


1. FLEXION–DISTRACTION INJURIES OF THE THORACOLUMBAR SPINE: HEALTH-RELATED QUALITY OF LIFE (HRQoL) AND RADIOGRAPHIC OUTCOMES
Purpose:
To determine the long-term HRQoL in patients treated for thoracolumbar flexion–distraction injuries.
Significance:
Previous studies of flexion–distraction injuries are retrospective reviews of small inhomogeneous cohorts with considerable variability in their reported outcomes. There is little, if any, focus on outcome measures relating to the patients’ HRQoL. This study represents the largest series of well-defined flexion–distraction injuries with outcomes measured using validated, standardized instruments of HRQoL.
Method:
Seventy-four patients were treated either operatively or nonoperatively at a tertiary care referral centre between 1995 and 2000. A retrospective chart review was done to obtain baseline variables. Injury classification, healing and alignment were determined by radiographic analysis. Cross-sectional outcome analysis using the NASS and SF-36 was done. Regression modeling assessed baseline variables. Limitations were characteristic of retrospective reviews; however, the study is strengthened by a homogenous cohort and cross-sectional validated outcomes.
Summary of results:
Seventy-four patients met eligibility criterion, with 50 completing questionnaires. 55.4% were treated surgically and 44.6% conservatively. Average follow-up was 3.3 years. The average NASS Pain and SF-36 Physical Health scores were 77.3 and 61.0 among the surgical group, and 74.9 and 63.5 among the nonsurgical group, respectively. The average SF-36 Mental Health scores were 70.9 for the surgical group and 73.2 for the nonsurgical group. The most common mechanism of injury was a motor vehicle accident (72.7%) and the use of seatbelts in this group was 86.5%. Forty-one patients had associated injuries, with blunt abdominal trauma representing 51.2% of these.
Conclusion:
The outcome of these patients treated either surgically or conservatively is favourable when treatment is based on patient factors, stability and neurology. Secondary factors such as mechanism of injury, associated injuries and third-party coverage should be evaluated but do not significantly influence patient outcomes.
2. PREOPERATIVE PREDICTIVE FACTORS IN LUMBAR DISCECTOMY
Consecutive patients undergoing hemilaminectomy and discectomy by a single surgeon for radicular symptoms due to lumbar disc herniation were enrolled. The change in Roland Morris Questionaire (RMQ) scores 2 years postoperatively was used as the outcome measure to evaluate the effect of surgery.
Preoperative and 2-year follow-up RMQ scores were available for 91% (51/56) of the patients enrolled. Seventy-six per cent noted significant improvement (> 4 change in RMQ score). All patients had measurement of the area of both halves of the thecal sac and nerve roots (symptomatic and asymptomatic sides) at the disc level involved. Results of the relationship between the amount of radiologic neural impingement (ratio of the area of the symptomatic to the asymptomatic side), duration of symptoms, focal neurologic deficit, straight leg raising, and WCB claims to the change in RMQ scores will be presented.
3. RESULTS OF POSTEROLATERAL FUSION VERSUS COMBINED POSTEROLATERAL AND INTERBODY FUSION IN THE LUMBAR SPINE: PRELIMINARY RESULTS
This retrospective study of 50 patients from a prospective databank analyzes the results of decompression, pedicle screw rod fixation and posterolateral fusion with and without interbody fusion. The objective was to evaluate the outcome of these 2 methods for one-level degenerative disorders of the lumbar spine.
The concept of anterior column support has gained increased popularity, particularly to theoretically increase fusion rate and prevent deformity. Fifty patients were divided into 2 equal groups and treated with either posterolateral fusion alone or instrumented posterolateral and interbody fusion. These 2 groups were compared for a clinical outcome, fusion rate and subsequent development of deformity.
In this preliminary study, the fusion rate seems similar in both groups. Subjective outcome was slightly improved, but not statistically significantly, in the interbody fusion group. Deformity correction was much improved in the interbody fusion group, as was maintenance of correction. In conclusion, this preliminary study of 50 patients indicates that there are slight advantages to interbody fusion, but longer term analysis will be required.
4. POSTEROLATERAL INTERBODY FUSION USING A UNIQUE OSTEOCONDUCTIVE IMPLANT, SUPPLEMENTED WITH POSTERIOR PEDICLE-SCREW INSTRUMENTATION AND UNILATERAL INTERTRANSVERSE FUSION USING LOCAL GRAFT. EARLY RESULTS
Purpose:
To report the early morphological results of a technique for posterolateral interbody fusion (PLIF) without iliac graft harvest.
Methods:
Independent chart and imaging review was undertaken after 50 cases had been done. In 47 cases there was complete documentation available, and of those, 22 qualified for this preliminary report at a minimum of 12 months’ follow-up.
Results:
Subjects included 7 males of mean age 66 years (range 45–84 yr) and 15 females of mean age 54 years (range 34–78 yr). Review was at a mean of 16 months. Thirty motion segments were stabilized and 57 implants inserted. Blood loss averaged 1.6 L/case or 1.1 L/level. Sentinel sign of trabeculated bone bridging the disc space was seen in 20 instrumented motion segments (67%). There were no infections, dural tears, loss of fixation or evidence of nonunion in the series. Intertransverse consolidation of bone was completely consistent.
Conclusions:
This protocol for 270° arthrodesis in lumbar reconstruction allows for consistent stabilization of the spine without iliac bone grafting, eliminating donor site morbidity. The Prospace™ device is sufficiently osteoconductive to facilitate interbody consolidation in approximately 67% of cases.
Discussion:
The PLIF operation is recognized as a difficult and often very bloody procedure that offers the advantage of anterior-column stabilization without an anterior approach. The Prospace™ implant is promoted as sufficiently osteoconductive to facilitate interbody arthrodesis without bone grafting. The combination of a large volume of morcellized local graft material harvested from the wide decompression required for PLIF and the mass effect of that volume being concentrated in one intertransverse gutter is also unique. Together with the stability afforded by interbody spacers combined with pedicle-screw instrumentation, an optimal environment for arthrodesis may be created. Early results of this series suggest the technique is successful.
Significance:
Patients qualifying for PLIF reconstruction can be stabilized without a requirement for iliac harvest.
5. THE MORPHOLOGY OF THE L4–L5 AND L5–S1 DISCS IN ASYMPTOMATIC AND SYMPTOMATIC SPINES: MRI STUDY OF NORMAL AND DEGENERATED DISCS IN THE SITTING AND KNEELING POSITIONS WITH OR WITHOUT THE ADDITION OF 40-LB WEIGHTS
The objective of this study was to first compare the morphology of the L4–L5 and L5–S1 normal discs in asymptomatic spines in different positions (supine, sitting and kneeling) and with the addition of a 40-lb weight under MRI. We then studied the morphology of asymptomatic L4–L5 and L5–S1 pathologic discs (moderate to severe degeneration with or without disc fissures or herniation observed on a prestudy 1.5 tesla MRI) in the same positions and with the addition of weight. These results were then compared to those obtained with symptomatic spines, in the different positions and with the addition of weight.
Symptomatic spines have significantly thinner pathologic discs than asymptomatic pathologic spines. However, in our groups, aged from 30–60, the incidence of disc pathology was similar in both the symptomatic and asymptomatic spines (70% v. 76%). Pathology was not worse in the symptomatic spines. Studies in the sitting and kneeling positions showed new pathology in 6 symptomatic patients. A 40-lb weight addition to the spine did not modify the disc in all groups.
6. CAPACITY OF A SINGLE-UNIT PROSTHETIC DISC NUCLEUS TO RESTORE BIOMECHANICAL BEHAVIOUR IN A SIMULATED PROLAPSED INTERVERTEBRAL DISC
Introduction:
The biomechanical behaviour of a new singleunit hydrogel-based prosthetic disc nucleus was evaluated in a cadaveric model and compared with that of the paired-unit design currently in use. When hydrated, the single-unit device has 40%–50% less gel volume but only 15% less contact area with the end-plates than the paired-unit design.
Methods:
Intact, fresh-frozen human lumbar motion segments were sequentially tested in compression (700 N), flexion, extension, and right and left lateral bending (21 Nm) in each of 4 conditions: intact, after removal of the nucleus, after implantation of the prosthetic nucleus devices, and after 72 hours of device hydration in saline. Stiffness values were obtained from the loaddisplacement curves using a repeated-measures general linear model (GLM) and compared using Bonferroni’s post-hoc tests.
Results:
Motion segment stiffness in compression decreased significantly following nucleus removal and increaseed significantly following implantation and hydration of both the singleunit and paired-unit designs when compared with the denucleated condition (p < 0.05). The difference in the hydrated state between the 2 designs was not significant. Behaviour of the motion segments in bending was too variable to reveal statistical differences.
Conclusions:
The single-unit design requires no greater surgical access than the paired-unit design and offers the potential for reduced surgical time due to the reduced complexity of implantation. Results of this study indicate that the single-unit design is capable of restoring the intact behaviour of the motion segment in compression and is no different than the paired-unit design in this regard.
7. ARTIFICIAL DISC REPLACEMENT: THE CANADIAN EXPERIENCE
The first lumbar artificial disc replacement surgery was done at the London Health Sciences Centre in London, Ont., in April 2000. Seventeen patients have been operated on with an 80% 1-year or better follow-up.
An examination of the literature reveals a gap of information available about Canadian patients. The purpose of this clinical review is to derive population-specific information available to health care professionals about artificial disc replacement surgery for degenerative disc disease. This study will compare pre- and postoperative patient symptoms, physical examination findings, radiographic data and quality-of-life indices. Operative findings and complications will be reported to gain insight into technical factors and operative considerations related to the Charité III Disc Replacement in the lumbar region. Finally, data will be used to plan a system-based approach for orthopedic care of this patient population using health promotion theory.
8. CRYOTHERAPY OF THE FACET JOINTS IN THE TREATMENT OF THE FACET SYNDROME. TREATING AT −150°C INSTEAD OF −80°
Cryotherapy has been used in the treatment of the facet joint syndrome since the 1960s. The temperature of the probes was −80°C. Patients were better for a few months (< 1 yr). Zhou and colleagues have shown that temperatures of −30°C to −100°C cause no permanent damage. Irreversible nerve damage is observed with temperatures below −140°C. Gallil probes used under MRI vision permit treatment temperatures of −150°C to −180°C. Forty-eight patients ages 26–74 years were treated with facet cryotherapy once blocs confirmed the diagnosis. The average follow-up was 11.4 months. Seventeen patients had a pur facet syndrome without other pathology. Eighty-eight percent of these had a pain relief of 72.6% at 12.1 months. These results compare favourably with other percutaneous or open techniques.
9. A PRIORITY SCORING SYSTEM TO ASSIGN URGENCY TO REFERRALS IN A SCIENTIFIC AND TIME EFFICIENT MANNER
The demand for specialist spinal assessment in Alberta exceeds what can currently be offered. This has resulted in extensive waiting periods. In an attempt to make the referral process more efficient, a referral scoring system was developed by the University of Calgary Spine Program.
The scoring system evaluates 3 specific areas of information. This consists of clinical patient information, radiologic results and disease type. Depending on the severity and urgency in each of these areas, a priority score is calculated. The priority score is used as a tool to guide the urgency of a referral.
To validate the scoring system, inter-observer and intra-observer reliability were evaluated by comparing priority scores of 100 patients scored in a blinded fashion by medical and nonmedical personnel.
The results of the initial and subsequent scoring revealed this tool to be useful and reliable in appropriately prioritizing referrals. The application of the form to an electronic online service may further increase the efficiency of the referral process.
10. TYPE II ERROR IN THE SPINE SURGICAL LITERATURE
Purpose:
To determine the frequency of potential type II error in randomized controlled trails reported in the spine surgical literature.
Method:
A literature search was conducted of the MEDLINE, PubMed and the Cochrane databases using the key words “spine” and “surgery,” between 1967 until the present to identify randomized controlled trials involving spine surgery. Trials were included in this study if they were of a 2-group design, with at least 1 of the groups being a surgical cohort, and that reported a nonsignificant difference in the primary outcome. We determined the frequency for which the primary outcome and sample size calculation was reported. The sample size was assessed to determine whether the trial had sufficient subjects to detect a 25% and 50% relative difference in the primary outcome for a power of 80%.
Summary of results:
Twenty-nine studies satisfied the inclusion criteria. Nine studies specifically identified a primary outcome. All others reported multiple outcomes with no specified primary measure. Four studies reported a sample size calculation. Of the remaining 25 that did not, 3 had sufficient power and the rest were at significant risk of committing a type II error.
Conclusion:
The spine surgical literature is plagued with a high potential for type II errors in published trials with a nonsignificant outcome.
Significance:
In the spine surgical literature, a randomized controlled trial that fails to reject its null hypothesis requires careful scrutiny of its methodology to prevent misinterpretation of the results.
11. ANTERIOR TRANSARTICULAR C1–C2 FIXATION: A BIOMECHANICAL STUDY
Purpose:
To describe a new technique for anterior transarticular screw fixation of the atlantoaxial joints, and to compare the stability of this construct to posterior transarticular screw fixation with and without laminar cerclage wiring.
Methods:
Nine human cadaveric specimens were used. The C1–C2 motion segment was instrumented using either anterior transarticular screws (group 1) or posterior transarticular screws alone (group 2) or posterior screws with interlaminar cerclage wires (group 3). The specimens were then tested in translation, rotation, lateral bending and flexion-extension. A 50 N axial load was used to simulate the weight of the head. Translation forces were 100 N, whereas 2 Nm of torque was used for flexion-extension, rotation and side bending.
Results:
All values for the 3 groups with regards to anterior/posterior displacement, rotation and lateral bending were statistically similar using ANOVA testing. The only significant difference was registered in flexion-extension testing, where mean values of 5.4° of movement were registered in group 1, 6.8° in group 2, and 1.7° in group 3.
Conclusion:
Anterior C1–C2 fixation using transarticular screws is as stable as posterior transarticular fixation in all clinically significant planes of motion. The addition of posterior interlaminar wiring only improves resistance to flexion-extension forces.
Discussion:
Anterior transarticular screw fixation of the atlantoaxial spine has several advantages over posterior fixation techniques, including supine patient positioning, a less extensive surgical approach and the ability to perform this procedure in the presence of severe thoracic kyphosis. In the absence of biomechanical and technical disadvantages, this should become the method of choice for C1–C2 stabilization.
12. ACCURACY AND SAFETY OF PEDICLE SCREW FIXATION IN THORACIC SPINE FRACTURES
Study design:
A prospective cohort outcome evaluation of unstable thoracic spine fractures treated with posterior pedicle screw fixation.
Objective:
This study was done to determine the accuracy of placement, safety of pedicle screws in open reduction of unstable thoracic spine fracture.
Methods:
Surgery was performed by 1 of 5 fellowship-trained spine surgeons. CT scans were performed on 23 patients using 3-mm cuts in sagittal and transverse planes. Pedicle screw position was assessed by 3 independent reviewers. Screw position was categorized as within or in violation of the pedicle wall. Further subclassification of wall violation reviewed the direction and distance of perforation. Independent perioperative and postoperative surveillance for complications was done.
Results:
Twenty-three unstable thoracic spine fractures treated with 200 posterior pedicle screws were analyzed. The pedicle screws spanned from T1–T12 with the majority of screws in the mid-thoracic region. Of the 200 thoracic pedicle screws placed, 70% were fully contained within the pedicle wall. The remaining screws were deemed “out” with cortical perforation (30%). Of these, 20% were lateral perforations, 5% were medial perforations and 5% were anterolateral perforations. No superior, inferior or anteromedial perforations were found. There was no regional area variation in incidence of perforations. Ten percent of all perforations were directly related to pedicle diameter to screw diameter mismatch. There were no adverse neurologic, vascular or visceral injuries detected intraoperatively or postoperatively.
Conclusions:
Nintey-eight per cent of screws had satisfactory accuracy. Although very minor misplacement of pedicle screws occurred, there were no complications and we recommend the use of pedicle screws in thoracic fractures.
13. A COMPARISON OF PERCUTANEOUS ENDOSCOPIC THORACIC DISCECTOMY VERSUS THORACOTOMY FOR THE TREATMENT OF THORACIC DISC HERNIATION
Introduction:
Symptomatic herniated thoracic discs are an uncommon but important cause of thoracic back or radicular pain or myelopathy. Although many cases will respond to nonoperative treatment, progressive neurologic deficit or long standing incapacitating pain are indications for surgical intervention. Excision of a herniated disc can be accomplished utilizing anterior, posterior or lateral approaches. The transthoracic approach is the most common anterior approach. Video-assisted minimally invasive techniques are variations of the transthoracic approach and have gained recent popularity as a treatment option for selected thoracic disc herniations. The purpose of this study was to compare the open transthoracic approach to a percutaneous endoscopic approach for excision of herniated thoracic discs. Specific attention was paid to hospital stay, operating time, blood loss, narcotic use and complications.
Methods:
Retrospective observational study. In a thorough chart review, 23 patients were identified as having recently undergone an anterior approach for a herniated thoracic disc. Eighteen of these patients presented with myelopathy. There were 10 thoracotomy procedures and 14 endoscopic procedures identified.
Results:
Both groups were similar with respect to demographic data. There was a significantly shorter hospital stay and less narcotic use with the endoscopic group. There were no significant differences identified in operating time or in complications. There was an average of 1610 mL of blood loss in the open thoracotomy group and 1032 mL in the endoscopic group.
Conclusions:
Both procedures are acceptable for the excision of a herniated thoracic disc. Percutaneous endoscopic thoracic discectomy imparts an added benefit of less postoperative pain and a shorter hospital stay than the open technique and may lead to fewer complications.
14. THE STRENGTH PROFILE OF THE THORACOLUMBAR ENDPLATE REFLECTS THE SAGITTAL CONTOURS OF THE SPINE
Purpose:
To map the strength profile of the thoracolumbar endplates using indentation testing.
Method:
Indentation testing was performed on the T9, T12 and L2 endplates of 6 fresh-frozen human cadaver spines using a materials testing machine (Dynamight; Instron Corp., Canton, Mass.). A minimum of 25 indentations were performed in a rectangular grid (7 columns by 5 rows, Fig. 1). A 3-mm hemispherical indendor was lowered at 0.2 mm/s to a depth of 3 mm, producing endplate failure.
Summary of results:
The failure load significantly varied with the AP and LAT positions (p < 0.0001). Each row was significantly stronger than the rows anterior to it (p < 0.04), except for the most anterior row. (Fig. 2) The most lateral columns were stronger than the central (range p = 0.04–.0002). The mean strength of the L2 posterior row was greater than that for the thoracic endplates (p < 0.01), while no difference existed between levels within the 2 anterior rows. The ratio of the mean strength for the posterior row compared with that of the anterior row was significantly different across level (p < 0.036). The ratios for L2, T12 and T9 were 1.35, 0.97 and 0.91, respectively.
Conclusion:
The periphery of the thoracolumbar endplate is stronger than the centre. The interaction identified between position and level suggests a relative strength increase in the anterior aspect of the endplate with rostral ascent into the thoracic spine.
Significance:
This knowledge may assist in preventing intervertebral implant subsidence by influencing implant positioning and design.

Rectangular grid of indentation sites.
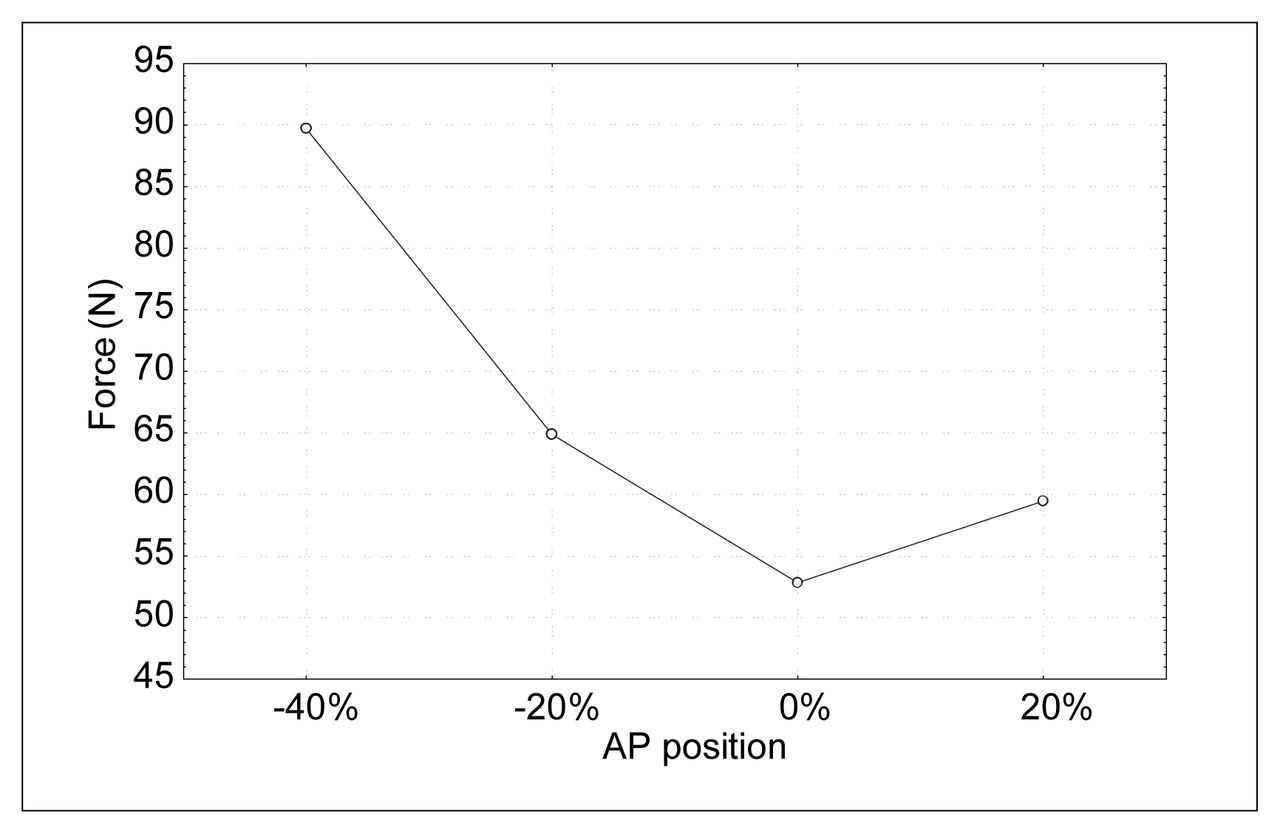
Anteroposterior position.
15. SURGEON RELIABILITY IN RATING COSMESIS IN ADOLESCENT IDIOPATHIC SCOLIOSIS (AIS)
Purpose:
To compare pediatric spine surgeons’ relative rankings of the importance of surgical considerations and their reliability of ratings of the physical deformity of patients with AIS.
Method:
First, 5 surgeons ranked the relative importance of 13 surgical considerations. Second, while viewing clinical photographs, surgeons rated the physical deformity of 40 patients with AIS (0 [best] to 5 [worst]) for shoulder blades, shoulders, waist asymmetry and the overall appearance of the back. Ratings were repeated 2 weeks later.
Results:
“Severity of deformity” was consistently ranked the most important surgical consideration. Surgeons varied widely in their reliability of their ratings of physical appearance, and their reliability was not related to experience; shoulder blades (κ = 0.34 mean; range 0.09–0.50); shoulders (κ = 0.22 mean; range 0.10–0.38); waist (κ = 0.24 mean; range 0.10–0.51); and overall appearance (κ = 0.40 mean; range −0.02–0.79).
Significance:
Given that 1 component of surgical decision-making is evaluation of physical deformity, low reliability suggests surgeons may not be consistent in their decision-making.
Conclusion:
The ratings of the specific physical features varied among surgeons. Although overall appearance had fair to acceptable reliability, the ratings of specific elements of physical deformity were often “poor.”
Funding:
This trial was funded by (in alphabetical order) DePuy, AcroMed, Johnson & Johnson Medical Products, The Canadian Institutes of Health Research and Synthes, Canada.
16. EN BLOC RESECTION FOR PRIMARY BONE TUMOURS OF THE SPINE
Purpose:
The objective of this study is to demonstrate that the principles of oncologic surgical resection, commonly applied to appendicular skeleton, may be used for the treatment of primary bone tumours of the spine with acceptable morbidity and satisfactory survival. Application of these principles to the spine will lead to more standardized reporting and potentially curative resections, as opposed to ill-conceived intralesional procedures that create a palliative scenario where wide resection was once possible.
Method:
A prospective cohort study design. All patients were staged preoperatively and discussed in a multidisciplinary conference. Tumours were classified using the Enneking and WBB staging systems. All specimens were submitted to 1 experienced musculoskeletal pathologist. Surgery was performed by the authors. Surgical approach, specimen margins, complications, adjuvant therapy, neurologic status and survival were prospectively collected.
Results:
Tumour resection was done on 19 patients (8 males, 11 females, average age 42 yr). After review by 1 pathologist, 11 resections were wide, 3 marginal and 5 intralesional. Average surgical time was 16.9 hours (4–39 h). There were 2 anterior approaches, 5 posterior and 12 combined anterior and posterior. Complications included 4 patients with excessive blood loss, 1 spinal epidural abscess, 1 incidental durotomy, 1 subarachnoid–pleural fistula, 2 wound infections, 1 pressure sore, 1 intraoperative myocardial infarction eventually resulting in postoperative death. There were no unexpected neurologic deteriorations. Diagnoses included 4 chordomas, 3 osteosarcomas, 2 osteoblastomas, 2 chondrosarcomas, 2 giant cell tumours, 1 of each PMNST, malignant fibrous histiocytoma, hemangioendothelioma, mesenchymal hamartoma, Pancoast’s tumour and alveolar soft part sarcoma. Disease-free survival was observed in 15 of 19. Average follow-up was 31 months (6–96 mo).
Discussion:
Wide or en bloc resection for primary spine tumours can be successfully performed with acceptable morbidity and mortality by a multidisciplinary team. Extensive and fastidious staging and standardized postoperative reporting is essential if future interinstitutional analysis is to be done. Surgery must be extensively planned and carried out by a team because of the length and complexity.
17. CONTROVERSIES IN PERFORMING ANTERIOR CERVICAL DISCECTOMY AND FUSION: A SURVEY OF PRACTICE PATTERNS AMONG CANADIAN SURGEONS
Objective:
The need for anterior cervical plating and the perioperative management of patients undergoing anterior cervical discectomy and fusion (ACDF) for single-level degenerative disc disease remains unclear. We surveyed Canadian spinal surgeons to characterize current practice patterns.
Methods:
A Web-based survey was conducted with neurosurgeons and spinal orthopedic surgeons in Canada. Questions asked included the use of fusion following single-level discectomy for degenerative disease, preferred fusion technique, frequency of use and indications for anterior plating, and the use of external cervical orthoses following ACDF. Demographic factors assessed included training background, and type and length of practice.
Results:
Sixty respondents indicated that their practice involved at least 5% spine surgery and were included in further analysis. Neurosurgeons made up 59% of respondents, and orthopedic surgeons 41%. Seventy-two per cent of respondents were in academic positions. Fusion was performed 93% of the time following ACD, with autologous bone used in 76% of cases. Neurosurgeons employed anterior cervical plates in 42% of ACDF cases, whereas orthopedic surgeons used plates 70% of the time. External cervical orthoses were recommended for 92% of patients without plates and for 61% of patients with plates. Surgeons who had been in practice for under 5 years were most likely to be performing spinal surgery, using anterior cervical plates and recommending postoperative use of cervical orthoses.
Conclusion:
Practice patterns vary among Canadian spinal surgeons. Nearly all surgeons perform a fusion following ACD, with many surgeons using anterior cervical plating for single-level degenerative disease. Training background, and type and length of practice appear to influence practice habits.
18. ANTERIOR CERVICAL RECONSTRUCTION AND INTERBODY FUSION USING TITANIUM HARMS CAGES WITH ANTERIOR PLATING
Study design:
A collaborative neurosurgery and orthopedic surgery outcome assessment study of titanium HARMS cage implants with anterior cervical plating in anterior cervical reconstruction and fusion.
Objective:
To evaluate the effectiveness and safety of using titanium HARMS cage implants and anterior plating in cervical reconstruction.
Summary of background information:
For over 40 years, anterior decompression and interbody fusion has been a widely accepted form of treatment for myelopathy/radiculopathy secondary to cervical spondylosis. Graft materials used in the reconstruction must provide structural support to the anterior column and allow for a high fusion rate, with minimal complications and failures. The most commonly used graft materials, autologous iliac crest grafts and fibular allografts, are associated with significant complications, which include donor-site morbidity, pseudarthrosis, collapse and extrusion of grafts.
Method:
Thirty patients underwent single or multilevel corpectomies using the standard Smith and Robinson technique, with subsequent placement of a titanium mesh cage packed with locally generated autologous bone graft, for stabilization and fusion of the anterior column. Anterior cervical plating was used in all 30 cases. Average follow-up period was 24 months and included clinical and radiographic evaluations.
Results:
After 24 months, all of the 30 patients experienced improvements in pain, sensation, power and overall function. Radiographic evidence of fusion was demonstrated in 97% of the patients. Two of the patients experienced complications: one intraoperative durotomy and the other cage slippage as identified on follow-up radiography.
Conclusion:
Titanium mesh cages packed with locally generated autologous graft provide adequate anterior column support, high fusion rate, positive patient outcome, with minimal graft complications and no donor graft-site morbidity. Titanium mesh cages with anterior plating is an effective and safe technique for anterior cervical reconstruction, while avoiding some of the complications of using bony strut grafts.
19. CLOSED REDUCTION OF CERVICAL SPINE FRACTURE DISLOCATIONS WITH MRI GUIDANCE
Closed reduction of the cervical spine for acute fracture dislocations has been a traditional technique used for re-establishing alignment and providing decompression of neural elements. The safety of this technique has been questioned, with concerns of disc migration and overdistraction cited as reasons to choose operative reduction and decompression as a safer option in some circumstances. A technique for monitoring the process of closed reduction using MRI scanning was developed. A case series of 15 patients with cervical spine fracture dislocations for whom closed reduction was recommended and carried out with MRI guidance is reported. Closed reduction provided early improvement in canal dimensions, even without complete reduction being achieved. The spondylotic spine may behave in a less predictable fashion with traction providing no significant decompression. Traumatic disc disruptions tend to return to normal positions with traction. One case of spontaneous reduction noted prior to traction therapy and resulting in neurologic worsening requiring emergent surgery is reported. MRI guidance in closed cervical reduction is a useful research tool for this technique. In the otherwise normal spine, closed reduction appears to be safe as used in this study, and is effective in effecting immediate spinal cord decompression.
20. ANTERIOR STABILIZATION FOR FRACTURE DISLOCATIONS OF THE CERVICAL SPINE
Purpose of study:
To assess the efficacy of anterior instrumentation and fusion for cervical spine fracture dislocations.
Methods:
Over an 18-month period, 46/52 patients with C-spine injuries requiring surgical treatment were followed prospectively. All patients underwent anterior approaches to stabilize and fuse the unstable segments using tricortical bone grafting and application of an anterior plate (CSLP, Synthes). Thirty-eight patients had single-level injuries treated with discectomy and fusion. Two patients had 2-level discectomies. Six patients underwent corpectomy and fusions for fractures of the vertebral bodies.
Summary of results:
There were no approach-related complications such as recurrent laryngeal nerve injuries, esophageal perforations, vascular injuries or strokes. One patient deteriorated neurologically. All other patients either improved neurologically or remained with their original findings. Two patients required oral antibiotics for superficial infections at the donor site. There were no spine infections, hardware loosening or graft extrusions. All bone grafts healed within 4 months both clinically and radiologically. Forty-one patients complained of minor or no pain after 4 months. Five patients continued to have moderate discomfort. One of these patients had a missed injury above his 2-level fusion with gradual progression into kyphosis requiring posterior stabilization.
Significance/discussion:
Halo-vest immobilization and posterior stabilization for C-spine fracture dislocations have been the treatment of choice for many surgeons. The low complication and failure rate has spurred on a gradual change toward anterior instrumentation and fusion. Our study very strongly supports this trend. We see little indication for the more invasive posterior approach given our present results.
21. THE FEASIBILITY OF TRANSARTICULAR SCREW FIXATION IN THE RHEUMATOID PATIENT
Introduction:
Significantly improved fusion rates have popularized the use of C1–2 transarticular screw fixation. A high-riding vertebral artery precludes safe bilateral screw placement in approximately 15%–20% of patients. We postulate this number to be higher in rheumatoid arthritis (RA) patients.
Method:
Retrospective analysis of 24 RA patients treated for their occipitocervical instability at our institution. Imaging studies and chart information were reviewed. Measurements taken from sagittal reconstructed images were taken at 3 levels in the pars interarticularis. The presence of erosive disease was noted.
Results:
Twelve patients had bilateral transarticular screws, 4 patients had unilateral and 8 patients had none. Eight patients out of 12 had significant erosive pathology to prevent transarticular screw placement. Screw placement was deemed impossible in 3 based on anatomy and 1 secondary to previous Gallie fusion. Inability to place a transarticular screw was secondary to significant erosive pathology in 8/12, a high-riding vertebral artery in 3/12 and a previous Gallie fusion.
Discussion and conclusion:
In this small retrospective series of RA patients, safe placement of bilateral transarticular screws was only possible in 50%. Patients with RA seem to have more variability in the size of their pars interarticularis, further limiting the use of transarticular screw fixation. Erosive disease was the main reason for the inability to place a screw. This variability is based on anatomy and erosive disease.
22. ARTIFICIAL DISC INSERTION FOLLOWING ANTERIOR CERVICAL DISCECTOMY: REPORT OF 10 CASES
Introduction:
Fusion following anterior cervical discectomy (ACD) has been implicated in the acceleration of degenerative changes in the adjacent spinal segments. Discectomy followed by implantation of an artificial cervical disc maintains the functionality of the spinal unit, while still providing excellent symptomatic relief. We prospectively analyzed our clinical and radiographic outcomes in 10 cases of single-level cervical disc herniation treated with the insertion of the Bryan artificial cervical disc.
Methods:
Ten patients presenting with cervical radiculopathy, without evidence of myelopathy, were chosen as appropriate candidates for artificial disc insertion following ACD. Clinical and radiographic outcomes were collected prospectively for all patients. Neurologic, pain and functional outcomes were assessed preoperatively and at regular intervals following surgery. Operative data and any perioperative complications were recorded.
Results:
No complications were experienced during the insertion of the prosthesis. All patients experienced immediate postoperative resolution of their radicular pain. Postoperative radiographs confirmed accurate placement of the prosthesis and preserved mobility of the spinal segment, up to 12 months following surgery.
Conclusion:
Insertion of the Bryan artificial cervical disc prosthesis following anterior cervical discectomy for single-level degenerative disease is a precise and safe procedure. Long-term follow-up is required to determine whether its use will reduce the incidence of adjacent segment disease.
23. ANATOMIC CONSIDERATIONS IN POSTERIOR APPROACH TO VENTRAL EPIDURAL SPACE OF AXIS
A posterior approach through an extended C1 laminectomy for ventral epidural lesions may be desirable in selected patients. The craniocervical junction was studied using 3 cadavers and 10 normal CT scans of trauma patients to assess the feasibility of a posterior approach to the ventral epidural space at the level of the axis. A standard posterior dissection and C1 laminectomy was performed in each cadaver, followed by detailed measurements of the operative corridor to reach the posterior aspect of the dens. CT scan of each specimen was also obtained to correlate operative findings with imaging. Similar measurements were made in each of 10 CT scans done on consecutive trauma patients.
The posterior approach may be a useful alternative to the transoral route to lesions in the ventral epidural space at the atlantoaxial level.
24. MINOCYCLINE FACILITATES RECOVERY OF HIND-LIMB FUNCTION FOLLOWING SPINAL CORD COMPRESSION IN MICE
Ameliorating CNS tissue loss will improve functional recovery from spinal cord injury (SCI). Minocycline has many actions distinct from its antimicrobial action. These include inhibition of microglia activity, caspases-1 and 3, iNOS and MMPs, which are factors that may contribute to secondary tissue damage. We tested the hypothesis that minocycline confers neuroprotection after acute SCI. Mice were subjected to a compression injury at the level of T3–4. Half of the animals were given an injection of minocycline (50 mg/kg, ip) 1 hour after surgery, followed 24 hours later by a second injection of 50 mg/kg. Subsequently, treated mice were injected with a 25 mg/kg dose every 24 hours for the next 5 days. Control mice were injected with saline vehicle. Minocycline-treated mice had significantly higher scores in the BBB locomotor test at the earliest time tested (3 d). There was gradual but significant recovery out to 28 days with mice achieving a final score of 10 (weight-supported plantar steps) compared to a score of 4 (slight movement of all joints of the hind limb) in saline-treated controls. Minocycline-treated mice had significantly higher inclined plane scores at weeks 3 and 4 post-injury (p < 0.05). Histologic analysis of H & E-stained tissue indicates that lesion size was significantly reduced in minocycline-treated mice (p < 0.05). Finally, tissue processed with Bielchowsky silver stain indicates that there was axonal sparing with minocycline. As minocycline has a good safety record clinically, the results of the present study indicate that clinical trials with this compound are warranted in patients with SCI.
25. THE OPERATED-ROOM C-SPINE TRACTION TEST AS A METHOD OF ASSESSING CERVICAL INSTABILITY IN MULTIPLE TRAUMA PATIENTS. PROTOCOL AND PRELIMINARY RESULTS
Purpose:
To present the protocol and preliminary results of a modified White & Panjabi cervical stretch test in the assessment of cervical instability in multiple-trauma patients.
Methods:
Multiple-trauma patients having no radiographic evidence of cervical instability on static imaging are routinely protected in hard collars until able to cooperate with clinical assessment and/or undergo flexion–extension radiographs for concern with respect to possible discoligamentous instability in the neck. Beginning in January 2000, such patients who were going to the operating room were routinely assessed with a stress test incorporating fluoroscopically-controlled axial distraction to tensile limit of the neck followed by maximum passive flexion and extension stressing. In the absence of intersegmental hypermobility, cervical precautions and immobilization were considered unnecessary and discarded. Chart documentation was reviewed for outcome and complications after discharge from the hospital.
Results:
To date, 32 tests have been performed, and 26 cases had complete chart documentation available for review. No complications of the procedure and no missed instabilities have been identified. An average of 13 days’ collar immobilization was eliminated by this protocol. Two cases of ligamentous hypermobility without instability were identified, one at O–C1 and the other at C5–6; both patients were treated observationally and have done well. One case of an undisplaced C2 pedicle fracture in a massively traumatized geriatric case was confirmed as stable on the day of injury, eliminating the need for collar support until the patient died of multiple organ failure 21 days later. Two patients went on to have neck pain complaints on regaining consciousness but could be reassured that there was no instability.
Conclusions:
The operating-room cervical stress test is a practical and safe manoeuvre that can eliminate the requirement for collar immobilization in obtunded trauma patients, safely identify subtle ligamentous injuries without frank instability and confirm stability in cases of undisplaced fracture. Discussion: The operating-room cervical stress test is an effective tool in screening trauma patients for such injuries. It does not require access to MRI technology and can be used in any hospital with an operating room.
Significance:
Prolonged cervical collar immobilization and missed discoligamentous injuries of the neck in multiple trauma patients can be eliminated with the application of this test.
26. FACET RHIZOTOMY FOR NECK PAIN
Chronic neck pain from whiplash injuries continues to be an important clinical problem. More than 90% of patients present with no identifiable pathology on clinical and radiologic examinations. Although psychological factors, litigation and compensation often contribute to the clinical picture, physicians and other health care professionals treat the chronic neck pain patient with a variety of pain control techniques.
Recently, the facet joint has been proposed as the potential source for chronic pain after a whiplash injury, given the absence of bone and disc pathology and empiric evidence that soft-tissue lesions heal in 6–8 weeks.
We have treated 14 patients with chronic neck pain from a cervical acceleration injury by facet rhizotomy using the Bogduk technique under fluoroscopic guidance. 1 mL of 0.5% Marcaine was used. Of 14 patients treated, 10 had a successful outcome with long-term pain relief. There were no major complications, and some patients complained of pain at the injection site. These results are in keeping with published data on facet rhizotomy for whiplash-associated chronic neck pain. While these early results are promising, more study is needed to refine selection criteria and to examine long-term results.
27. A PRELIMINARY REPORT ON INTRADISCAL ELECTROTHERMAL THERAPY (IDET)
Introduction:
Intradiscal electrothermal therapy (IDET) is a treatment that is used to treat chronic low back pain. The SpineCath system used for IDET was approved in Canada in July 2001. The University of Ottawa Spine Surgery Unit is the first group in Canada to perform this procedure and report their results.
Methods:
This is a retrospective study on 3 patients who underwent the IDET procedure. To be considered for IDET these patients had a positive discogram prior to the procedure, pain at L4–L5 and/or L5–S1, no previous spine surgery, back pain greater than leg pain, lumbar pain longer than 6 months, disc space more than 50%, baseline Beck Depression Scale less than 20, no sequestered disc herniations and had exhausted all conservative therapy. Patients completed the Oswestry VAS, SF 36v2 and Beck Depression Scale preoperatively and postoperatively at 1, 3, 6 and 12 months.
Results:
Length of the procedures ranged from 35 minutes to 2 hours. The catheter was heated to between 80° and 90°. Heat was administered for 4–6 minutes. Catheter placement was complete in 2 cases. Follow-up is from 3 months to 1 year. All 3 patients showed improvements in their lumbar back pain. Two of the patients showed significant improvement on all of the outcome questionnaires. The other patient showed improvement on the VAS only.
Discussion:
Based on literature and our experience with IDET we suggest that IDET can be a beneficial, cost-effective treatment to a select group of patients.
28. ANTERIOR LUMBAR INTERBODY FUSION FOR PERSISTENT PAIN AFTER POSTERIOR FUSION
Persistent pain after posterior lumbar fusion has several etiologies, including pseudarthrosis, recurrent stenosis, psychological disorders, occult infection and discogenic pain. The objective of this study was to evaluate the functional outcome of patients undergoing anterior lumbar interbody fusion (ALIF) for suspected pseudarthrosis or discogenic pain after posterior lumbar fusion (PLF).
We reviewed the charts of 63 patients who had ALIF and identified 15 patients who had previous PLF. Ten patients were available to complete a NASS questionnaire and obtain recent radiographs. Three of these patients had a solid PLF identified radiographically, while 7 patients had documented pseudarthroses. Mean follow-up was 25 months (range 9–55). Five patients were WCB cases and 5 patients were smokers. There were 5 ALIF with solid fusions and 3 nonunions at 1 or more levels. NASS pain/disability scale averaged 43 and 46 in the discogenic pain and pseudarthrosis groups, respectively. Despite poor functional outcomes, only 1 patient responded that he would not have the surgery again. Sixty percent of patients stated that they would undergo the surgery again. We conclude that in our small series, ALIF for discogenic back pain did not provide good pain relief as has been previously reported and had similar outcomes to patients with pseudarthroses. We believe that ALIF alone for a symptomatic posterior lumbar fusion in a difficult patient population can provide good patient satisfaction.
29. EPIDEMIOLOGY AND DEMOGRAPHICS OF SPINAL CORD INJURY: A REGIONAL STUDY
Objective:
An appreciation of the epidemiology of acute spinal cord injury (SCI) is essential for medical care, resource allocation and primary prevention. We describe the incidence, demographic data and management of patients sustaining acute SCI treated at our tertiary care trauma centre.
Methods:
We performed a retrospective review of all patient charts with a diagnosis of SCI between January 1997 and July 2001. The variables assessed included: age, gender, length of hospitalization, type and mechanism of injury, type of associated spinal fracture(s), neurologic deficit and management.
Results:
One hundred and fifty-one patients with SCI were identified. A bimodal age pattern of SCI was found. The average hospitalization was related to the severity and the level of the neurologic deficit as well as associated systemic trauma. SCI was most common in the cervical region followed by thoracic and lumbar regions. Burst fractures and bilateral facet dislocations correlated with the most severe neurologic deficits. Cervical SCI had an equal number of cases with and without associated fractures. Management of thoracic and lumbar fractures associated with SCI was predominantly surgical, whereas cervical fractures associated with SCI had equal numbers of cases treated with external immobilization alone or with surgery.
Conclusion:
These results may be of use in future research endeavours, public resource allocation and primary prevention.
30. PRIMARY EXTRAOSSEOUS SPINAL EPIDURAL EWING’S SARCOMA
Introduction:
Primary extraosseous spinal epidural Ewing’s sarcoma is an unusual cause of cord compression. This case report illustrates a rare example of this malignant disease.
Methods:
A 33-year-old healthy male presented with myelopathy due to cord compression in the thoracic spine. The patient had a subacute onset of upper back pain and progressive paraparesis. MRI scan revealed an epidural lesion extending from T4–T7. A laminectomy was done at the appropriate levels and the cord was decompressed.
Results:
Pathological analysis confirmed the presence of Ewing’s sarcoma. Postoperatively, the patient’s strength improved and he became ambulatory. A metastatic work-up was negative. After receiving chemotherapy and radiation therapy, he has been disease free for 9 months.
Discussion:
The case study includes a review of the literature. In addition, details of the pathological and radiologic findings of extraosseous spinal epidural Ewing’s sarcoma are presented. So far, only 17 cases of this disease have been reported. In several cases, a herniated intervertebral disc was suspected as the cause of cord, cauda equina or nerve root compression. This misdiagnosis may lead to a delay in surgery and treatment. Good imaging techniques and a strong index of suspicion is necessary to rule out this very malignant disease. Inadequate data exist about the efficacy of chemotherapy and radiation and little is known about long-term survival. However, complete resection can lead to improved survival and prognosis.
31. POSTERIOR LUMBAR INTERBODY FUSION USING FEMUR ALLOGRAFT
Background:
Posterior lumbar interbody fusion (PLIF) is an increasingly popular means to fuse the lumbar spine. By substituting the conventional cages with intraoperatively shaped femur allograft, we have been able to replicate the success rates of PLIF while drastically cutting out the costs of the cages.
Methods:
A total of 12 patients who underwent lumbar interbody fusion between July 2000 and June 30, 2001, were included in this retrospective study. Follow-up visits occurred between 3 and 12 months. 15-mm rings of femur, which have been cut and shaped to the appropriate height and length intraoperatively, are ready within a matter of minutes to be used as a biological spacer in the intervertebral space.
Results:
The mean improvement in VAS for leg pain, from preoperative to postoperative was 5.4. The mean VAS improvement for back pain was 3.1. There were no new neurologic deficits. There were few cases of transient minor sensory radiculopathy, which all disappeared at the last follow-up.
Conclusions:
Custommade intraoperatively shaped femur allograft used for PLIF is an acceptable alternative to the more expensive cage. The femur ring is easy to shape to fit perfectly in the interbody space.
32. CERVICAL OPEN-DOOR LAMINOPLASTY: THE MINI-PLATE AND KEYHOLE TECHNIQUE
Background:
At the Ottawa Hospital, an increasing proportion of patients suffering from cervical myelopathy are being treated with our modified version of the cervical open-door laminoplasty. It is believed that this procedure may reduce the rate of post-laminectomy kyphosis.
Methods:
The charts of 12 patients were reviewed for presentation, pre- and postoperative radiologic evolution and outcome. Postoperative follow-up extended from 3–18 months. The surgical technique used was a modification of Hirabayashi’s technique. A unilateral opening is performed followed by a greenstick fracture contralaterally. The “door” is kept open by the use of a miniplate. Foraminotomy is achieved, when needed, by the keyhole technique.
Results:
Twelve patients were operated on for cervical myelopathy. Radiologic decompression was achieved in all cases. Complications included 1 wound infection and 1 transient C5 palsy. All 12 patients showed a certain degree of improvement.
Conclusions:
Cervical open-door laminoplasty using a mini-plate is an effective way to decompress the cervical cord. The complication rate compares favourably with anterior decompression. The late post-laminectomy kyphosis may be avoided with laminoplasty.
33. CURRENT OPTIONS AND FUTURE TRENDS IN IMAGING MANAGEMENT FOR SPINE SURGERY
Imaging continues to play a central role in spine surgery. Access to these studies in the clinic and operating theatre is essential. Diagnostic imaging services are moving toward electronic formats for image handling, storage and viewing for radiologists. Huge cost savings are possible for health care institutions by avoiding printed film. It is important at this time of transition that certain guidelines be established by the “end users” in spinal imaging to ensure that appropriate imaging is readily available for patient care. Current options for intraoperative image viewing, image handling and storage, and cost implications will be reviewed.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.