


Abstract
Background: A loss of reduction due to inadequate support of the anterior column when using short-segment instrumentation to treat burst fracture and novel methods for support of the anterior column through a posterior approach to augment posterior instrumentation have been reported in the literature. We hypothesized that if anterior column support is an important adjunct to posterior short-segment instrumentation, then avoidance of axial load until sufficient anterior column healing occurs, allowing load-sharing with the implant, would improve spinal alignment at follow-up.
Methods: We conducted a retrospective cohort study in which consecutive patients who had instrumentation and fusion with the AO spinal fixator were immediately ambulated after surgery or had 4 weeks of bedrest. We measured kyphosis and wedge angles preoperatively, immediately postoperatively and at the time of final follow-up. We used radiologic measures to assess instrumentation and bone failure.
Results: We found significant differences in the mean loss of wedge and kyphosis angle correction between patients immediately ambulated and those who had 4 weeks of bedrest (0.71º v. − 4.73º for wedge and 1.81º v. − 6.55º for kyphosis, respectively). There was significant correlation between instrumentation and bone failure in both the immediate ambulation and bedrest groups.
Conclusion: Bedrest improves the maintenance of intraoperative sagittal alignment correction, which is in agreement with the theory that inadequate support of the anterior spinal column is the mechanism for loss of reduction when using short-segment instrumentation to treat burst fractures. Therefore, addressing the anterior column directly through anterior surgery or by employing novel techniques in posterior surgery is recommended if one of the goals of treatment is to maintain the sagittal correction achieved at the time of surgery. Trying to achieve this goal by addressing posterior implant design or bone quality alone will not be successful because instrumentation and bone failure occur together.
Burst fractures comprise about 15% of all thoracolumbar spinal injuries.1–4 Treatment options include nonoperative management, posterior surgery, anterior surgery and combined anterior and posterior surgery, and there is much controversy over the optimal method of management.5
Nonoperative management, through a period of recumbency and/or the use of hyperextension casting or bracing, avoids the morbidity associated with surgical intervention, and its supporters cite acceptable functional results, particularly in patients with burst fractures who are neurologically intact on presentation.6–10 Alternatively, the advantages of surgery include a shorter period of bedrest and hospital admission, better correction of kyphotic deformity and the avoidance of late neurologic deterioration due to instability.2,3,11–13
Earlier literature on surgical treatment supported the use of posterior instrumentation, citing excellent results with respect to spinal stability, postoperative neurologic improvement, anatomic alignment and low patient morbidity.14–17 Short-segment instrumentation such as the AO internal spinal fixator (Synthes) was considered to be more favourable than traditional Harrington rod posterior instrumentation and its modifications because short-segment instrumentation allowed stable fixation and reduction across all 3 columns and was limited only to adjacent spinal segments.14 Supporters of short-segment internal fixators have reported favourable results.1,4,18,19
In more recent literature, detractors of a purely posterior approach have reported a loss of reduction due to inadequate support of the anterior spinal column.20–23 The pedicle screw-based implants have failed owing to loosening, bending or fracturing, resulting in a mean loss of kyphosis correction ranging from 9° to 11° in the reported pedicle screw studies.24–29 This has led to proponents for anterior strut grafting and instrumentation to treat burst fractures.30–33
Most recently, there have been reports of novel methods for support of the anterior column through a posterior approach to augment posterior short-segment instrumentation. Cho and colleagues34 have reported on the use of polymethylmethacrylate (PMMA) vertebroplasty, Acosta and colleagues35 on the use of PMMA kyphoplasty, Verlaan and colleagues36 on the use of calcuim phospate cement kyphoplasty and Li and colleagues37 on the use of a titanium transpedicle body augmenter.
We sought to go back a step and demonstrate that the mechanism for loss of alignment correction in patients with burst fractures treated with short-segment posterior instrumentation was due to inadequate support of the anterior column. We hypothesized that if anterior column support is an important adjunct to posterior short-segment instrumentation in maintaining the sagittal correction achieved at the time of surgery, then avoidance of axial load until sufficient anterior column healing occurs, allowing load-sharing with the implant, would improve spinal alignment at follow-up. We tested this hypothesis by comparing maintenance of correction among patients with posterior instrumentation who were immediately ambulated after surgery to that among patients who had bedrest for the first 4 weeks after surgery to offload the spine.
Methods
We retrospectively reviewed the medical records and radiographs of patients with burst fractures treated with posterior short-segment instrumentation and fusion by one of us (D.Y.) at our tertiary-care centre from October 1991 to June 2003. All patients underwent computed tomography (CT) scanning to confirm the diagnosis of a burst fracture as defined by Denis and colleagues.12 Additional inclusion criteria were vertebral height loss greater than 50% or kyphosis greater than 20°, no neurologic deficit that would interfere with walking, no medical illnesses that would preclude operative intervention, no pre-existing diagnosis or active treatment for osteoporosis and sufficient pedicle size for posterior instrumentation. We obtained hospital ethics approval as a quality assurance review.
The treatment for all patients in both groups was posterior short-segment instrumentation with the AO spinal fixator and posterolateral fusion using autologous bone graft from the iliac crest, as previously described by Dick.16 In keeping with the early reports of maintaining deformity correction through posterior short-segment instrumentation and fusion, we ambulated the initial cohort of patients immediately after surgery. Later, when reports of loss of correction began appearing in the literature, treatment changed to include an initial period of 4 weeks of bedrest to allow strengthening of the anterior column before axial loading. Patients in the bedrest group were allowed bathroom privileges and they were allowed to have the head of the bed raised up to 90°. They received deep vein thrombosis prophylaxis. All patients in both groups wore a spinal orthosis while ambulating for the first 3 months after their injuries.
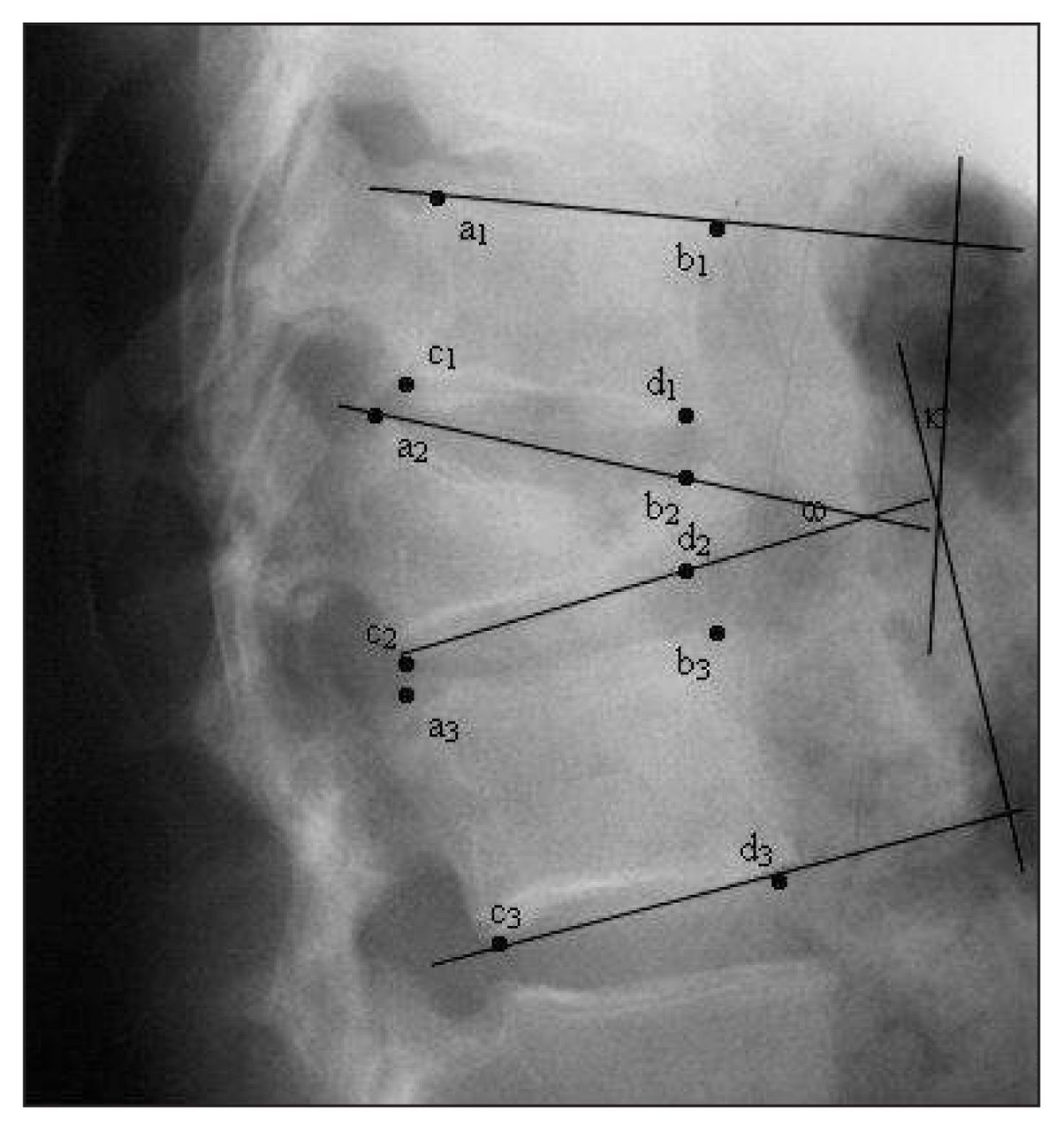
We took radiographic measurements at 3 points during patient care: on admission, immediately after surgery and at final out-patient follow-up. We obtained the postoperative radiographs for patients in both cohorts using the same technique. We obtained the anteroposterior radiograph while patients were supine, and the lateral radiograph while the patients were in the lateral decubitus position. We measured kyphosis and wedge angles according to the method described by Denis and colleagues38 (Fig. 1). Two observers measured all the radiographic parameters while blinded to the treatment groups, with differences settled by consensus.
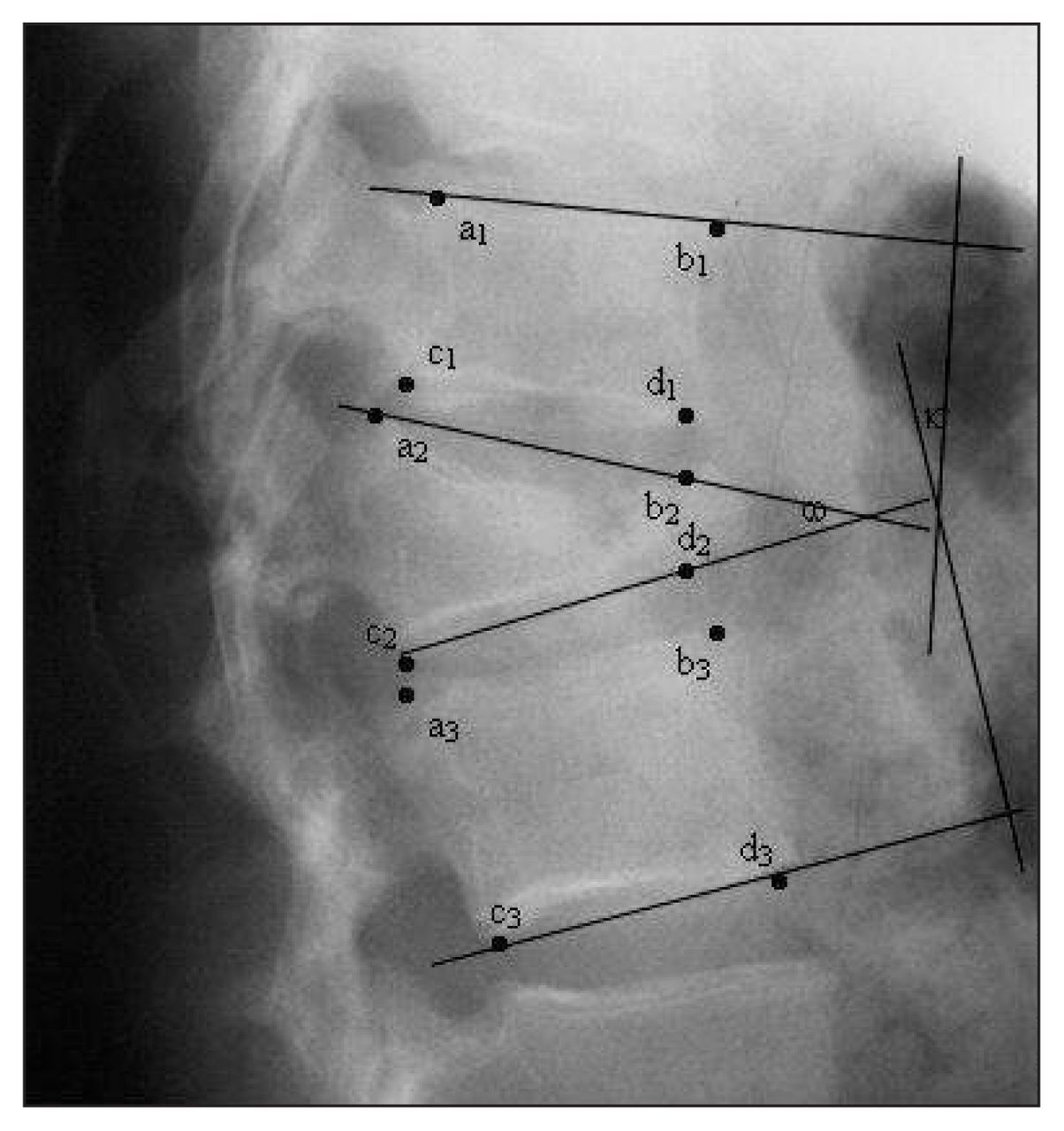
Kyphosis angle κ between a1b1 and c3d3, reflecting the contribution of both bony collapse and disc damage to angular deformity. Wedge angle ω between a2b2 and c2d2, reflecting solely the degree of bony collapse.
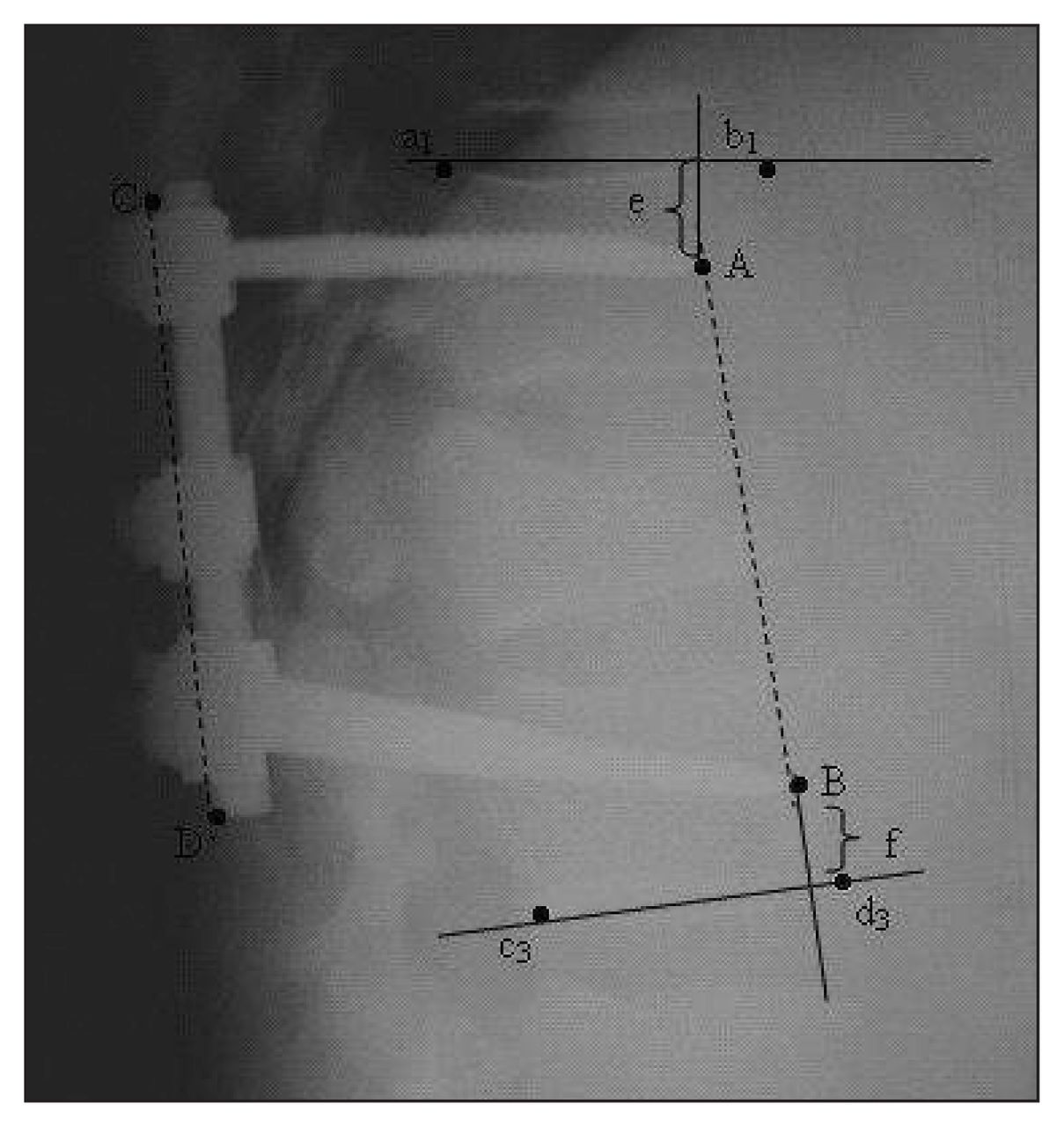
There were no instances of broken screws. Therefore, to assess the contribution to the loss of kyphotic correction by implant bending (instrument failure) and screw migration (bone failure), we measured interscrew-to-rod ratios and screw-end plate–to-rod ratios (Fig. 2).
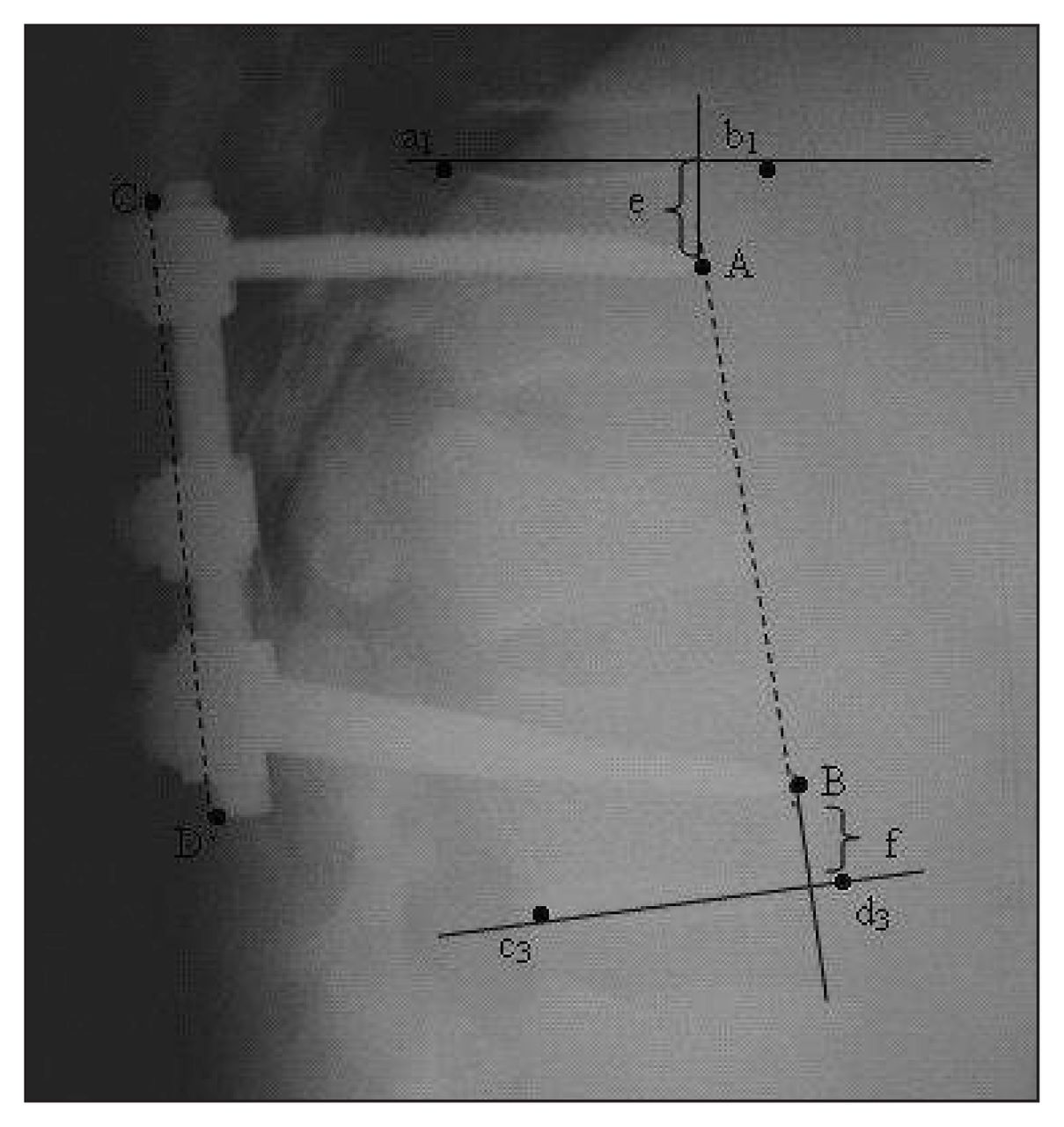
Interscrew-to-rod ratio, AB/c3d3, as a measure of instrument failure. Screw-end plate-to-rod ratio, (e + f)/c3d3, as a measure of bone failure, where e and f are the distances from screw tips A and B to the superior and inferior end plates, respectively.
Statistical analysis
We entered the data into an Excel spreadsheet, and we used SPSS version 12.0.1 (SPSS Inc.) for our analysis. After descriptive analysis (frequencies, means, standard deviations), we assessed the data for normality of distribution using histograms and box plots. We used independent samples t tests to analyze the alignment data collected in the bedrest versus the ambulation groups. We used Pearson correlation to analyze the relation between bend and migration.
Results
We reviewed the medical records and radiographs of 36 patients with burst fractures treated with posterior short-segment instrumentation, as confirmed on CT scans, from October 1991 to June 2003. Of these, 4 patients were lost to follow-up (3 owing to relocation and 1 owing to death from unrelated causes) before the final follow-up could be performed, which left 32 patients for inclusion in our study.
An initial 19 patients treated between October 1991 and September 1997 formed the immediate ambulation group, and 11 patients treated between October 1997 and June 2003 formed the bedrest group. Two patients, presenting in August 1998 and June 2001, respectively, requested immediate ambulation and thus were included in that group, bringing its number of participants to 21.
The immediate ambulation group comprised 16 men and 5 women with a mean age of 45 (range 17–76) years. There were 2 patients older than 70 years. Excluding these patients reduced the mean age of the group to 42 years. The mean follow-up was 18 (range 1–117) months. The location of the fractures were the T12 vertebra in 5 patients, L1 in 8, L2 in 6, L3 in 1 and L4 in 1. The mechanism of injury was motor vehicle collision in 7 patients, a fall from a height in 12, a direct blow from an object in 1 and no known trauma in 1.
The bedrest group comprised 7 men and 4 women with a mean age of 42 (range 19–58) years. The mean follow-up was 16 (range 3–79) months. The location of the fractures were the T12 vertebra in 1 patient, L1 in 3, L2 in 4, L3 in 1 and L4 in 2. The mechanism of injury was motor vehicle collision in 6 patients, a fall from a height in 4 and a direct blow from a heavy object in 1.
Preoperative, postoperative and follow-up wedge angles and kyphosis angles were normally distributed, permitting the use of parametric statistics. The mean results for both groups are listed in Table 1. The change from the pre-operative to the follow-up period was also normally distributed for both angles. There was no difference in the mean postoperative wedge angle between the immediate ambulation and bedrest groups (10.29° v. 11.27°, t = − 0.14, p = 0.66). However, the mean change in wedge angle at final follow-up compared with preoperative angles was statistically significant at 0.71° in the immediate ambulation group and − 4.73° in the bedrest group (t = 2.56, p = 0.016).
Preoperative, immediately postoperative and follow-up measurements of 32 patients with burst fractures, by treatment group
The difference in the mean postoperative kyphosis angle between the immediate ambulation and bedrest groups approached significance at 4.24° and − 3.18°, respectively (t = 1.75, p = 0.09). However, the mean change in kyphosis angle at final follow-up compared with pre-operative angles was 1.81° in the immediate ambulation group and − 6.55° in the bedrest group (t = 2.59, p = 0.015).
We recognized that the follow-up was short in 3 patients (1 month in 2 patients and 2 months in another), therefore, we repeated our analysis excluding the data on these patients. Significance levels were similar despite the loss of power associated with the reduction in sample size: significance levels changed to p = 0.017 from p = 0.016 for the wedge angle and from p = 0.015 to p = 0.012 for the kyphosis angle, remaining statistically significant for both values.
Migration and bend were normally distributed, allowing the use of the parametric Pearson correlation to assess the association between the 2 measures. They were significant and positively correlated at r = 0.498 (p = 0.005).
There were no decubitus ulcers, thromboemboli or other complications related to bedrest.
Discussion
There were no differences in the mean postoperative wedge and kyphosis angles between the immediate ambulation and bedrest groups. However, in the former group, there was a failure to maintain the correction of sagittal alignment achieved intraoperatively, and there was a further loss of 0.71° of wedge angle and 1.81° of kyphosis angle at follow-up compared with the preoperative measurements. This is consistent with reports in the literature indicating that posterior short-segment instrumentation alone is insufficient in maintaining anatomic correction, with loss of kyphotic correction by the loosening, bending and fracturing of pedicle screw–based implants.20,23,30,32
Sasso and colleagues17 noted that in patients who experience substantial compression of the anterior vertebral body, the disrupted anterior column lacks structural integrity and places significant bending loads on the implant. We hypothesized that avoidance of axial load until sufficient vertebral body healing occurs, providing anterior column support and allowing load-sharing with posterior short-segment instrumentation, would improve the maintenance of the intraoperative reduction. The significant difference that we observed between the ability of the immediate ambulation and bedrest groups to maintain the sagittal alignment correction obtained intraoperatively, with the bedrest cohort having a wedge angle that was 4.73° better at follow-up than preoperatively, supports the findings of Sasso and colleagues and our hypothesis.
Loss of reduction due to disc collapse has been reported by Lindsey and Dick26 and Speth and colleagues;27 the loss of reduction occurs because the intervertebral disc material is redistributed into the fractured vertebral body.39,40 This is important because it can contribute to the local kyphosis. As a result, we measured the kyphosis angle, which includes the vertebral body and the adjacent discs. There was a significant difference between the bedrest and immediate ambulation groups, with the former having a kyphosis angle that was 6.55° better at follow-up than preoperatively. We hypothesize that the period of bedrest allowed sufficient healing of the vertebral body to prevent redistribution of disc material with subsequent disc collapse, accounting for our finding.
We found that in the immediate ambulation and bed-rest groups, there was loss of correction due to screw migration and bending of the instrumentation. Analysis demonstrated a positive correlation between migration and bend. This means that in patients with loss of correction, migration and bend occurred together. Therefore, the loss of reduction in posterior short-segment instrumentation is not due to implant or bone quality in isolation. This explains the finding of Alvine and colleagues22 that, despite progressive improvement in flexion bending endurance of the pedicle screws, there was still loss of sagittal alignment in follow-up when using variable screw plate instrumentation to treat burst fractures.
There were no complications due to bedrest, but we recognize the advantages of early ambulation and shortened hospital admission as well as our small sample size. Therefore, we present this study not to promote bedrest, but rather to demonstrate that the loss of alignment correction in patients with burst fractures treated with short-segment posterior instrumentation is due to inadequate support of the anterior column. Addressing inadequate support through novel techniques34–37 is an important adjunct to posterior implants in maintaining the sagittal correction achieved at the time of surgery.
Our study has limitations. Acquiring follow-up data on patients in a transitional population is difficult, and 4 of 36 patients (11%) were lost to follow-up. In addition, the change in practice over time to produce the 2 cohorts introduced a potential learning curve bias. This may have caused better results in the bedrest group, which was treated later. However, during this later time period, 2 patients requested immediate ambulation. One of these patients had better wedge (by 1º) and kyphosis (by 7º) angles at follow-up compared with preoperative measures. The other had worse wedge (by 6º) and kyphosis (by 5º) angles at follow-up compared with preoperative measures.
Our aim was to study the importance of the anterior column to the mechanism of failure of short segment instrumentation, not patient satisfaction or function with the use of bedrest. Therefore, we gathered radiologic parameters rather than long-term patient questionnaire data. Although our follow-up was relatively short, we believe our results are valid because radiographic analysis would define early on whether avoidance of axial load until sufficient vertebral healing occured would improve sagittal alignment at follow-up.
Conclusion
Bedrest improves the maintenance of intraoperative sagittal alignment correction, consistent with the theory that inadequate support of the anterior spinal column is the mechanism for loss of reduction when using posterior short-segment instrumentation to treat burst fractures. Addressing the anterior column directly through anterior surgery or novel techniques in posterior surgery is recommended if one of the goals of treatment is to maintain the sagittal correction achieved at the time of surgery. Trying to achieve this goal by addressing posterior implant design or bone quality alone will not be successful because instrumentation and bone failure occur together.
Footnotes
Presented in part at the annual meeting of the Canadian Spine Society, Mar. 22–24, 2001, Mont Tremblant, Que.
Competing interests: None declared.
Contributors: Drs. Dang and Yen designed the study. Dr. Yen acquired the data, which Dr. Dang and Ms. Hopman analyzed. All authors wrote and reviewed the article and gave final approval for its publication.
- Accepted February 2, 2008.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.