


Abstract
Objective: Our primary objective was to evaluate demographic and causal factors of inhospital mortality for significant firearm-related injuries (i.e., those with an Injury Severity Score [ISS] > 12) in Canadian trauma centres.
Methods: We analyzed data submitted to the Canadian Institute for Health Information (CIHI) in the National Trauma Registry for all firearm-injured patients for fiscal years 1999–2003. Univariate and bivariate adjusting for ISS and multivariate logistic regression were performed.
Results: Men accounted for 94% of the 784 injured. In all patients, the percentages of self-inflicted, intentional, unintentional and unknown injuries were 27.8%, 60.3%, 6.1% and 5.7%, respectively. The inhospital fatality rate was 39.8%, with 83% of fatalities occurring on the first day. Two-thirds of patients were discharged home. Univariate and adjusted analysis found that ISS, first systolic blood pressure (BP), first systolic BP under 100, first Glasgow Coma Scale (GCS) score, age over 45 years, self-inflicted injury, intentional injury and injury at home significantly worsened the odds ratio of death in hospital and that police shooting was relatively beneficial. BP under 100, age over 45 years and a low GCS score had an adjusted odds ratio of death of 4.12, 1.99 and 0.64 per point increase, respectively. The multivariate model showed that ISS, BP under 100, first GCS score, sex and self-inflicted injury were significant in predicting inhospital death.
Conclusion: A predominance of young men are injured intentionally with handguns in Canada, whereas older patients suffer self-inflicted injuries with long guns. The significant number of firearm deaths, largely in the first day, highlights the importance of preventative strategies and the need for rapid transport of patients to trauma centres for urgent care.
In Canada, firearms are responsible for about 1000 deaths annually. However, for every person killed with a firearm, it is estimated that 2.6 more are injured.1 The lethal nature of these weapons ensures that a large portion of victims require significant medical care, and despite policy attention, it is estimated that criminal offences involving firearms cost Canadians $6.6 billion annually.2 Many authors have looked both at particular anatomic types of firearm injuries and at larger socioeconomic issues of gun violence.3–6 In the Canadian context, we have examined firearm mortality and the effect of various policy interventions on homicide and suicide rates.7–13 Unfortunately, little is known about patients who are seriously wounded by firearms in Canada or about what demographic and social factors contribute to their injury and outcome. The proportion of victims injured by self, intentionally or accidentally, has not been conclusively determined. The location of the incident and mitigating factors that could be useful in prevention strategies and in reducing the mortality of these patients has been largely unexplored.
In the United States, individual state-based injury reporting systems or national estimates have been researched. Beaman and colleagues14 examined firearm injuries that were cared for in US emergency departments and showed high levels of injuries to male patients from ethnic minorities and an overall fatality rate of 34%. This correlates well with another study from Galveston, Texas, that showed 30% overall mortality, with 80% of mortalities resulting from self-inflicted injuries.15 The US Centers for Disease Control and Prevention issued a thorough report on firearm-related injuries examining associated factors. The report’s conclusions were built on surveillance-based estimates of 91 centres that rely exclusively on emergency department reporting. This tends to limit the validity of the report.16 There are several US-based national studies on pediatric firearm injuries, but the external validity to the adult population is limited.
The primary objective of this study is to inverstigate all cases of significant firearm-related injuries (i.e. those with an Injury Severity Score [ISS] > 12) that survived transportation to Canadian trauma centres between fiscal years 1999 and 2003; we evaluate demographic and causal factors and their relation to inhospital mortality.
Methods
Data acquisition and elements
We obtained data from fiscal year 1999 to 2003 for all patients injured by firearms who were treated in Canadian trauma centres. Data were retrieved from information submitted to the Canadian Institute for Health Information (CIHI) National Trauma Registry (NTR), which is a national pooling of Canadian provincial trauma registries (http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=services_ntr_e). The provinces of British Columbia, Alberta, Manitoba, Ontario and Nova Scotia have participated since 1999, Quebec and New Brunswick since 2000 and Newfoundland and Labrador since 2003. Together, these provinces hold 95% of the Canadian population as defined by Statistics Canada, although trauma centres do not serve all patients. The NTR records data on patients in participating trauma centres. Included patients have an ISS greater than 12 and have either been admitted to a participating hospital or were treated or died in the emergency department.
The ISS is an internationally recognized scoring system for quantification of trauma. It is anatomically based and attempts to summarize multiple injuries with a single number and correlates linearly with death.17 The ISS is not the ideal marker for severity of injury in penetrating trauma, but it was universally collected by the NTR as a predefined trauma score, and it does represent a valid metric for severity of injury in penetrating trauma.
In this study, we investigated the following data elements for epidemiologic evaluation: patient age, province of injury, sex, date of injury, length of stay in hospital, ISS, first recorded blood pressure (BP), first recorded Glasgow Coma Scale (GCS) score, blood alcohol level, postal code, death in hospital, operations (if any were performed), site of disposition, International Classification of Diseases 9 and 10 (www.who.int/classifications/icd/en/) codes for intention of injury (self-inflicted, intentional or unintentional), weapon type, police shooting and location of incident.
Variables
The categorical variables examined in the study were intention in regard to the injury, weapon type and location of incident. We analyzed these variables with the use of dummy variables for each category with the referent groups of the unknown/other category. The categories for intention of injury consisted of self-inflicted, intentional, accidental and unknown/other. Weapon type consisted of handgun, long gun and other/unknown. Location of incident is categorized by the CIHI into home, street/highway, sports or athletic centre, industrial or other/nonspecified. Industrial sites include construction sites or factories; “sports or athletic centre” includes any location where a sport is played, such as a basketball court or football field. The data element “death in hospital” was defined as any death after the initiation of treatment in the emergency department.
The postal code of the patient’s home address was used to determine whether the residence was rural, defined as a location with a minimum population concentration of 400 people per square kilometer or a total population of less than 1000.18 When this data element is interpreted, however, it is important to stress that living in a rural area does not necessarily mean a rural place of injury. On chart review, we included the first recorded systolic BP and first recorded GCS score as important variables seen in presenting patients. The data for BP were analyzed both as a continuous variable and as a dichotomous variable (BP < 100 or BP > 100). Patients with an initial BP of 0 were excluded from analysis because BP of 0 was uniformly fatal in this study. We thus excluded patients whose initial BP of 0 would distort the relation between initial BP and probability of death. This exclusion permitted a more clinically relevant interpretation of the data.
We analyzed the data for age in 2 ways. First, the subjects were grouped into 5-year age categories. To allow for a simpler comparison between older and younger subjects, we performed a second analysis in which the age variable was dichotomized, dividing the subjects into 2 categories: below and above age 45 years.
The variable “blood alcohol” was transformed from its absolute number to a present/absent dichotomous variable. The same was done for police shootings and for whether any operation was performed. With regard to operative treatment, the complexity, variability and level of recorded information in the national registry made any more specific comment subject to too much error. The site of disposition was categorized by CIHI into home, home with support, rehabilitation, another acute hospital or other.
The values recorded for each variable are presented in Table 1.
Results of univariate logistic analysis of various demographic and clinical variables unadjusted and adjusted for ISS on death
Statistical analysis
Values and distributions of the data elements were examined. To better understand the patient population, we graphed intention, location and frequency of firearm injuries by age category. As well, to understand which weapons are most frequently associated, we examined weapon type as it related to intention of injury.
Missing data may be nondifferentially distributed (e.g., subjects with a normal GCS score may be more likely not to have their GCS score reported) and may be related to outcome. To avoid bias introduced owing to missing data, we used a multiple regression technique in which replacement values for missing data greater than 10% were imputed; all variables where data were present for more than 90% of subjects were used.19 These variables included rural residence, first GCS score and positive blood alcohol.
Time to fatality was recorded to establish a timeline from time of injury to death and the proportion of fatalities occurring in the first 24 hours. The severity and course of injury during the hospitalization was further examined, as indicated by the ISS, length of stay and site of disposition.
For exploratory purposes, we performed univariate logistic regression to evaluate the single-variable odds ratio on inhospital death with all variables. Further, to standardize for degree of injury, we used a bivariate logistic regression adjusting for ISS. Following the univariate model analysis, all variables with p values below 0.20 were entered into a logistic multivariate analysis. This was deemed strict enough to exclude random associations from the model and permissive enough to ensure that a true association was not excluded. While variables were categorized in multiple ways, we used only the dichotomized data to ease interpretation of results. For example, we used age of more than 45 years rather than precise ages because the interpretation of odds per year change in age is difficult to appreciate clinically. We explored interaction terms of all significant variables individually, using a likelihood ratio test. Higher-order interaction terms were not explored. Patients with a first recorded BP of 0 were not included in the multivariate analysis because to include those would bias results, as mentioned above.
Statistical calculations were done with Stata v9.0 (StataCorp, College Station, Tex.); the significance level was set at 0.05.
Results
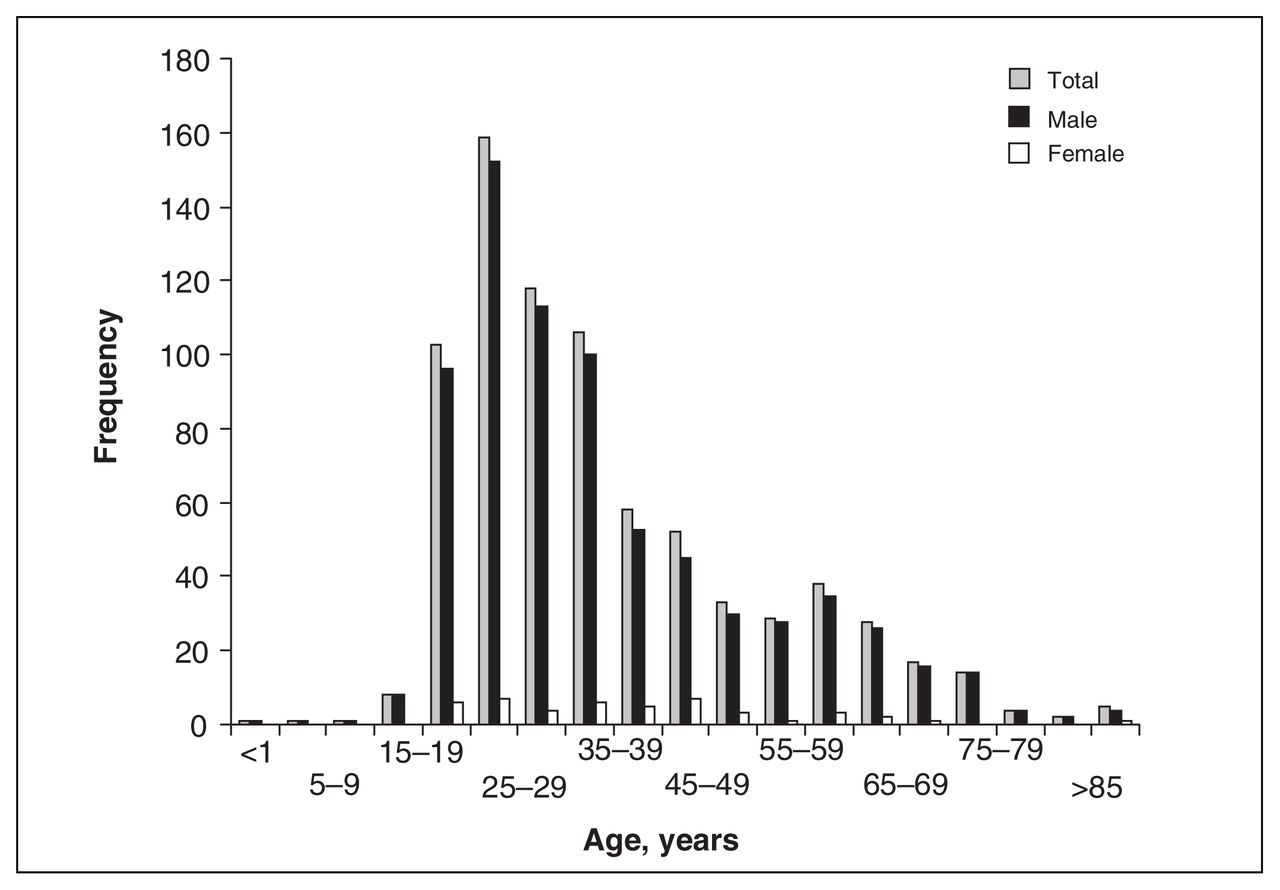
In the time frame of this study, significant firearm injuries were seen in 784 people. Over 94% of the injuries occurred in men (736/784). The largest proportion of the patient population comprised men aged 15–34 years (Fig. 1).

The age distribution for firearm injuries in Canada.
Patients evaluated in this study had a mean ISS of 26.1 (standard deviation [SD] 11.9), and the overall fatality rate was 39.8%. The average length of hospital stay was 17.7 (SD 35) days, and 39.1% of the patients received an operation at some point during their hospitalization. Blood alcohol, as measured on admission, was positive in 35% of patients.
Where firearm injuries occurred varied with age: with increased age, a higher percentage occurred at home. For persons aged 60 and older, for example, more than 70% of firearm injuries occurred at home and less than 10% on the street (Fig. 2). (Not included in Fig. 2 is the small percentage of patients who were also injured in areas defined as sports and industrial areas; these areas make up less than 3% of all locations.)
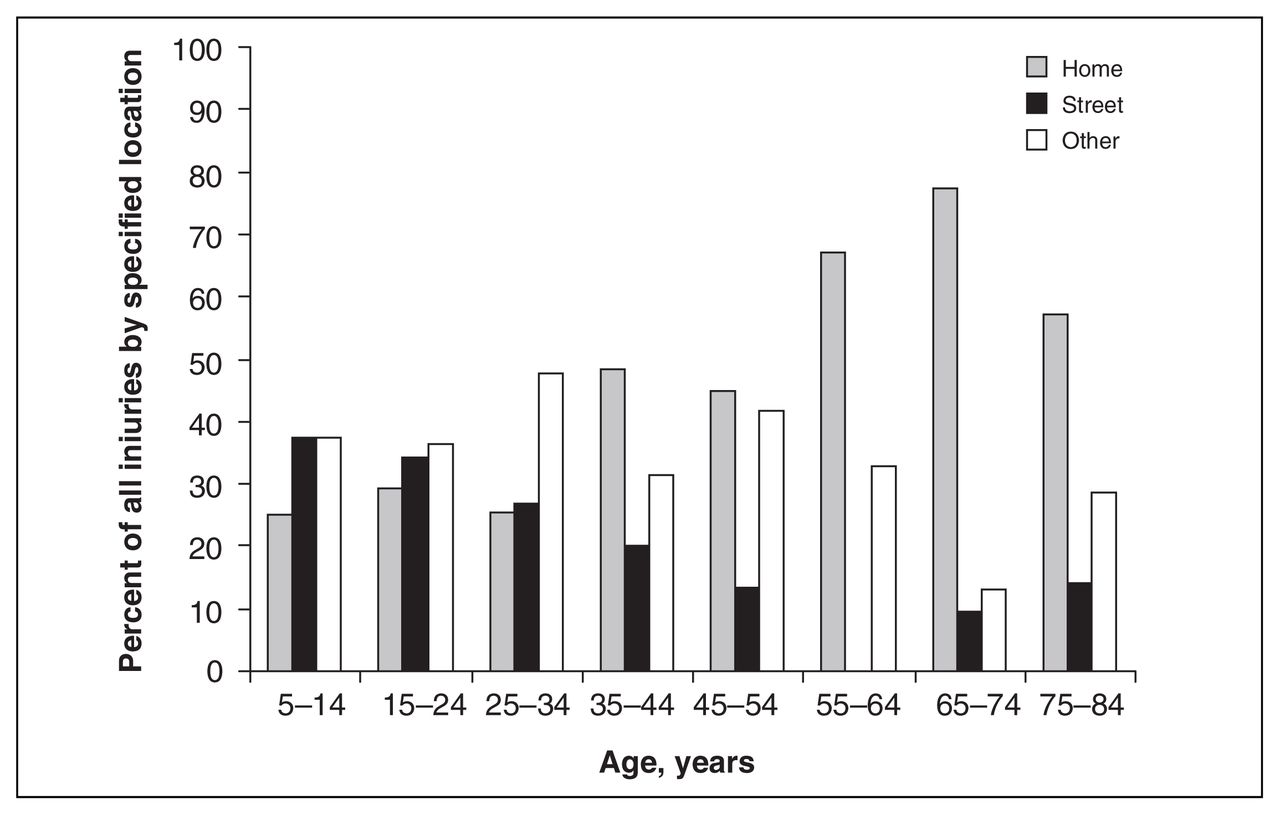
The percentage of all injured patients in each age range who are injured at home, in the street or in other or nonspecified locations.
The percentages of self-inflicted, assault, unintentional and unknown injuries were 27.8%, 60.3%, 6.1% and 5.7%, respectively. The percentage of self-inflicted gunshot wounds increased with age; the relative percentage of gun injuries from assaults decreased. For example, in the group aged 20 to 24 years, 80% of gun injuries were due to assaults. Conversely, 100% of gun injuries in the group aged 75 and older were self-inflicted (Fig. 3).

Percentages of self-inflicted and intentional injuries, compared by age group.
Most accidental and self-inflicted gun injuries were from long guns. By contrast, handguns were more likely to be used in firearm assaults (where the type of gun is unknown more than 50% of the time) (Fig. 4).

The percentage of all patients with a specific intention of injury and the weapon type used.
Of the fatalities, 83% occurred on the first day. Fatalities followed a binomial pattern, with most occurring early and a smaller number occurring late, after presumed multiorgan failure. Patients who survived were discharged to typical locations: home with or without support, rehabilitation, another acute hospital or “other.” Most patients went home (Fig. 5).
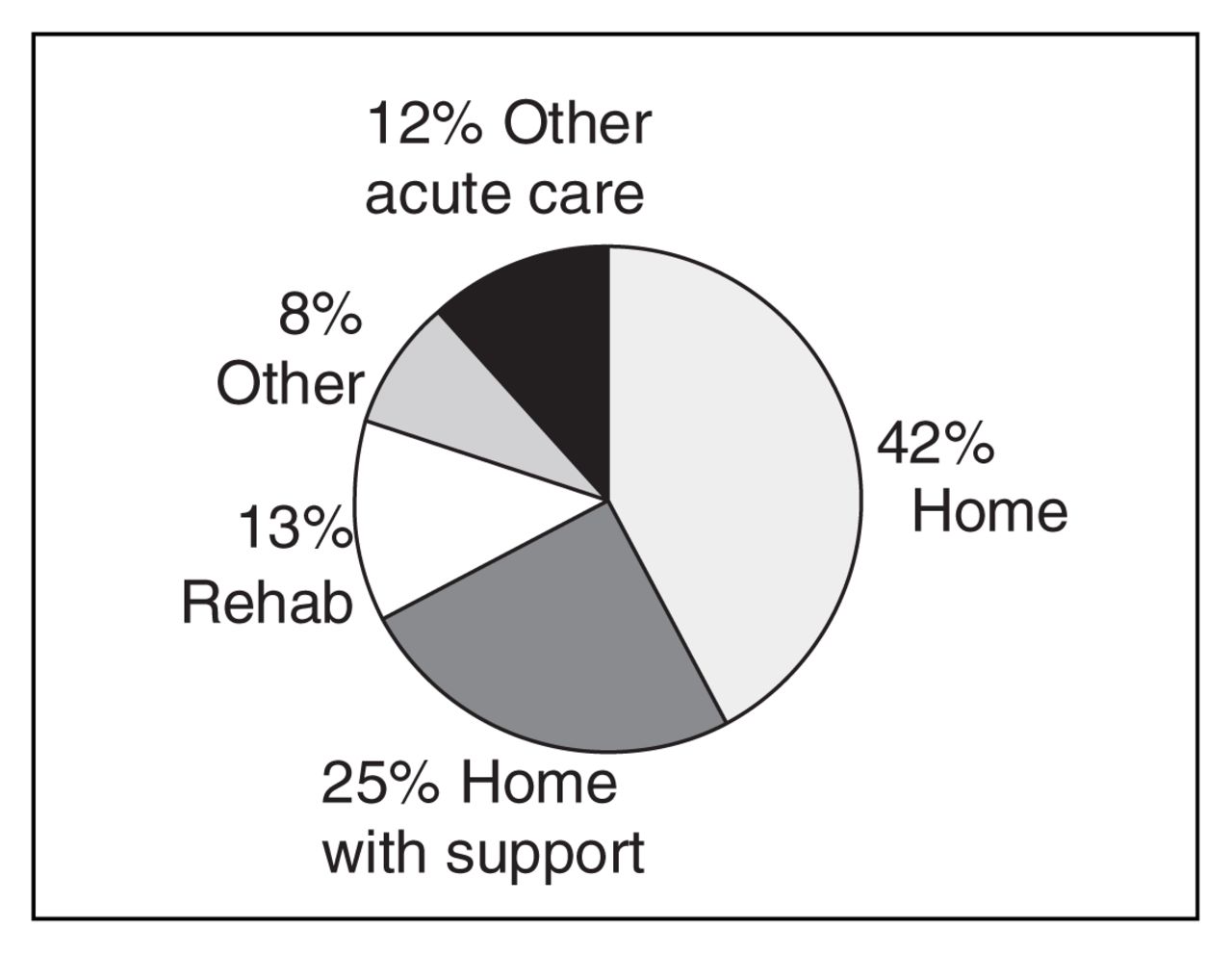
Discharge locations of surviving patients.
In the univariate logistic analyses of all patients admitted to hospital, ISS, the continuous variable for BP, BP less than 100, first GCS score, the continuous variable for age, age over 45 years, self-inflicted injury, intentional injury, police shooting, rural residence and whether the person was injured at home were all risk factors for death (Table 1). In the bivariate logistic regression (adjusting for ISS), all these variables except rural residence remained significant.
In the multiple logistic regression ISS, BP less than 100, first GCS score, sex, rural residence and self-inflicted injury remained significant risk factors for death (Table 2). We also expored interaction terms; these failed to reach significance.
Results of multivariate logistic regression for mortality for variables that reached 0.20 significance in univariate analysis*
Discussion
The demographic data in this study are consistent with the available literature for firearm fatalities, but they also provide some new and interesting insights. No other study has shown such a high rate of injury in male subjects. Male patients account for over 94% of those with firearm injuries, which is higher than the 87% observed in the United States.20 Most at risk is the group aged 20 to 24 years. Our results are similar to those found for fatal shootings in Canada and in the United States.20,21 However, the injury data differ from the mortality data in that most hospitalized patients had injuries due to assault, despite the fact that in Canada the number of firearm suicides is 5 times as great as the number of homicides.21 This result speaks to the lethality of suicide attempts and demonstrates that most individuals who attempt suicide with firearms don’t survive to reach hospital. As shown in this study, those who do are significantly more likely to die.
The case fatality rate in this study is 40%, higher than in US series, where the range is typically 30%–32%.14–16 This difference may be explained by the higher proportion of self-inflicted injuries in Canadian centres (28% v. 18%16), or it may be the result of lower volumes of penetrating trauma treated in Canada
It is interesting to note from the national registry data that older patients are more likely to have been shot at home with a self-inflicted injury. Almost 75% of patients over age 65 years were shot at home. It is not until their late 40s to early 50s that patients are more likely to have self-inflicted gunshot wounds than to be victims of firearm assault.
The weapon type used in each injury category is interesting yet intuitive. As Figure 4 reveals, self-inflicted and unintentional injuries were most often received from long guns. According to a 1998 study, long guns are the more prevalent weapon in Canada and were present in 19% of all households, whereas handguns were present in only 2.3% of households.22 Assaultive gun injuries are largely committed with handguns, perhaps the weapon of choice owing to the ease with which they are concealed.
At discharge, more than two-thirds of patients were discharged to their home, which speaks to the dichotomy that, if they survive this injury, patients usually go home. Perhaps the young average age of the patients allows them to rebound quickly from injury.
The vast majority of fatalities occurred in the first 24 hours after the shooting, indicating that, in addition to prevention, the most important window of opportunity for improved survival occurs immediately after injury, in the first “golden hour,” when the patient must be transported to an appropriate trauma centre.
The univariate unadjusted and adjusted analyses indicate that ISS is directly related to probability of death. Adjusted for ISS, the first BP, first GCS score, self-inflicted wounds, intentional wounds, injury at home, police shooting and age all significantly affect survival. This finding is not surprising, but certainly, the quantification of these variables’ effect is important. Clinically, having a low GCS score, being older and having a BP under 100 would intuitively suggest a worse outcome, when taken together; their respective adjusted odds ratios of death of 0.68, 1.99 and 4.12 per point increase emphasizes their importance.
Meanwhile, factors affecting the timely arrival of a patient to hospital are also important. Having self-inflicted wounds, injury at home as opposed to visibly on the street, or even the relatively beneficial effect of being shot by police, all affect the speed of arrival at the hospital. Whether because of a suicide attempt that goes unreported or because of delay in medical personnel entering the home, self-inflicted injuries and injuries at home have poorer outcomes. However, other factors contribute to a lower survival for those with self-inflicted gunshot wounds. These wounds are proportionally more likely than assaultive injuries to be to the head: 51% versus 14%, respectively. 16 This results in a case fatality rate for gunshot wounds to the head that is 3.3 times higher than the rate for gunshot wounds to other parts of the body.14
In the multivariate analysis, ISS is still significant, as are the following variables: BP under 100, first GCS score, sex, rural residence and self-inflicted injury. Self-inflicted wounds, even with adjusting for all the other variables in the model, are still significant, which may relate to the delay in assistance and transport to hospital. The significance of rural residence likely reflects the location bias of the urban trauma centres that recorded the data. Surviving patients from rural locations who are transported to a trauma centre likely are less seriously injured or more stable; those with more severe injuries are likely to die en route or are not transported at all. The most interesting finding is that male patients have a poor outcome in the multivariate model. With a preponderance of young men in this study, it may reflect young men’s likelihood to be involved in violent or crime-related activities, compared with women in the study, making them less likely to seek timely medical assistance.
It is important to stress that the data set represents only those patients surviving transportation to trauma centres involved in this study, which may limit its external validity.
Conclusions
Firearm injuries remain a significant concern in Canada. The financial and human cost is considerable. The predominance of young men injured intentionally with handguns in Canada offers a focus for firearms programs geared to high-risk individuals. The significant number of firearms deaths, largely in the first day, highlights the importance of preventative strategies and the need for rapid transport of patients to trauma centres for urgent care.
Important clinical factors such as initial BP, GCS, age and ISS offer significant predictors of mortality. In the case of self-inflicted wounds, our greatest effort should be preventive, promoting the availability of good mental health systems and continued restriction on access to firearms.
More attention must be directed toward education, policing and strategies to deal with the intentional injuries among our youth and young adults. We need to pay equal attention to those less visible older patients who are injuring themselves. Firearm violence in Canada is increasingly being acknowledged nationally and demands a multidisciplinary approach.
Footnotes
Competing interests: None declared.
Contributors: Drs. Finley, Brown, Simons and Hameed designed the study. Dr. Finley acquired the data, which Drs. Finley, Hemenway and Clifton analyzed. Dr. Finley wrote the article. All authors reviewed the article and gave final approval for its publication.
- Accepted January 10, 2007.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.