


Abstract
Objective: To assess whether patients with a fracture of the high superior pubic ramus have functional outcomes worse than those of the lower or more central superior pubic ramus.
Method: We carried out a retrospective cohort study of all patients with pubic ramus fractures seen in either the emergency department or outpatient clinic of a level-1 trauma centre in Montréal. Patients were grouped according to their fracture location, determined from radiographs of the anteroposterior pelvis. Harris Hip Score and Musculoskeletal Functional Assessment questionnaire (short form) data were determined by an independent observer.
Results: Both the hip score (p = 0.0024) and functional assessment (p = 0.0304) indicated that patients in the group with high superior fractures had significantly poorer functional status.
Conclusion: High superior pubic ramus fractures have a poorer prognosis with respect to functional outcome.
Fractures of the superior pubic ramus (SPR) are generally the result of a direct blow, often in elderly patients, and are the result of minimal traumatic force.1–3 Current literature continues to describe this injury as a pelvic fracture. Traditional teaching is that this fracture, when encountered without a concomitant posterior pelvic injury, is a stable fracture with minimal ring displacement.1
To the best of the authors’ knowledge, no delineation has ever been proposed to distinguish the fracture that occurs just outside the weight-bearing portion of the true acetabulum from a more medial SPR fracture. Definitely, this more medial injury, because of its inherent stability, is only rarely considered to require surgical stabilization.1 When Matta3 described the only relative indication for fixation of SPR fractures as a displacement > 2 cm, he was actually describing the medial type of SPR fracture adjacent to the pubic symphysis. Even with considerable displacement in the anterior–posterior plane, the SPR fracture rarely displaces laterally.3 When displacement does occur, it is thought to be secondary to injury to the attaching soft tissue: Poupart’s ligament, Cooper’s ligament and the insertion of the pectineus muscle. This lack of tendency for displacement, coupled with a plenitude of soft-tissue attachment, leads to favourable conditions for bony union, although sometimes in a non-anatomical position.3 Nevertheless, pubic ramus fracture non-union is a recognized entity, and open and percutaneous techniques for fixation have both been well described.4,5 Fixation is usually applied to treat continued pain after fracture and has not been advocated for early treatment of particular fractures.
The current study was initiated after clinical suspicion that patients referred to the orthopedic clinic for more lateral or high superior pubic ramus fractures (Hspr) had clinically functional outcomes inferior to their counterparts who sustained medial SPR fractures (Mspr). This notion became our study hypothesis. Definition of Hspr as a discrete entity may serve as a prognostic indicator for more aggressive therapy. Identification of patients with a predictably worse outcome may lead to further investigation and/or alter treatment recommendations for such fractures.
Method
This is a retrospective cohort study of trauma patients sustaining an SPR fracture. The trauma registry of a level-1 centre identified patients with isolated, stable pubic ramus fractures without symptoms of posterior injury, associated neurological or soft-tissue injury, or other medical comorbidity. Patients were included if their injury occurred 12 or more months previously (range 12–40 mo). This follow-up period represented only a single visit for evaluation in this study. At our institution, these patients are treated in the emergency department/short stay unit by a nonorthopedic team according to standard protocol. No follow-up appointments take place with the orthopedic or trauma service. In-hospital treatment for all patients includes analgesics and early ambulation. Protocol imaging includes radiographic but not computed tomographic (CT) examination unless posterior pelvic or spinal pain is present.
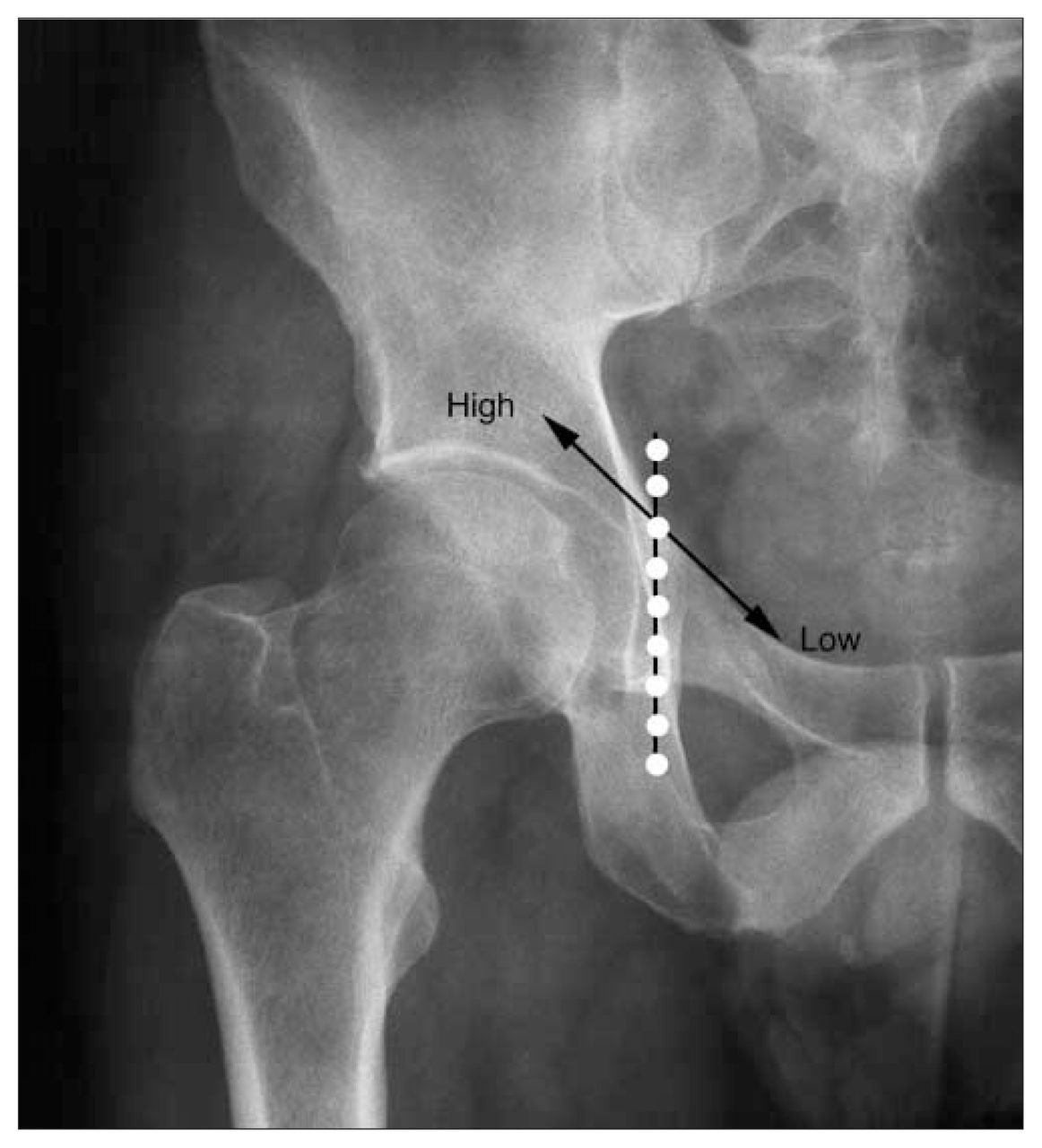
All radiographs of study patients were reviewed and categorized. Review of the chart and subsequent interview ensured that each case was an isolated fractures without injury to the posterior pelvis, spine, neurological or other soft tissue, or other concomitant trauma. Cases were categorized into the Mspr or Hspr group according to the location of the fracture relative to a vertical line drawn along the medial edge of the acetabular teardrop on a plain film of the anteroposterior (AP) view (Fig. 1). This was chosen as a reference point so that screening evaluation was possible with a single AP radiograph. (The cost of further evaluation of these patients with a CT image or alternate views was not supported by current standard of care or hospital budgetary policy.) Any part of the fracture that crossed the teardrop line (Fig. 1) placed the patient in the Hspr group. Consensus was obtained after 3 independent reviewers had evaluated the radiographs.

An anteroposterior radiograph of the pelvis. The vertical (dotted) line along the medial edge of the acetabular teardrop was used to classify pubic ramus fractures as high or relatively low (i.e., medial).
Thirty-six patients agreed to return to the hospital for orthopedic examination 12–18 months after their injury: 18 in the Hspr and 15 in the Mspr group. The remaining 3 patients were excluded: 1 because of a recent additional injury, and 2 because of secondary-gain issues.
All 33 patients completed the Musculoskeletal Functional Assessment (MFA) questionnaire (short form)6 and were evaluated with the Harris Hip Score. Data were also collected on patient demographics, time since the injury and Orthopædic Trauma Association (OTA) fracture classification. Patients were also asked a single question, “Is hip pain the biggest factor limiting your mobility?” All patients had a physical exam. MFA data were used as an overall score and also broken down into the bother index and the functional index. The 2 groups were compared with a 2-tailed Wilcoxon nonparametric test for continuous variables to ensure identical populations according to comorbidities and other demographics.2
Results
Clinical examinations revealed no cases of nonunion. The average age in the Mspr group was 46.8 years, 46.1 in the Hspr group (p = 0.77). Follow-up radiographs were obtained in 16 cases; fracture fragment location was judged to be unchanged compared with the original AP pelvis view for these patients. No nonunions were observed upon radiographic follow-up.
When data from the groups were compared, statistically significant differences were found for the Harris Hip Score (p = 0.0024; Fig. 2), the MFA (p = 0.0304; Fig. 3) and its bother index (p = 0.0338; Fig. 4) and functional index (p = 0.0385; Fig. 5) scores. Patients with Hspr were much more likely to state that hip pain on the affected side was the limiting factor in their mobility (p = 0.011; Fig. 6). When examined for confounding variables, patient age, sex (p = 0.668), length of time since the accident (p = 0.5287) and OTA fracture classification (segment 61: pelvic ring) were all found not to differ significantly between the 2 groups.

Patients with medial superior pubic ramus fractures (white columns) had significantly better function (p = 0.0024 by the 2-tailed Wilcoxon test) than those with high fractures (dark columns) when measured with the Harris Hip Score.

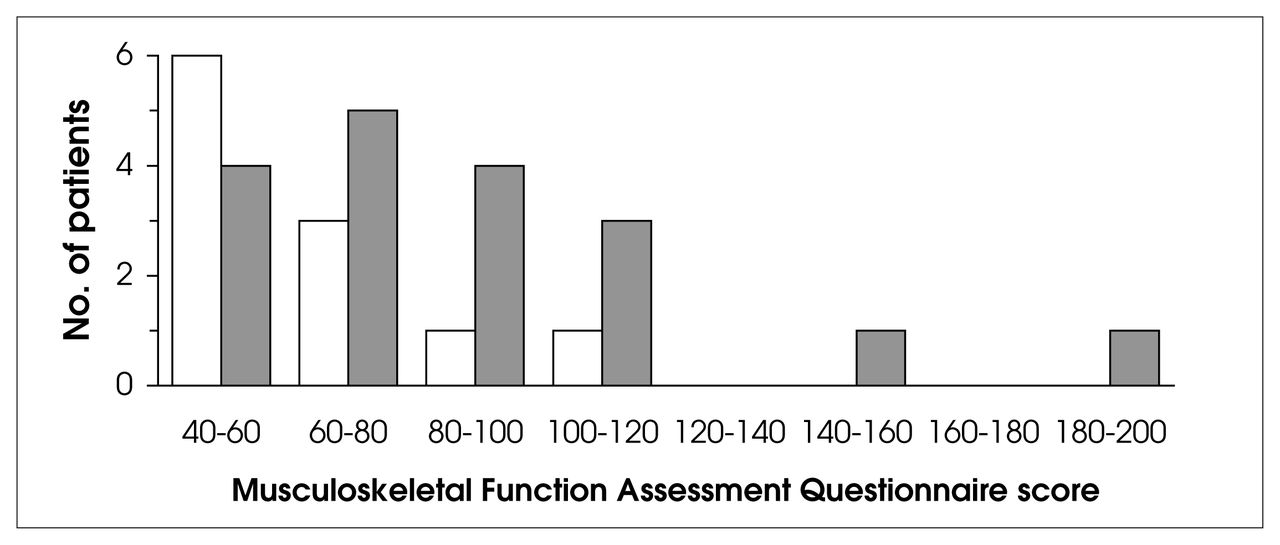
Patients with high superior pubic ramus fractures (dark columns) scored significantly higher on the Musculoskeletal Functional Assessment questionnaire (p = 0.0304 by the Wilcoxon test), implying greater disability or impairment.

Patients with high superior pubic ramus fractures (dark columns) scored significantly higher (p = 0.0338 by the Wilcoxon test) on the bother index, indicating a poorer functional outcome.
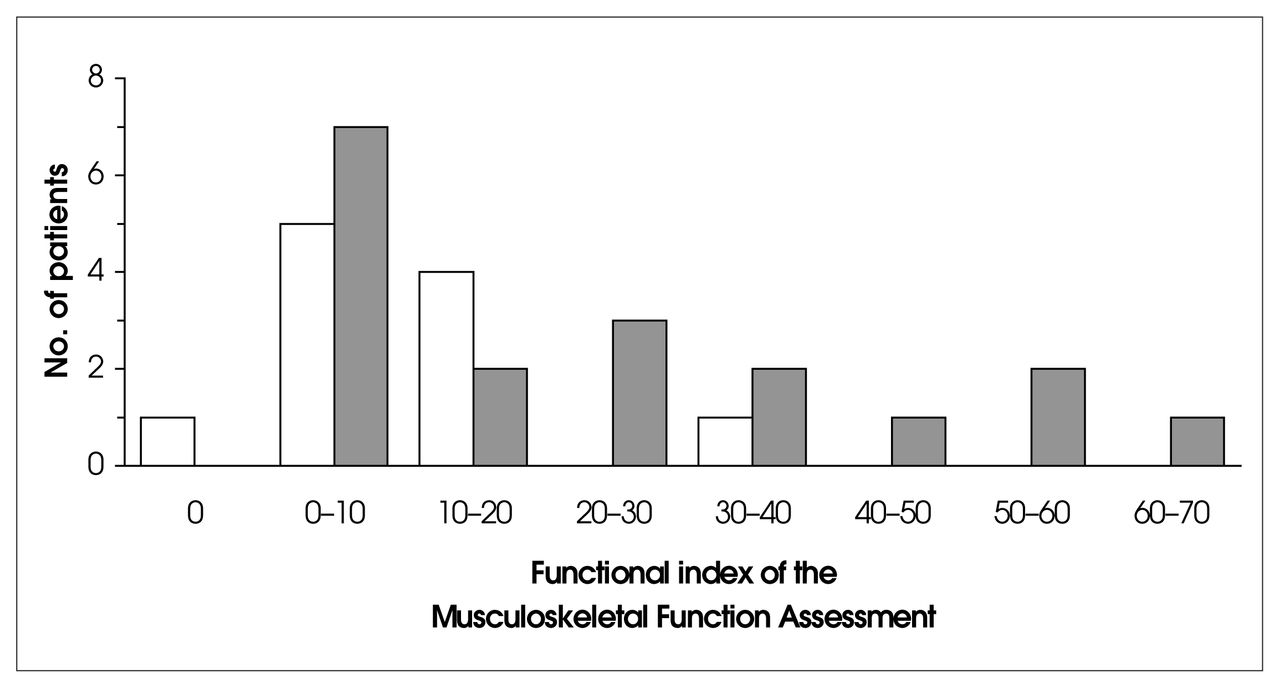
Significantly higher functional index scores likewise indicated worse outcomes for patients with high superior pubic ramus fractures (dark columns) than for those with medial superior pubic ramus fractures (white columns; p = 0.0385 by the 2-tailed Wilcoxon test).
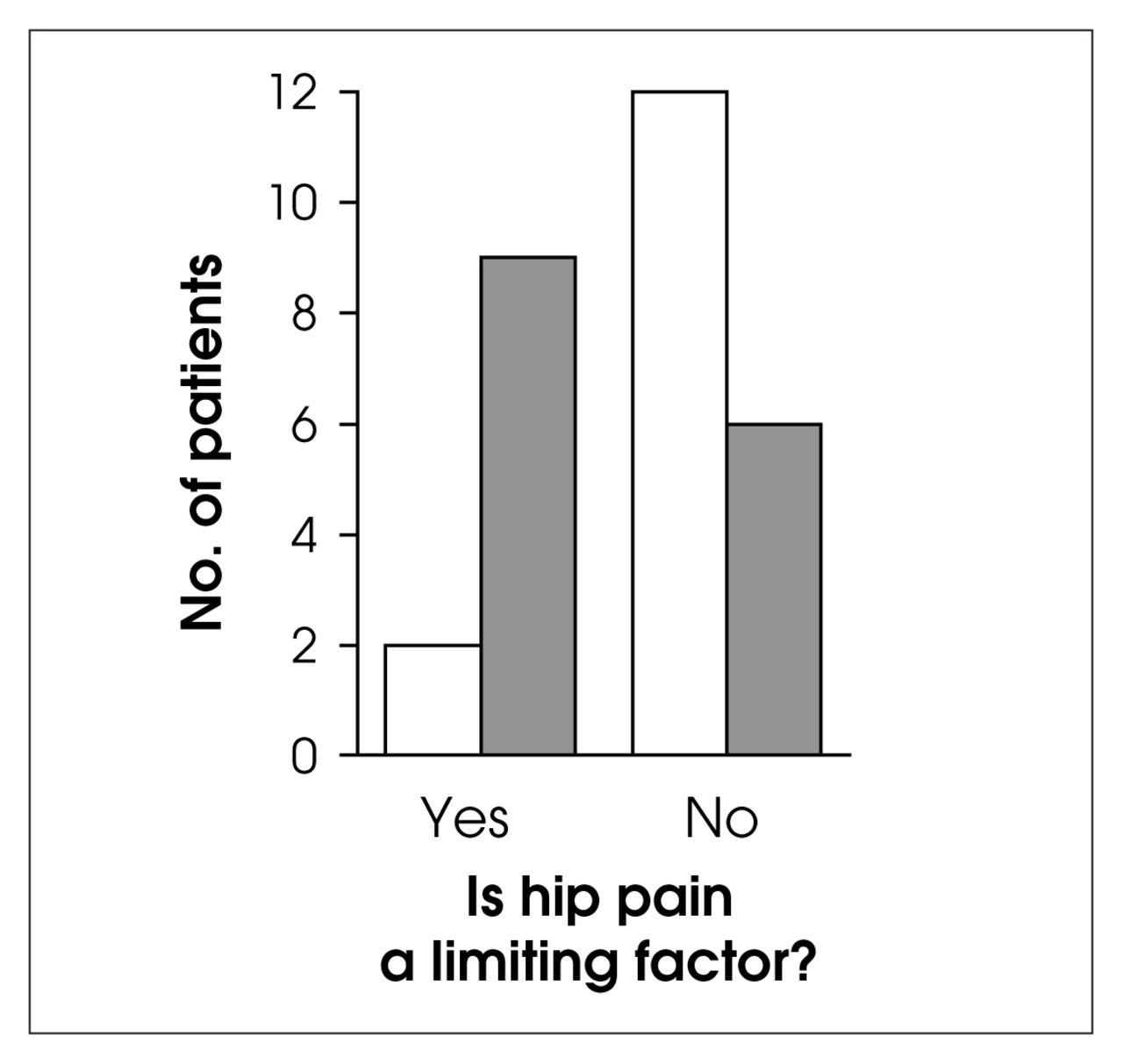
Significantly more patients with high superior pubic ramus fractures (dark columns) considered hip pain a primary limiting factor in their lives than those with medial superior pubic ramus fractures (white columns; p = 0.0024 by the χ2 test).
Discussion
SPR fractures are generally felt to be of minimal significance even when the fracture line approaches the teardrop on the AP radiograph. Common treatment regimes are usually limited to pain control and early mobilization. 2,3,5,7 We know of no clinical distinctions or treatment decisions that are made according to the level of this common fracture.
The hypothesis of our study was that patients with high SPR fractures had outcomes that were functionally worse if they had relatively low (medial) SPR fractures. Our statistical analysis confirms this hypothesis. The etiology of increased pain and functional disability in patients with high SPR fractures remains unclear, but the difference between the 2 identified clinical groups was distinct. Proximity of the fracture to the acetabulum is a prognostic indicator of poorer functional outcome. Certainly, these fractures represent a type of anterior-column involvement that has a detrimental prognosis even in relatively undisplaced fractures.
The decreased functional scores are tied to many factors, including general patient health; but our Mspr group of patients has had the same general medical concerns. Perhaps Hspr represents a more serious intra-articular injury of the acetabulum through either labral or cartilaginous involvement. Even though the mechanism seems identical, Hspr may have a greater energy transfer for the fracture to occur near the acetabulum, which may influence prognosis. In either case, the commonly held belief that superior pubic ramus fractures are trivial may indeed be incorrect.
This study also identifies a need for better definition of the pathology involved and proves a need for a prospective study plan. Koval and colleagues2 had noted that certainly some patients die after pubic ramus fracture, and that others definitely have decreased function and need institutional care. When evaluated by the Harris Hip Score and the Musculoskeletal Functional Assessment instrument, Hspr patients consistently scored significantly worse on functional testing for mobility and activities of daily living. The physical abilities of patients in the Hspr group were also more limited, as was post-trauma lifestyle adjustment. If early placement in a non–acute care institution or an alternative treatment or diagnostic procedure could be determined to aid patient recovery or to be cost-effective, such options could benefit patient care and overall hospital budget planning.
Footnotes
Presented in part at the Canadian Orthopædic Association Annual Meeting, Winnipeg, 2003.
Competing interests: None declared.
- Accepted June 15, 2004.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.