


Abstract
Background: With the aging of the North American population and therefore the need for more modern vascular surgeons familiar with open operations and less invasive diagnostic and therapeutic regimens, we wished to obtain suggestions and recommendations that would allow our training programs to more adequately fulfil these needs. Our objectives were to assess recent trends in Canadian vascular surgery training with respect to the trainee’s operative and nonoperative experience.
Methods: We mailed a survey to the directors of the 8 Canadian vascular surgery training programs, to ascertain the yearly operative volumes of their 3 most recent trainees with respect to 6 index operations: carotid endarterectomy (CEA), types I–IV thoracoabdominal aortic aneurysm (TAA) repair, elective open infrarenal aortic aneurysm (eAAA) repair, ruptured abdominal aortic aneurysm (rAAA) repair, endovascular abdominal aortic aneurysm repair (EVAR) and lower extremity arterial bypass (LEB). Additionally, information pertaining to nonvascular surgery rotations and the final practice location and type of practice for each trainee was requested.
Results: Seven (88%) of 8 program directors completed the survey. Between 1999 and 2002, vascular surgery trainees in Canadian training programs were exposed to the following yearly clinical volumes (expressed as mean [and standard deviation]): CEA 55.4 (33.9), TAA 6.2 (3.8), eAAA 63.8 (30.0), rAAA 13.5 (9.4), EVAR 14.9 (9.6) and LEB 74.5 (34.5). The range of yearly clinical volumes were: CEA 21–124, TAA 1–18, eAAA 30–133, rAAA 3–45, EVAR 0–34 and LEB 20–143. Nonvascular surgery rotations included: endovascular therapy, interventional radiology, noninvasive diagnostics and research. Forty-five (80.4%) of 56 recent graduates practise only vascular surgery. Most (73.2%) of our recent trainees have remained in Canada, with 41.1% settling in the province in which they trained.
Conclusions: Canadian vascular surgery training programs provide more than sufficient operative experience for their trainees. Although some programs have been successful at providing training in endovascular therapies, the integration of such experience in our training programs continues to be a challenge.
Vascular surgery has been recognized as a separate specialty by the Royal College of Physicians and Surgeons of Canada (Royal College) since 1983. Currently there are 8 established and 1 newly accredited university-affiliated training programs across the country offering 2 years of training to those who have completed general, thoracic or cardiac surgery residencies. These 2 years comprise 15 months of clinical vascular surgery and 9 months of other clinical or research rotations. On completion of training, surgeons are eligible to sit the Royal College examination in vascular surgery, with successful candidates receiving a Certificate of Special Competence.
With our rapidly aging population there is a recognized need for increasing numbers of vascular surgeons in both Canada1 and the United States.2 However, this is only one challenge facing our training programs. Perhaps more significant is the requirement that the modern-day vascular surgeon be facile with open operations and with risk-factor management and less invasive, or endovascular, diagnostic and therapeutic regimens. The most appropriate physicians to advise patients with peripheral vascular disease regarding treatment options are those trained in a wide array of treatment modalities. The vascular surgeon is currently the one with the broadest base of training and expertise and should reasonably be expected to expand this base as newer modalities are developed.
Traditionally, the basic skills required for endovascular therapies have been employed by physicians in such specialties as interventional radiology and cardiology. Unfortunately, recent attempts by vascular surgeons to obtain sufficient endovascular training have been met with difficulty and controversy.3 The present atmosphere is not unlike the one that existed more than 10 years ago following Dr. Fry’s presidential address to the Canadian Society for Vascular Surgery calling for increased utilization of duplex scanning and diagnostic vascular laboratories by vascular surgeons.4 Regardless, as the current reality requires vascular surgeons to be capable of offering patients standard and endovascular treatment options, it is essential that our training programs provide sufficient experience in these modalities.
The present study utilized a survey whose purpose was to identify recent trends with respect to the exposures and experiences a vascular surgery trainee might expect. We hoped that this would translate into suggestions and recommendations allowing our training programs to more adequately fulfil the needs of our future surgeons and, most importantly, our patients.
Methods
In early 2003, surveys were mailed to the directors of the 8 established vascular surgery training programs in Canada. Yearly operative case volumes were requested for their 3 most recent trainees (1999–2002) with respect to the following 6 selected operations: carotid artery endarterectomy (CEA), types I–IV thoraco-abdominal aortic aneurysm (TAA) repair, elective open infrarenal aortic aneurysm (eAAA) repair, ruptured abdominal aortic aneurysm (rAAA) repair, endovascular abdominal aortic aneurysm repair (EVAR) and lower extremity arterial bypass (LEB). No attempts were made to identify the trainee’s level of contribution or exposure (e.g., primary operating surgeon v. first assistant). Additional information was requested pertaining to nonvascular surgery rotations. As well, Royal College examination pass rates and the final practice location and type of practice for the trainees over the last decade were requested.
An identical follow-up survey was mailed 2 months later to any nonresponders to ensure maximum participation. All results are listed as mean (and standard deviation) and have been presented so as to not identify individual training programs.
Results
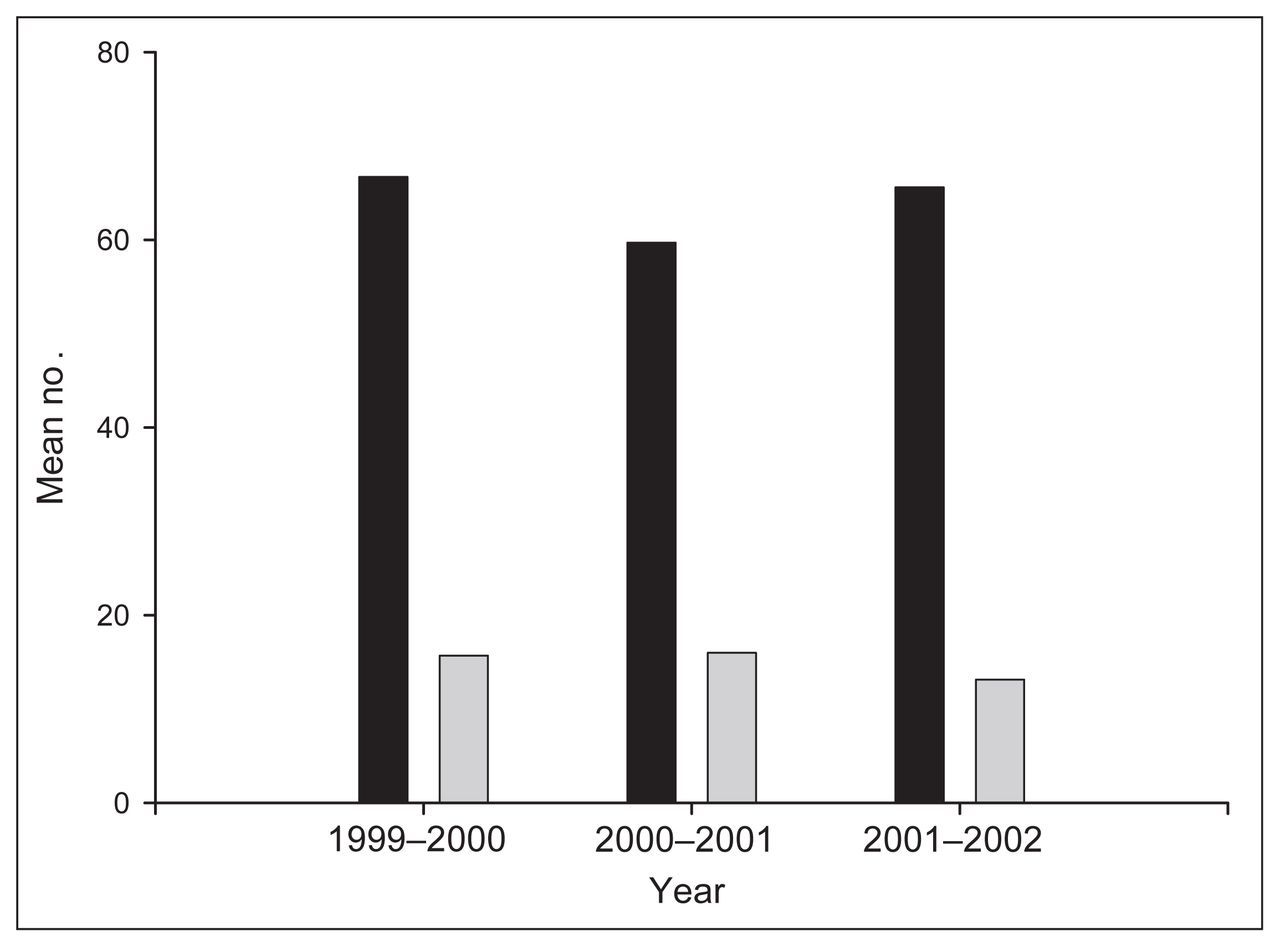
Seven (88%) of 8 program directors completed and returned the survey. Case volumes were obtained from a number of sources including computerized case logs and databases, hospital records and operative notes. The trainees’ yearly case volume means for each program are tabulated in Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5 for each index operation. The program directors provided data pertaining to their 3 trainees (21 in total). The national yearly means (SDs) and ranges are listed in Table 1 for the 3-year study period (1999–2002) with respect to these index operations. During this short 3-year study period, there were no statistically significant changes in the number of index cases that the trainees were exposed to. Specifically, with the introduction of EVAR there has not been a change in the number of eAAAs to which our trainees were exposed to during these 3 years (Fig. 6). This is consistent at both the national and individual training program levels.
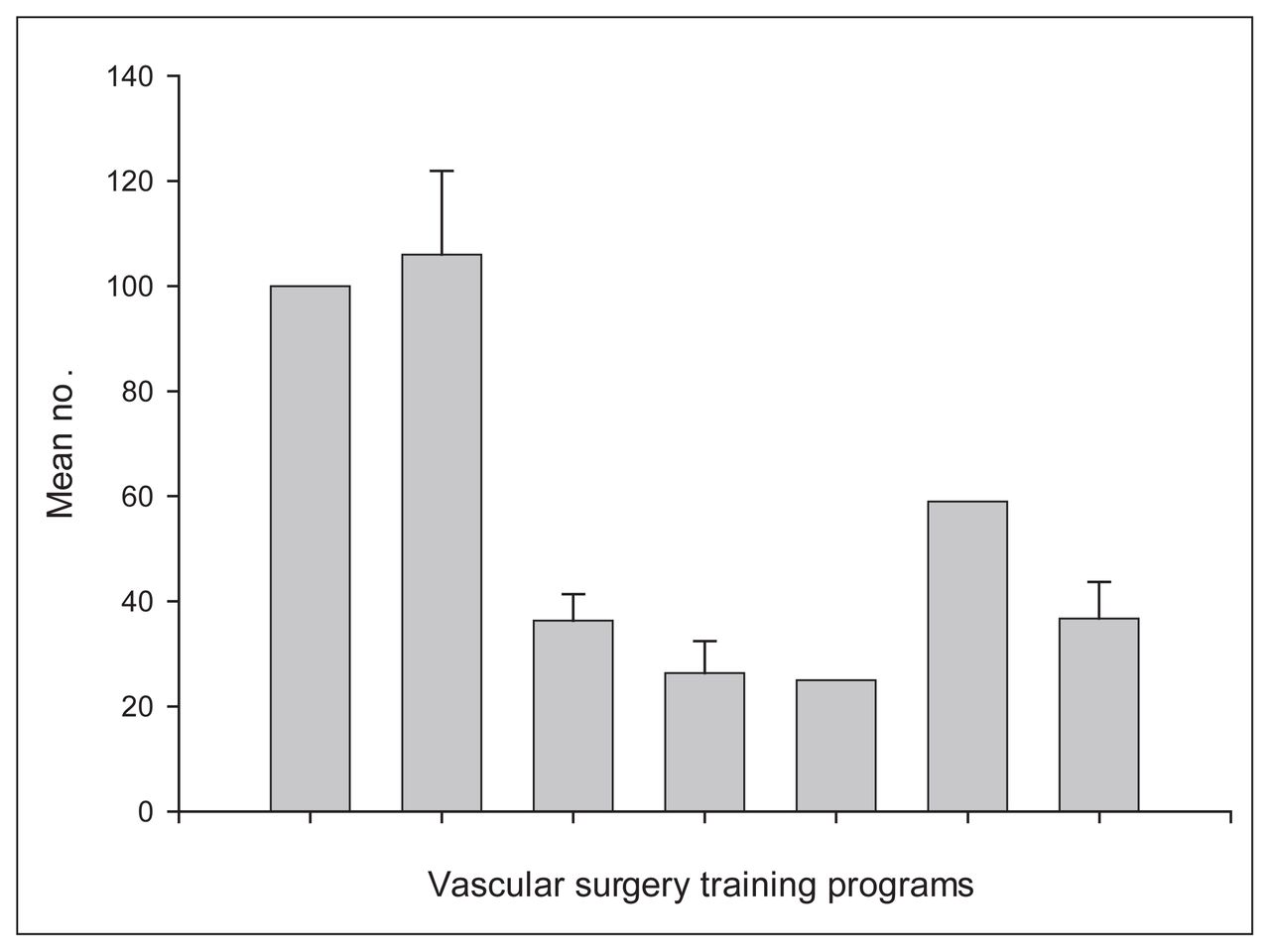
The mean number of cases of carotid endarterectomy performed per year for each trainee from 1999 to 2002.

The mean number of cases of thoracoabdominal aortic aneurysm repair types I–IV performed per year for each trainee from 1999 to 2002.

The mean number of cases of elective open infrarenal aortic aneurysm repair (black) and endovascular aortic repair (grey) performed per year for each trainee from 1999 to 2002.

The mean number of cases of ruptured abdominal aortic aneurysm repair performed per year for each trainee from 1999 to 2002.

The mean number of cases of lower extremity bypass performed per year for each trainee from 1999 to 2002.

Trends in the mean number of cases of endovascular (grey) and open (black) abdominal aortic aneurysm repairs performed per year for each trainee from 1999 to 2002.
Yearly clinical volumes for Canadian vascular surgery programs (1999–2002)
Nonvascular surgery rotations included exposure to endovascular therapies, interventional radiology, noninvasive vascular diagnostics and research (Table 2). Royal College examination pass rates remain high (40 of 41, 98%). Most vascular surgery trainees from the last decade practise 100% vascular surgery (45 of 56, 80%) and have remained in Canada (73%), with 41% remaining in the province in which they received their training (Table 3).
Nonvascular surgery rotations
Practice location of 56 trainees in vascular surgery
Discussion
The present study is unique in that, excluding a recent Danish study5 and a more dated paper from the United Kingdom and Ireland,6 there have been no published reviews describing vascular surgery training experiences from a national standpoint. The Danish study reviewed the operative case volumes of their recent vascular surgery trainees. Vascular surgery training in Denmark encompasses 3 years with at least 2 of those years occurring at a university-affiliated centre. Case-volume requirements do exist, with certification requiring a minimum of 200 major vascular procedures (includes CEA, eAAA and rAAA repairs, femoral–femoral crossover grafts, LEBs and thromboembolectomy) during training. The results of this study revealed a huge variation in the number of operations performed by Danish trainees, with a low exposure to CEA being of particular concern. The authors conclude that case volumes of all Danish surgical trainees are limited by the mandated 37-hour work-week under which they practise. At the time of this 2002 report, Denmark’s vascular surgery training programs were planning the adoption of case-volume minimal requirements for each index operation similar to their European colleagues. The earlier study from the UK and Ireland (1992) surveyed case volumes experienced by senior registrars and consultant surgeons. Trainees in both of these reviews were exposed to far fewer operative procedures than their contemporary Canadian counterparts presently described.
The current study used a survey to document the clinical case volumes to which our recent vascular surgery trainees have been exposed in the 12-month period that forms the majority of their 15 months of clinical vascular surgery experience. With 88% of program directors responding, this survey’s results offer a true representation of the current status of Canadian vascular surgery training. The 6 surveyed operations were chosen somewhat arbitrarily as the procedures that form the bulk of operative experience. Although no attempt was made to delineate each trainee’s level of contribution to an operative procedure, it is reasonable to conclude that as senior surgical trainees each would have performed some, if not all, of the key steps of most operations. This may not be the case, however, for such lower volume operations as TAA repair and EVAR. A possible weakness of any survey is that the study’s conclusions depend on the accuracy of the data obtained. The present data were obtained from a number of sources including case logs, databases and operative reports, but were all approved and confirmed by the respective program director.
Although vascular surgery trainees in Canada receive extensive practical exposure, the range of number of cases with respect to several operations is significant (Table 1). By reviewing the national means one may conclude that our trainees receive more than adequate exposure to these 6 procedures. However, significant disparity is evident when it is noted that several trainees received little if any exposure to TAA and EVARs during their 12-month clinical periods. Additional experience in these areas can be, and have been, obtained through rotations on other services or at other institutions. Nevertheless it is evident that there is significant variability among programs pertaining to case-volume mixes, in part due to surgeons’ clinical and research interests, local demographics and population, and referral patterns. It is essential to recognize this variability when national training standards and minimum case requirements are considered.
A specific concern primarily expressed in the US is that the introduction of EVAR may have a negative impact on a trainee’s experience with open aortic surgery. Contrary to this, several American centres have described an overall increase in aneurysm case volumes with the introduction of an endovascular program7–9 and a corresponding positive impact on their training programs. Although at some centres case volumes in eAAA repairs have decreased, 8 this reduction has been regarded as being more than offset by an increase in the proximal extent and complexity of open aneurysm repairs. During the 3-year period encompassing this study there was no significant change in the number of endovascular and open aneurysm repairs in which our trainees were involved (Fig. 6). The proportion of infrarenal aneurysms repaired with endovascular techniques did not change, although the absolute numbers are small compared with American programs. These trends are evident at the national and individual training program level. As most Canadian endovascular programs were instituted prior to this 3-year period, any impact of the introduction of endovascular techniques on open aneurysm case volumes may not be represented in this survey. However, unpublished data from our institution demonstrates the positive impact the introduction of an endovascular program can have on overall aneurysm case volumes and its respective training program.
During the 9 months of training during which clinical vascular surgery is not prescribed, trainees in Canadian programs can choose from several rotations. The most common rotations our recent trainees have experienced are endovascular therapy and interventional radiology, with slightly fewer programs offering dedicated research time or diagnostic vascular laboratory rotations (Table 2). This is in contrast to the US where 69% of American programs offer protected research time with a mean duration of 12 months.10 The choice of specific rotations in Canadian programs may be a reflection of the perceived requirements of individual trainees in the face of inter-program differences in clinical exposures. Given these differences the majority of Canadian programs cannot provide protected research rotations.
As a means of recognizing the increasing demands on vascular surgeons, training programs in Europe and the US have begun to institute minimum case number requirements to determine adequacy of training. Until recently, vascular surgery training in Europe has varied significantly among countries. Total duration of training has varied from 5 years (Spain) to as long as 11 years (UK), with prior general surgery requirements ranging from 3 to 7 years.11 Recently, a survey undertaken by the European Board of Vascular Surgery (EBVS) revealed that training in endovascular procedures is not part of the curriculum in only 3 countries (Denmark, Ireland and Norway), and it was not mandatory in the UK.12 Since then the training requirements of the EBVS have changed to include mandatory training in endovascular procedures. In order to be eligible to sit the European Board of Surgery Qualification in Vascular Surgery (EBSQ-VASC), a candidate must demonstrate sufficient experience in the form of a minimum number of index cases, including several open procedures, percutaneous transluminal angioplasty (PTA) and EVAR.11 These minimum case requirements are summarized in Table 4.11,13
American and European case-volume requirements
In the US, minimum case requirements have long been a component of vascular surgery training. Shortly after the process of accreditation and certification began in 1983, the Residency Review Committee for Surgery (RRC-S) established minimal operative vascular experience as 70 major vascular cases.14 At the time, regulations required familiarity with angiography and endovascular therapies but not the ability to perform these procedures. With the introduction of EVAR, demands on vascular surgeons, and by extension the training programs, increased. Trainees recognized these changes, and by 2000 only 50% of American vascular surgery fellows believed they were adequately trained in endovascular therapies at the completion of their program without additional training.15 These factors, among others, resulted in a remodelling of American vascular surgery training.16 The RRC-S reviewed society guidelines and care requirements for catheter-based procedures17 and with input from the Association for Program Directors for Vascular Surgery set minimum case requirements for several groups of procedures.13 All American vascular surgery training programs are now required to provide minimum case volumes in several procedural categories, including open operations, endovascular grafting, and diagnostic (angiography) and therapeutic (PTA) interventional radiology procedures (Table 4). Duration of training is also being discussed in the US, resulting in the initiative to form an independent American Board of Vascular Surgery.18 Significant intersocietal debate continues regarding the need for lengthening the duration of vascular surgery training with a corresponding decrease in general surgery training requirements.
Until recently Canadian vascular surgery training requirements have parallelled those of Australia,19 with both countries requiring a 2-year training period, most commonly after completion of a general surgery residency, with no minimum case-volume requirements. Despite this, the adoption of minimum case volumes by European and American training programs, particularly with respect to endovascular therapies, is certain to have far-reaching ramifications. As summarized in Figure 7, trainees from Canadian programs can come close to meeting or exceeding the European and American total case-volume requirements11,13 with most open procedures (CEA, eAAA, and rAAA repairs and LEB grafting) after 12 months of clinical exposure. However, several Canadian programs would currently have difficulty fulfilling the minimum case requirements for endovascular grafting, and few, if any, would fulfil the requirements pertaining to diagnostic and therapeutic interventional radiology procedures. In the short term this will result in our trainees being ineligible for certification in the United States and Europe. Irrespective of case-volume minimums, the designation of angiography, PTA and endovascular grafting as mandatory components marks a pivotal point in vascular surgery training. Currently, the adoption of mandatory minimum case volumes in Canada would be counter-productive as several programs would be unable to immediately provide sufficient experience in interventional radiology procedures and endovascular therapies. Rather than assigning mandatory minimum number requirements, these procedures should be designated as necessary components of vascular surgery training while avenues toward achieving this goal are explored. This could be accomplished with more efficient use and planning of the current 2-year training period without lengthening its overall duration.

Comparison of Canadian case volumes with international requirements. CEA = carotid endarterectomy, eAAA = elective open infrarenal aortic aneurysm repair, EVAR = endovascular abdominal aortic aneurysm repair, LEB = lower extremity arterial bypass, rAAA = ruptured abdominal aortic aneurysm repair and TAA = types I–IV thoracoabdominal aortic aneurysm repair. Black = United States training requirements,13 light grey = European Board of Surgery Qualification in Vascular Surgery,11 dark grey = mean Canadian yearly volumes.
Several instructive models of integrated training do exist. The University of California at San Francisco offers an integrated fellowship during which their fellows in vascular surgery and interventional radiology experience an identical year of training in interventional radiology and endovascular therapies.20 This is made possible by a unique level of cooperation between the 2 specialties. The University of Milan offers a 12-month program resulting in achievement of a Master in Endovascular Techniques and certification by the University and the Italian Health Department.21 This program is available to physicians who have completed training in vascular surgery, interventional radiology, interventional cardiology or neuroradiology and encompasses experience with angiography, PTA and endovascular grafting.
At present in Canada the necessary cooperation among specialties to achieve such an integrated training program has not been forthcoming in many centres. As each training program has found local solutions, elusive national discussions and resolutions are necessary at the Society and Royal College Specialty Committee levels. Certainly some integration of these training programs would be beneficial to all involved. Failing this, however, experience in interventional radiology techniques and endovascular therapies will continue to be necessary components of vascular surgery training. If our trainees cannot obtain sufficient experience through cooperation with other specialties they will have to rely on those vascular surgeons who, for the most part, have gone elsewhere to learn these techniques. There is already experience with this training option at a Canadian centre.22 As our patients will continue to require these therapies, our trainees will continue to rightfully demand sufficient experience from all of Canada’s vascular surgery training programs.
Conclusions
Advances in knowledge and technology continue to place further demands on vascular surgeons and, as a result, our training programs must adapt. This study reveals that vascular surgery training programs in Canada provide more than sufficient operative experience for their trainees. However, the integration of experience in interventional radiology and endovascular therapies continues to be a challenge. Although attempts at cooperation and some aspect of training program integration should continue with other specialties, those vascular surgeons who have received sufficient experience should be prepared to train our trainees should these overtures fail.
To meet societal needs and expectations and to keep abreast of international changes with respect to endovascular therapies, the training programs in Canada must respond with the addition of appropriate skills and knowledge in this area. Additionally, standards for training of surgeons with established practices, with respect to these new therapies, should be initiated.
Acknowlegements
We thank and acknowledge the assistance of all program directors of Canadian vascular surgery training programs: Dr. Jean-François Blair, Université de Montréal; Dr. Jerry Chen, University of British Columbia; Dr. Claudio Cina, McMaster University; Dr. Thomas Forbes, University of Western Ontario; Dr. Randy Guzman, University of Manitoba; Dr. Georges Hajjar, University of Ottawa; Dr. K. Wayne Johnston, University of Toronto; Dr. Oren Steinmetz, McGill University.
Footnotes
Presented at the 25th annual meeting of the Canadian Society for Vascular Surgery, Victoria, BC, Oct. 24–25, 2003.
Competing interests: None declared.
- Accepted March 5, 2004.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.