MRI scanner. Axial, coronal and sagittal fat saturated images were obtained using the spine and body array coils; TR (repeat time) = 630 ms, TE (echo time) = 12 ms; 256 × 256 matrix for axial and sagittal images, 512 × 512 matrix for the coronal image; 3-mm slice thickness using 200 mm field of view.

Anteroposterior radiograph of the left hip shows no significant dysplasia or arthritis.

Cross-table lateral view of the same hip illustrates the lack of femoral head–neck offset.
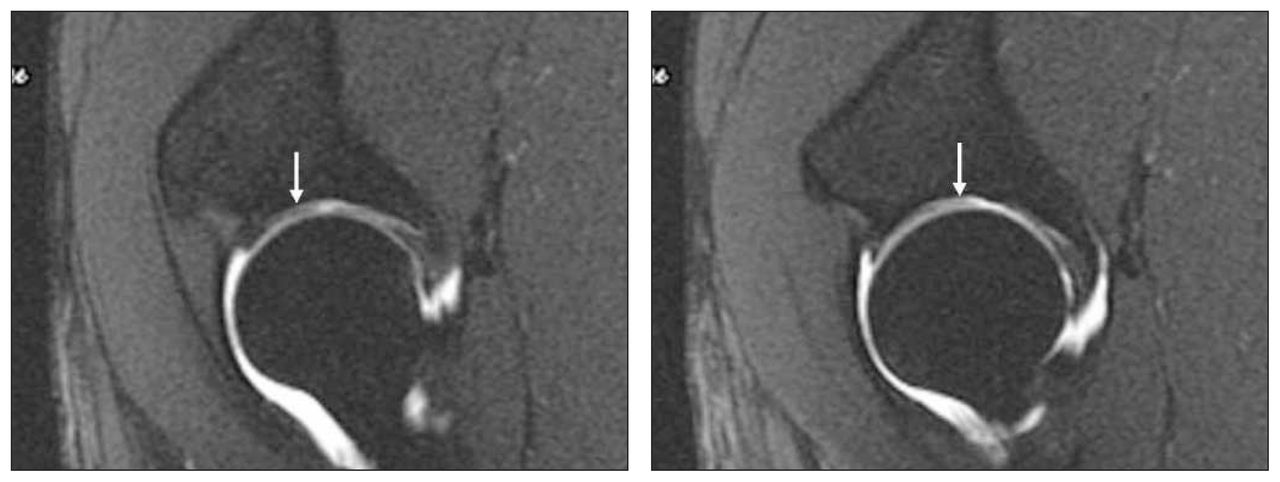
Sequential sagittal magnetic resonance images demonstrate cartilage delamination. The cartilage flap appears as a linear intra-articular filling defect of low signal intensity (arrows) surrounded by contrast that results in the appearance of an inverted “Oreo” cookie.
After nonoperative measures failed, the patient elected to undergo surgery. The surgical procedure consisted of a surgical dislocation of the left hip2 with débridement of the cartilage lesion and femoral chondroosteoplasty to improve the femoral head–neck offset. The patient was doing well 2 years after the procedure.
There is a relationship between the anatomy of the hip joint and the development of degenerative joint disease.1,3 Femoroacetabular impingement can result either from an overcoverage of the acetabulum4 (i.e., retroversion) or from a lack of offset between the femoral head and neck in the anterior and anterolateral areas.5 This offset refers to the difference between the maximal anterior radius of the head and the anterior radius of the adjacent femoral neck. The repeated contact of the femoral head–neck junction within the acetabulum leads to shearing of the labrum and the adjacent acetabular cartilage from the underlying subchondral bone (i.e., delamination).6 The location of the damage is rather constantly seen in the anterior superior rim area of the acetabulum where the femoral neck abuts the rim. The repeated insult is thought to lead to degenerative arthritis of the hip joint. In these situations, joint-preserving procedures such as surgical dislocation with chondroosteoplasty for femoroacetabular impingement can provide pain relief and improve function. As demonstrated here, MRI with gadolinium arthrography can be a useful adjunct in confirming the pathologic disorder by showing cartilage delamination at the site of impingement. In doing so, this may permit earlier intervention to prevent further degeneration of the acetabular cartilage. This cartilage delamination has the characteristic appearance of an inverted “Oreo” cookie.
Footnotes
Submissions to Surgical Images, musculoskeletal section, should be sent to the section editor Dr. Edward J. Harvey, McGill University Health Centre, Montreal General Hospital, 1650 Cedar Ave., Montréal QC H3G 1A4; edward.harvey{at}muhc.mcgill.ca
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.