


Breast carcinoma in men is extremely rare (< 1% of all breast cancers). The most common invasive subtypes are infiltrating ductal carcinoma (about 85% of tumours) and papillary carcinoma (5% of tumours).1 Lobular carcinoma represents only 1% of tumours.2 We report a case of lobular breast carcinoma.
Case report
A 64-year-old man presented with a painless mass in the left breast. His history showed no evidence of liver disease, and no medication had been taken; in particular, there was no history of hormonal treatment. Breast examination revealed a 3-cm firm mass without any enlarged axillary nodes. Mammography of the left breast showed a slightly infiltrative mass. Frozen section revealed an invasive lobular carcinoma. The patient underwent a modified radical mastectomy.
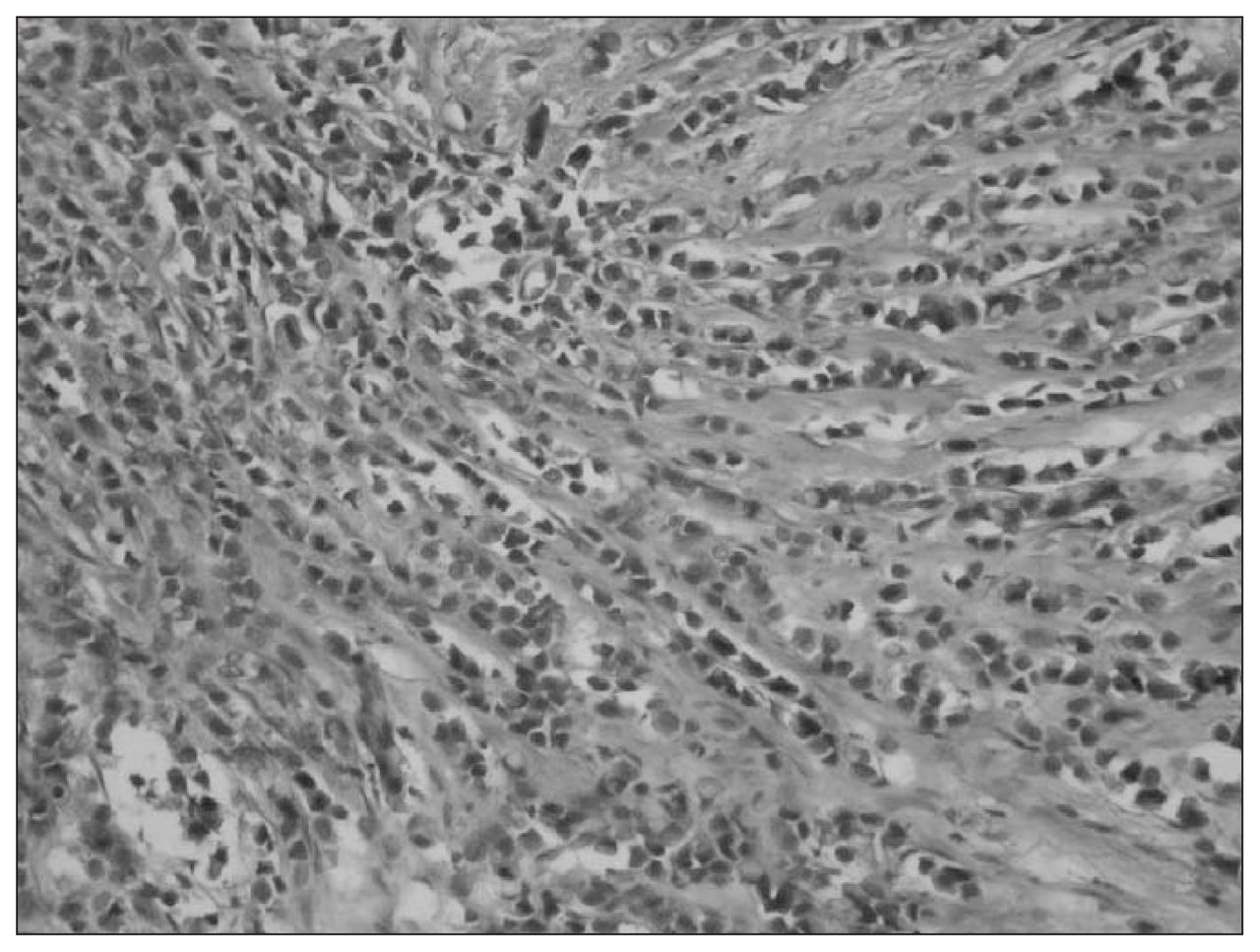
Histological examination of paraffin sections stained with hematoxylin and eosin revealed massive infiltration with small, relatively round tumour cells. Neoplastic cells displayed round-to-ovoid nuclei and a thin rim of cytoplasm with an occasional intracytoplasmic lumen. Loosely cohesive tumour cells diffusely infiltrated the mammary stroma (Fig. 1). Alcian blue–periodic acid-schiff staining was positive for intracytoplasmic mucin in tumour cells. Tumour cells were positive for estrogen receptor (40%), p53 protein (20%), c-erB-2 oncoprotein (diffuse) and MIB-1 antibody (25%), but negative for E-cadherin. Fifteen axillary lymph nodes were dissected and were negative for metastasis. A regimen consisting of cyclophosphamide (500 mg/m2), epirubicin (100 mg/m2) and 5-fluorouracil (500 mg/m2) in 6 cycles was given, and tamoxifen (20 mg/d for 5 yr) was prescribed. The patient is alive without any residual or metastatic disease 24 months after diagnosis.
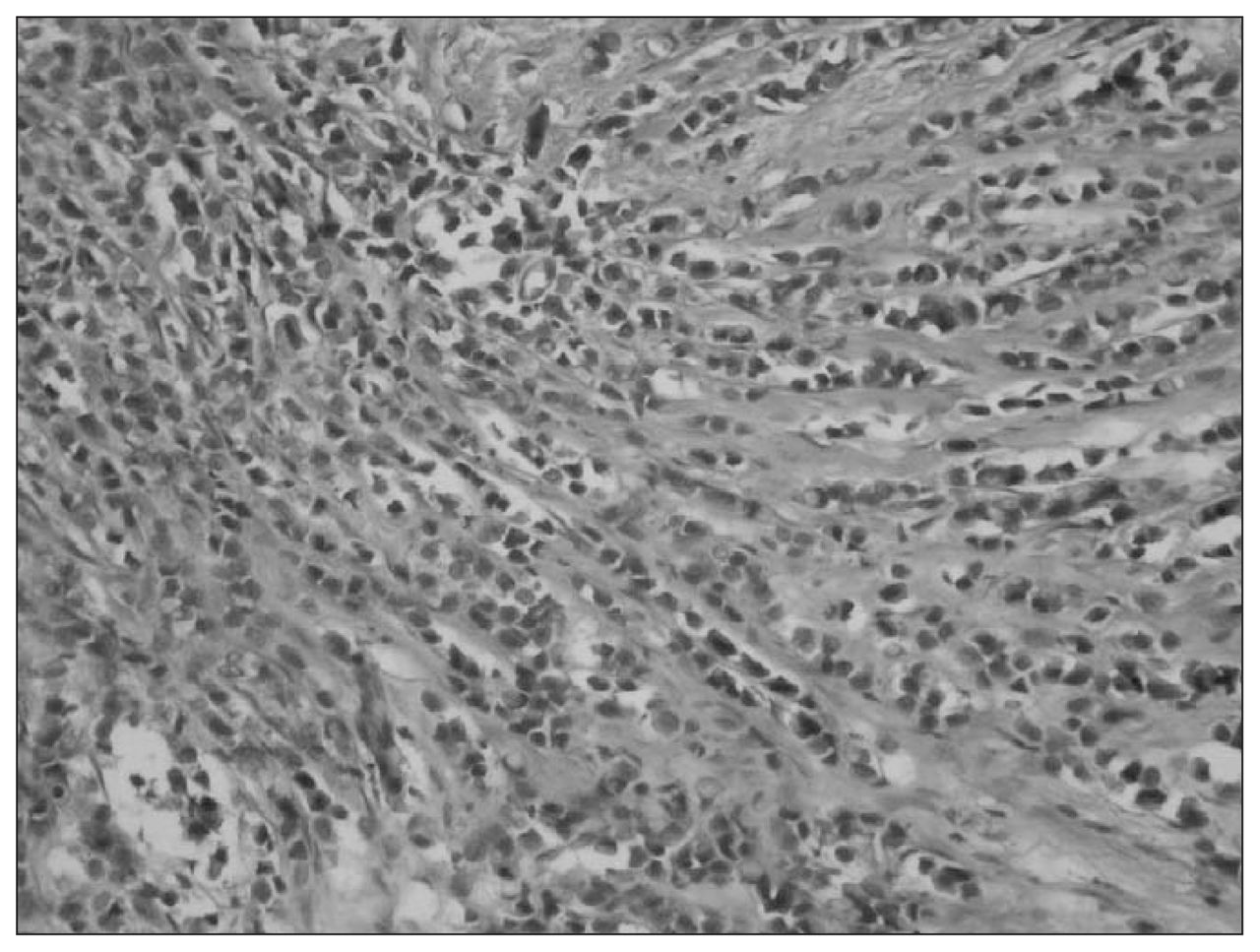
Infiltrating lobular carcinoma; isolated cells and small cords of cells can be seen invading the stroma (hematoxylin–eosin stain, original magnification × 100).
Discussion
Although the rate of male breast cancer in Western countries is approximately 1%, in Tanzania and in Central Africa the rate is 6% or more.3 The disease may be the result of an abnormal balance between estrogen and androgen. The risk is increased in patients with undescended testes, congenital inguinal hernia, orchiectomy, orchitis, testicular injury, infertility and Klinefelter’s syndrome.3
Lobular breast carcinoma in men is extremely rare because lobules and acini are not found in normal male breast tissue.2 However, lobules can be seen rarely in the male breast.4 Lobular carcinoma in situ has been reported in only 2 cases because of the absence of terminal lobules in the normal male breast. The only reported cases were in conjunction with invasive lobular carcinoma.5 In our case, although an in situ lobular component was not present, the characteristic histological appearance and E-cadherin negativity in tumour cells are reliable diagnostic criteria.
Carcinomas of the male breast have a higher rate of hormone receptor positivity than do those of the female breast when matched for tumour stage, grade and patient age. From a literature review, we found that 80%–85% of male breast cancers were estrogen-receptor positive and 26%–74% were progesterone-receptor positive.1,2 In our case, tumour cells were positive for estrogen receptor (40%) and negative for progesterone.
Although some factors favour early detection (frequent submammarian location, skin manifestation and thin soft-tissue cover), the interval between first complaints and diagnosis appears to be longer in men, so the tumour may be advanced at the time of initial diagnosis. Our patient did not have an advanced cancer, and no metastasis was seen.
Total mastectomy with axillary dissection is the optimum local therapy for the carcinoma of the male breast.6 Although the evidence is limited, most studies support a benefit for both adjuvant chemotherapy and tamoxifen in male breast cancer, particularly when the prognosis is poor.1
Footnotes
Competing interests: None declared.
- Accepted May 18, 2005.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.