


Although well-differentiated papillary and follicular thyroid cancers are treatable, 20% of patients have a recurrence associated with an 8% death rate. Earlier detection and effective management of local recurrence can improve the prognosis for these patients. These facts highlight the critical role of postsurgical monitoring for recurrent thyroid carcinoma. Traditional postoperative follow-up includes periodic serum thyroglobulin measurements and whole-body scanning (WBS) with the use of radiolabelled iodine-131 (131I) to localize the site of recurrence. 131I is administered therapeutically when uptake is demonstrated on WBS. However, there is a small but significant population of patients with an elevated thyroglobulin level and dedifferentiated recurrences that no longer trap iodine, leading to false-negative WBS results.1 This subgroup of patients presents clinicians with a true diagnostic dilemma, necessitating alternative imaging modalities for surveillance.
Several diagnostic tools are currently available for monitoring thyroid cancer recurrence with a negative result from WBS. The radiolabelled glucose analogue F-18 fluorodeoxyglucose with positron emission tomography (FDG-PET) provides important information regarding detection and staging of malignant lesions, owing to the increase in glucose metabolism associated with these tumours. However, FDG-PET imaging offers limited spatial resolution and a lack of identifiable anatomic structures, resulting in difficulty with precise localization of a tumour during surgical planning.2 CT scans offer high-resolution anatomic imaging, but CT is limited in its ability to distinguish between recurrent carcinoma and normal postsurgical changes.2 The recent development of PET/CT fusion imaging has combined the individual strengths of these 2 imaging modalities.3
Case report
A 40-year-old woman presented with palpable level 3 thyroid adenopathy on the right side. She had a history of papillary thyroid cancer treated with total thyroidectomy followed by 100 mcs of 131I 15 years earlier. Her last WBS was negative, and antithyroglobulin antibody titres were positive. A fine-needle aspiration biopsy of the mass confirmed metastatic papillary thyroid foci.
Preoperatively, the patient underwent PET/CT fusion imaging, which revealed cervical nodes 1 cm and 0.7 cm in diameter in level 3 and 4, respectively, on the right side and a nodule 0.8 cm in diameter in level 6 on the left side, all suggestive of metastatic disease (Fig. 1, Fig. 2). A right-modified radical neck dissection was carried out, sparing the internal jugular vein, accessory nerve and sternocleidomastoid muscle. The Nerve Integrity Monitoring-2 (NIM-2) endotracheal tube was applied to this procedure for recurrent laryngeal nerve (RLN) monitoring. The surgical pathology report confirmed that 7 of 20 lymph nodes were positive for metastatic papillary thyroid carcinoma. Three of the positive nodes were located in levels 3 and 4, with the largest measuring 1.8 cm in diameter and another displaying a small area of extra-capsular extension. Four of the positive nodes were located in level 6, with the largest measuring 1.3 cm in diameter and having no extranodal extension.
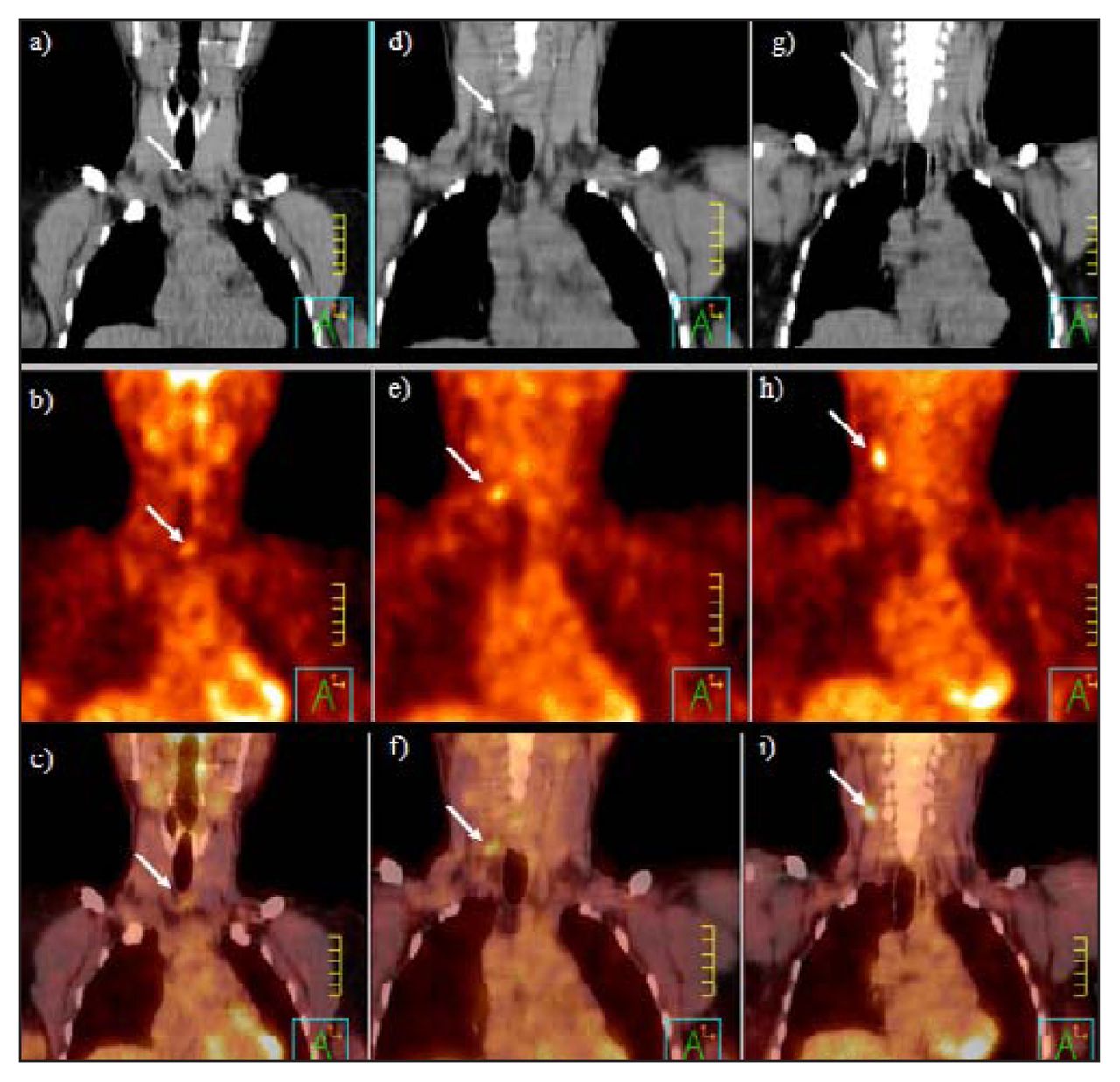
Top, middle and bottom rows correspond to coronal CT, positron emission tomography (PET) and combined PET/CT imaging, respectively. Arrows indicate a positive lymph node. the left column (a–c) shows a level 6 central compartment node measuring 0.8 cm × 0.5 cm, standard uptake value (SUV) 2.98. The middle column (d–f) shows a right-sided level 4 node measuring 0.7 cm × 0.3 cm, SUV 3.4. The right column (g–i) shows a right-sided level 3 node 1 cm in diameter, SUV 4.98.
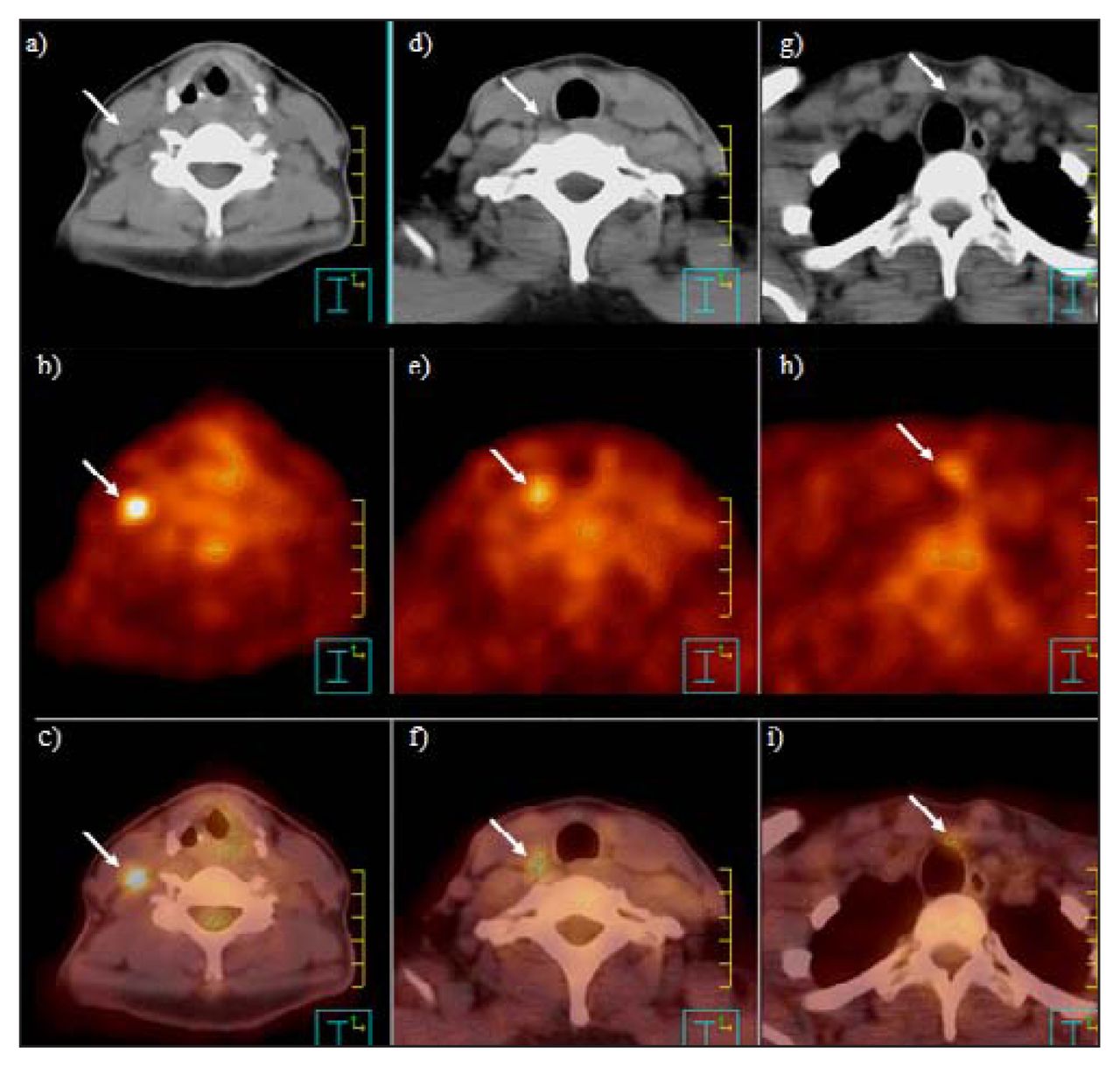
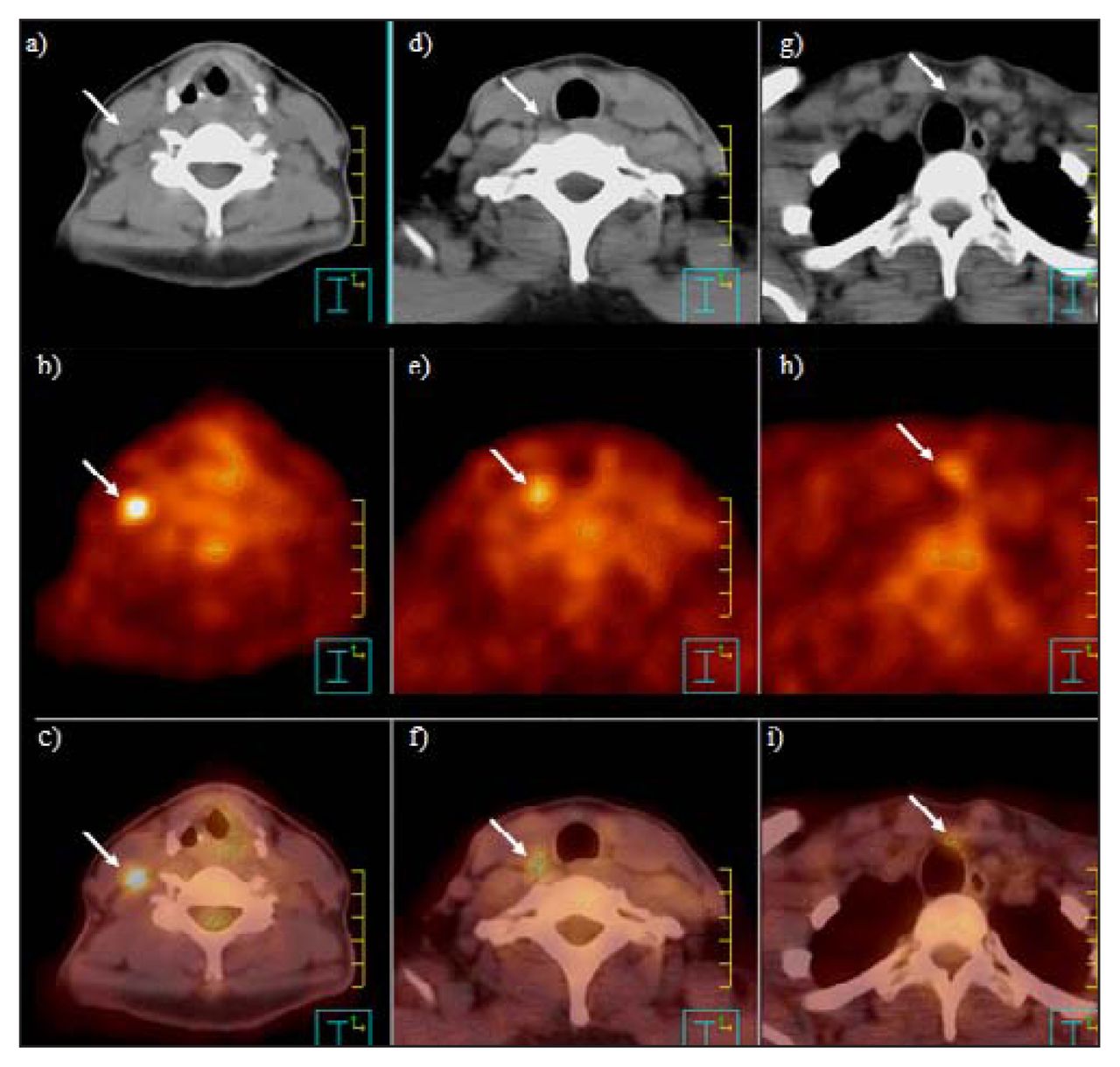
Top, middle and bottom rows correspond to axial CT, PET and combined PET/CT imaging, respectively. Arrows indicate a positive lymph node. The left-hand column (a–c) shows a right-sided level 3 node 1 cm in dimension, SUV 4.98. The middle column (d–f) shows a right-sided level 4 node 0.7 cm × 0.3 cm in diameter, SUV 3.4. The right column (g–i) shows a level 6 central compartment node 0.8 cm × 0.5 cm in diameter, SUV 2.98.
Discussion
The management of this patient was changed by the findings of the PET/CT fusion study. Imaging revealed a focus measuring 0.8 cm in level 6 that resulted in an extensive neck resection in the region bounded by the RLNs laterally, thyroid bed superiorly and innominate artery inferiorly. The involvement of the RLN necessitated the use of the NIM-2 endotracheal tube for electrophysiological nerve monitoring.
Nahas and colleagues3 monitored 33 patients for papillary thyroid cancer recurrence and demonstrated that PET/CT provided information beyond traditional imaging modalities, leading to an altered treatment plan in 40% of the cases. This was more likely in patients with negative WBS and serum thyroglobulin levels greater than 10 ng/mL.1–3 A combined PET/CT scanner allows for the simultaneous identification and anatomic localization of recurrent disease, resulting in precise distinction between normal tissue and juxtaposed neoplastic lesions.4 Regions localized as suspicious for recurrent disease by PET/CT imaging had an accuracy of 70% and a positive predictive value of 100% when correlated with histopathological findings.3 This may help improve oncologic results while minimizing the risks inherent with excessive or unnecessary explorations.
Another critical aspect in the management of this patient is the application of the NIM-2 endotracheal tube. RLN injury is one of the most dreaded complications of thyroid, parathyroid and neck dissections. Factors that increase the risk of RLN injury include operation for malignant disease, secondary operation, prior radiotherapy and anatomic distortion from goitre or neoplasm. The NIM-2 consists of an endotracheal tube with integrated bilateral paired electrodes that are exposed at the level of the glottis for vocal cord contact.5 It provides continuous electromyographic tracking in addition to the generation of electrically evoked potentials. The advantages of the NIM-2 over conventional needle electrodes include ease of placement, decreased risk of injury to the larynx and lack of obstacles in the surgical field.5 RLN monitoring provides feedback regarding nerve manipulation during surgery and allows for neural integrity assessment at the end of the procedure. Thus the endotracheal tube electode system may be particularly useful in more difficult cases of repeat exploration and recurrent malignant tumours of the thyroid gland.
Footnotes
Competing interests: None declared.
- Accepted December 12, 2006.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.