


Abstract
Objective: To develop a core curriculum for orthopedic surgery and to conduct a national survey to assess the importance of 281 curriculum items. Attention was focused on 55 topics pertaining to hip and knee reconstruction.
Methods: A 281-item curriculum was developed. We completed a content review and cross-sectional survey of a random selection of orthopedic surgeons whose primary affiliation was nonuniversity. We analyzed the data descriptively and quantitatively, using histograms, a modified Hotelling’s T2 statistic with the p value determined by a permutation test, and the Benjamini-Hochberg/Yekutieli procedure. Our analyses assumed that each respondent answered questions independently of the answers of any other respondent but that the answers to different questions by the same respondent might be dependent.
Results: Of 156 orthopedic surgeons, 131 (84%) participated in this study. Of 55 items ranked by all respondents, 42 received an average mean score greater than 3.5/4.0, and 51 received an average mean score equal to or greater than 3.0/40 (the standard deviation for each item ranged from 0.00 to 0.08), suggesting that 92.7% of the items are important or probably important to know by the end of residency.
Conclusion: This study demonstrates agreement that it is important to include 92.7% of the items that pertain to hip and knee reconstruction in a core curriculum for orthopedic surgery. Residency training programs may need to ensure that appropriate educational opportunities focusing on complex primary and revision surgery are available to meet the future needs of orthopedic surgeons whose primary affiliation is nonuniversity.
This paper is part of a larger study of the development and validation of a core curriculum for orthopedic surgery. One entire core curriculum was validated, and then 10 individual analyses were completed to clarify the content that residents should learn during residency in orthopedic surgery. This paper pertains specifically to core curriculum items relating to adult hip and knee reconstruction.
The World Health Organization (WHO) projects that by the year 2020 osteoarthritis will be the fourth leading cause of disability worldwide. Not surprisingly, the economic burden of illness generated from conditions as such arthritis will be enormous.1–11
The cost of illness resulting from musculoskeletal conditions was a main reason the WHO declared the years 2000–2010 to be the decade for bone and joint health, with a major aim being to increase education of health care providers at all levels. In Canada, the Bone and Joint Decade Undergraduate Curriculum Groups (BJDUCG) core curriculum recommendations for musculoskeletal conditions12 were validated in postgraduate education by 6 disciplines that manage patients with musculoskeletal conditions. These disciplines include family medicine, sports medicine, emergency medicine, physical medicine and rehabilitation, rheumatology and orthopedic surgery.13
The need to educate people with surgical skills to manage patients with hip and knee arthritis and related conditions will continue to be extremely important. Currently there are no guidelines on what orthopedic residents should be learning about musculoskeletal conditions involving the hip and knee. It is assumed that residents in all orthopedic training programs will become competent in performing primary total knee and hip reconstruction. However, no core curriculum content has been validated in the educational domain of adult hip and knee reconstruction.
An educational initiative to develop and validate an orthopedic curriculum designed to meet the needs of resident education in Canada was undertaken. This educational initiative was given full support by the Canadian Orthopaedic Association and Bone and Joint Decade Canada. In addition, the Specialty Committee for Orthopaedic Surgery of the Royal College of Physicians and Surgeons of Canada (RCPSC) and the Examination Committee for Orthopaedic Surgery in Canada specifically requested that this national survey to assess the importance of orthopedic curriculum items be determined by orthopedic surgeons whose primary affiliation is nonuniversity.
This study’s objective was to determine the importance of core content to be included in a core curriculum for orthopedic surgery, with a specific focus on content pertaining to adult hip and knee reconstruction.
The null hypothesis tested was that, on completion of his or her residency training, it is important for a resident to demonstrate equal knowledge of all items in the core curriculum for orthopedic surgery pertaining to adult hip and knee reconstruction or to perform all related procedures with equal proficiency.
Methods
Development of the outcome measure
A 281-item, 3-section questionnaire was developed. The previously validated international core curriculum for musculoskeletal health makes up the first section.13 Specialty objectives of the RCPSC specifically pertaining to orthopedic surgery make up the second cluster of items. The third section includes a complete procedure list based on codebooks from across Canada. Once this outcome measure was created, we compared it with the curricula of the various institutions to ensure that what the university programs thought to be important was also included.
The outcome was fully reviewed for content by 10 orthopedic surgeons (with FRCSC designation) of both sexes, representing adult and pediatric orthopedic surgery, education and research from within Canada and the United States. A modified outcome was then developed on the basis of feedback from this review, and the final questionnaire had 281 items. The questionnaire was translated into French to facilitate data collection from francophone orthopedists. This questionnaire is available on request from the corresponding author.
Randomization and cross-sectional survey
From the 2004 RCPSC list of actively practising orthopedic surgeons in Canada, 156 orthopedic surgeons whose primary affiliation was nonuniversity were randomized to this study via a random number table. The randomization was done in 3 separate processes to ensure appropriate representation from the Atlantic provinces and Quebec, central Canada (Ontario) and western Canada (Manitoba, Saskatchewan, Alberta, British Columbia and the 3 territories). These distributions were based on the numbers of orthopedic surgeons within regions.
A schedule for direct one-on-one interviews was arranged, and interviews were conducted in both official languages according to the functional language of each respondent. A cross-sectional survey was completed. The anglophone interviews were completed either over the telephone or in person, and the francophone interviews were completed via direct one-on-one interviews during a research tour through Quebec. Possible responses to each of the 281 questions were as follows: 0 = unable to assess; 1 = not important; 2 = probably not important; 3 = probably important and; 4 = important. A sample question is outlined in Box 1.
Sample item: “Please indicate the importance of the ability to perform with proficiency a cemented or uncemented hemiarthroplasty of the hip”
| Unable to assess | Not important | Probably not important | Probably important | Important |
| 0 | 1 | 2 | 3 | 4 |
Statistical analysis
We analyzed the data descriptively and quantitatively, using histograms, a modified Hotelling’s T2 statistic14 with p value determined by a permutation test, and the Benjamini-Hochberg/Yekutieli procedure.15–18 Our analyses assumed that each respondent answered questions independently of the answers of any other respondent but that the answers to different questions by the same respondent might be dependent. We used a histogram to summarize the average mean scores of items pertaining specifically to adult hip and knee reconstruction.
Each of the 131 identified orthopedic surgeons answered each of the 281 questions during the same sitting. Answers given to different questions by the same respondent must be considered related (“dependent”) to each other. Dealing with these dependencies entailed our using the modified Hotelling’s T2 statistic with a p value determined by a permutation test.
We then used the Benjamini-Hochberg/Yekutieli procedure to help us manage the large number of tests we did for differences between pairs of questions. This procedure showed definitively that questions are not all the same, in that the distribution of the ratings given to one question appeared to be different from that of another question for many pairs of questions.
The analysis first addressed all 281 items. Average ranked mean scores were obtained and listed in ascending order of importance for the entire core curriculum. This study high-lighted content pertaining to adult reconstruction of the hip and knee.
Results
Demographics
Of 156 orthopedic surgeons whose primary affiliation is nonuniversity, a sample of 131 participated in this study, for an overall response rate of 84%. There was a 90% response rate from the Atlantic provinces and Quebec and an 80% response rate from Ontario, the 3 territories and the western provinces of Manitoba, Saskatchewan, Alberta and British Columbia.
Of the respondents, 85% classified themselves as generalists and 15% as specialists. The average age of each respondent was 48.7 years. Each respondent had been in practice for an average of 16.8 years. Men made up 90% of the respondents and women 10%. The demographics of fellow-ship training experiences are outlined in Table 1.
Respondents’ fellowship training experiences (n = 131)
Orthopedic curriculum content for adult hip and knee reconstruction
The histogram (Fig. 1) demonstrates in graphical format the distribution of curriculum items pertaining to hip and knee reconstruction in ascending order of importance. Content pertaining to adult hip and knee reconstruction for the resident level of education is outlined in Box 2.
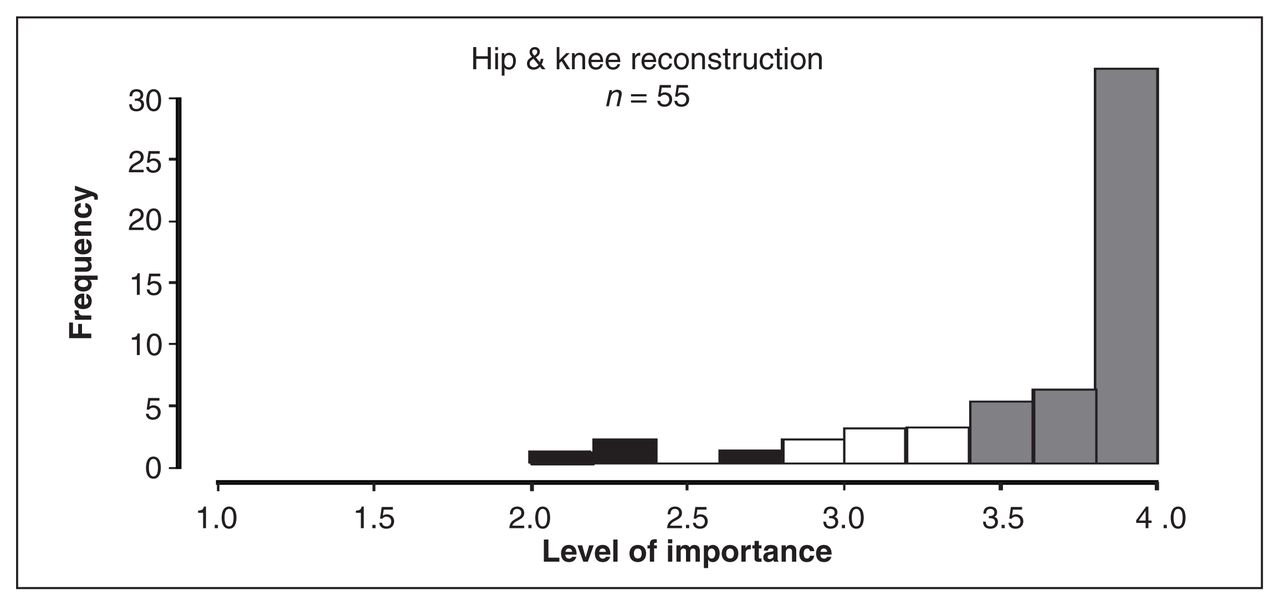
Histogram showing distribution of items for hip and knee reconstruction core curriculum content, based on level of importance according to respondents.
Core curriculum content for adult hip and knee reconstruction
| Item no. | Topic |
|---|---|
| 2.2 | Items that are NOT IMPORTANT to learn how to do with proficiency during a residency training program |
| 221 | Procedure — Osteotomy in the adult population of the pelvis |
| 2.4 | Items that are NOT IMPORTANT to learn how to do with proficiency during a residency training program |
| 178 | Procedure — Diagnostic arthroscopy of the hip |
| 151 | Procedure — Tendon transfers around the hip |
| 2.7 | Items that are Probably NOT IMPORTANT to learn how to do with proficiency during a residency training program |
| 152 | Procedure — Tendon transfers around the knee |
| 3.0–3.2 | Items that are PROBABLY IMPORTANT (“nice to know”) to perform with proficiency during a residency training program |
| 215 | Procedure — Arthrodesis of the hip |
| 118 | Procedure — Open reduction and internal rotation of the acetabulum |
| 216 | Procedure — Arthrodesis of the knee |
| 142 | Procedure — Synovectomy of the hip |
| 222 | Procedure — Osteotomy in the adult population of the femur (proximal and distal) |
| 246 | Procedure — Amputation and/or disarticulation through the hip |
| 188 | Procedure — Revision arthroplasty of the hip |
| 189 | Procedure — Revision arthroplasty of the knee |
| 174 | Procedure — Tenotomy of common tendons |
| 3.5–3.7 | Items that are IMPORTANT (“should know”) to be able to perform with proficiency during a residency training program |
| 186 | Procedure — Primary unicompartmental arthroplasty of the knee |
| 229 | Content — Understand and describe the principles of osteotomy of any bone |
| 223 | Procedure — Osteotomy in the adult population of the tibia (proximal and distal) |
| 48 | Content — Specify the signs and symptoms, predisposing factors, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with a crystalloid arthropathy |
| 197 | Procedure – Open reduction and internal fixation of a periprosthetic fracture of the hip/knee (shoulder/elbow etc.) |
| 278 | Content — Understand and describe the principles of a managing a patient with a limb-length discrepancy in the pediatric population |
| 275 | Content — Understand and describe the principles of limb salvage versus limb sparing versus amputation in the pediatric population |
| 45 | Content — Specify the signs and symptoms, predisposing factors, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with chronic inflammatory arthritis such as rheumatoid arthritis or any of the spondyloarthropathies |
| 143 | Procedure — Synovectomy of the knee |
| 198 | Procedure — Removal of total hip/knee components and insertion of antibiotic spacer |
| 3.8–4.0 | Items that are IMPORTANT (“MUST know”) to be able to perform with proficiency during a residency training program |
| 230 | Content — Understand and describe the principles of osteotomy of any bone |
| 249 | Procedure — Bone biopsy — superficial and deep |
| 244 | Procedure — Amputation and/or disarticulation through the knee |
| 248 | Procedure — Sequestrectomy and bone grafting |
| 39 | Content — Specify the signs and symptoms, the immediate complications, outline the assessment and investigations, outline the immediate and long-term management of a patient with soft tissue injures |
| 46 | Content — Specify the signs and symptoms, predisposing factors, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with a soft-tissue lesion or enthesopathy |
| 42 | Content — Specify the signs and symptoms, the immediate complications, outline the assessment and investigations, outline the immediate and long-term management of a patient with joint instability of the hip or knee (ankle/shoulder/elbow/finger) |
| 44 | Content — Specify the signs and symptoms, predisposing factors, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with osteoarthritis |
| 137 | Procedure — Arthrotomy of the hip or ankle |
| 247 | Content — Understand and describe the principles of amputation and/or disarticulation |
| 245 | Procedure — Amputation or disarticulation above the knee (through the femur) |
| 53 | Content — Specify signs and symptoms, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with metastatic bone disease |
| 243 | Procedure — Amputation and disarticulation below the knee |
| 54 | Content — Specify signs and symptoms, outline the assessment and investigations, propose a differential diagnosis, outline the principles of management of a patient with primary bone and soft-tissue tumours |
| 148 | Procedure — Fasciotomy for compartment syndrome of the lower extremity |
| 181 | Procedure — Arthroscopic menisectomy and debridement of the knee |
| 119 | Procedure — Open reduction and internal fixation of the patella |
| 183 | Procedure — Primary total hip arthroplasty |
| 185 | Procedure — Primary total knee arthroplasty |
| 114 | Procedure — Application of the external fixation device for fractures of the lower extremity |
| 179 | Procedure — Diagnostic arthroscopy of the knee |
| 111 | Procedure — Open reduction and internal fixation of the proximal tibia (tibial plateau fracture) |
| 27 | Content — Take a relevant history, identify and characterize major nontraumatic extremity problems including bone conditions such as malignancy and infections |
| 38 | Content — Specify the signs and symptoms, immediate complications, outline the assessment and investigations, outline the immediate and long-term management of a patient with joint dislocations |
| 106 | Procedure — Closed reduction and internal fixation of the femoral neck |
| 184 | Procedure — Hemiarthroplasty of the hip |
| 250 | Procedure — Bone graft harvesting from the iliac crest, distal radius, proximal ulna |
| 107 | Procedure — Closed reduction and internal fixation of the femoral shaft (intramedullary Nailing) |
| 108 | Procedure — Closed reduction and internal fixation of the tibia and fibula (intramedullary Nailing) |
| 109 | Procedure — Open reduction and internal fixation of the proximal femur |
| 110 | Procedure — Open reduction and internal fixation of the distal femur (bicondylar, supracondylar fractures) |
| 76 | Procedure — Joint injections and aspirations |
Of 55 adult hip and knee reconstruction items, 51 were given an average mean score of equal to or greater than 3.0/4.0 by all 131 respondents (Fig. 1), suggesting that 92.7% of the items (Box 2) are either probably important or important to know by the end of residency. The standard deviation (SD) for each item ranged from 0.00 to 0.08. In addition, the Benjamini-Hocherg/Yekutieli procedure demonstrates that, for 70% of the 1485 pairs of questions (55 × 54 / 2) pertaining to adult hip and knee reconstruction, the distributions of the ratings given to one question are different from that of another question for many pairs of questions. There is a false-discovery rate of less than 0.05 (Fig. 1).
Discussion
Currently, the expectation of the Specialty Committee for the RCPSC is that residents are graduating from their respective training programs with the ability to perform primary hip and knee reconstruction with competence. However, some questions arise: Are programs graduating residents competent to perform complex primary and revision procedures? Should residents be competent in their ability to perform such procedures around the hip and knee? Is the exposure to surgical hip and knee arthritic conditions and the ability to operate comfortably on such conditions specific to the fellowship level, or should this exposure also be given more serious attention at the residency level?
Our study suggests that orthopedic residents should be competent in their ability to know of and understand cognitive content pertaining to the ability to specify signs and symptoms and immediate complications. They should be able to outline the assessment, investigations and management plans for various musculoskeletal conditions such as arthritis, soft-tissue conditions, joint dislocations, joint instability, infections, malignancy and tumours, amputations and joint disarticulations, limb-length discrepancy and limb sparing versus limb salvage. Finally, they should understand the principles of managing patients with chronic inflammatory arthritis, such as rheumatoid arthritis or any of the spondyloarthropathies.
A specific focus on lower-extremity reconstruction procedures as they relate to arthritis, such as primary hip and knee reconstruction, unicompartment knee arthroplasty, osteotomy and removal of components and insertion of cement spacer in the presence of infection, were also identified as areas in which residents should have knowledge and competency on completion of residency.
In addition, lower extremity reconstruction procedures as they pertain to trauma, such as the ability to perform with proficiency a hemiarthroplasty, stabilization of lower extremity fractures and periprosthetic fracture fixation, will need to be emphasized.
Items considered to be less important include competency in more complex hip and knee procedures, including arthrodeses, joint disarticulations and some soft tissue procedures, along with competency in revision total joint procedures and stabilizing fractures of the acetabulum.
Items considered probably not at all important to be learned with proficiency during residency include tendon transfers around the hip, hip arthroscopy and osteotomies about the pelvis and femur. These procedures may reflect content that would be more suitable at the fellowship level of education.
The projected burden of illness for musculoskeletal conditions will be tremendous as our “front-end baby-boomers” enter their retirement years. By the year 2020, the WHO projects that, worldwide, 40% of a population that is living longer will be afflicted with osteoarthritis. These trends will specifically affect the number of joint reconstruction procedures performed by orthopedic surgeons. Epidemiologic data suggest that patient demographics of people receiving total joint procedures are changing19 and that many primary total joint replacements being performed will likely need to be revised at an exponential rate in the future.20 If these projections are true, then orthopedists whose primary affiliation is nonuniversity will need to be competent in these procedures. Will there be enough competent surgeons in Canada to meet these projected demands?
Previous studies indicate that educating orthopedic residents is expensive. 3,21–23 How residents are educated12,13,21–29 is not the focus of this particular study. However, educational planning will need to focus somewhat on cost-effective and efficient ways of educating future orthopedic surgeons to meet the projected health care demands. Residency training programs are uniquely positioned to implement suggestions and to provide solutions to ensure adequate surgical education in the area of hip and knee reconstruction. It will be important for programs to ensure that adequate learning opportunities are available for residents to learn the cognitive and technical skill sets essential to lower extremity reconstruction. 30
In addition, education tends to be driven by evaluation.31 Therefore, fellowship examination questions should reflect the areas being emphasized during training to ensure that what is being taught is also being evaluated. If examination questions reflect the areas of competence required for an orthopedic surgeon in the community, then residency training programs will tend to expose their residents to suitable learning experiences that will prepare them for success on the fellowship examination.
The strengths of the study included:
A previously validated international core curriculum for musculoskeletal health.
Randomization of orthopedic surgeons in 3 different regions of Canada and use of a translated outcome with direct one-on-one interviews, which may explain the 84% response rate.
A full content review before the study was conducted.
A translated outcome measure and direct interviewing of the francophone orthopedists, which may explain the 90% response rate from Quebec and the Atlantic provinces.
Full endorsement by the RCPSC Specialty Committee for Orthopaedic Surgery.
Unprecedented collaboration between the Canadian Orthopaedic Association and Bone and Joint Decade Canada for the sole purpose of improving education of orthopedic surgeons across Canada.
Study limitations include a positive response bias within the questionnaire and a limited scale grading the level of importance. As well, the wording of the questions asked each respondent to indicate the importance of either content or procedures. This implies that we are asking for opinions rather than asking about what respondents are actually doing.
Conclusions
Terminal and enabling objectives for orthopedic curricula pertaining to adult hip and knee reconstruction should focus on common problems of various musculoskeletal conditions, complex primary and revision procedures and the ability to manage complications.
The necessity to educate orthopedic surgeons in the area of adult hip and knee reconstruction within Canada will continue to be important. However, it is also our professional responsibility to ensure that surgeons entering into our health care system can in fact safely and competently deliver these services. Programs may need to consider strategies to balance the time that residents spend in the various disciplines of orthopedic surgery to ensure that specific content is learned and competence is evaluated. If these goals are not attainable, then other options, such as the development of regional referral centres, may need to be considered32 to meet current and projected health care demands for all Canadians.
Footnotes
Presented at the 2006 Annual Meeting of the American Academy of Orthopaedic Surgeons, March 22–26, 2006, Chicago, Ill., USA.
Competing interests: Dr. Wadey received funding support as the 2003 and 2004 Medical Education Travelling Fellow for the Royal College of Physicians and Surgeons of Canada. None declared for Drs. Maloney, Dev and Walker.
Contributors: Drs. Wadey, Maloney and Walker designed the study. Dr. Wadey acquired the data, and Drs. Wadey, Maloney, Dev and Walker analyzed it. Dr. Wadey wrote the article, which Drs. Maloney, Dev and Walker reviewed. All authors gave final approval for publication of the article.
- Accepted November 16, 2006.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.