


Abstract
Background: Previous reviews of the effectiveness of antibiotic prophylaxis for elective inguinal hernia repair were not conclusive owing to the limited number of patients enrolled in randomized controlled trials (RCTs). However, since new RCTs involving patients undergoing tention-free hernioplasty have been published in recent years, we performed a new meta-analysis to evaluate the effectiveness of antibiotic prophylaxis in the prevention of postoperative complications after this procedure.
Methods: We performed a meta-analysis of RCTs studying the use of antibiotic prophylaxis to prevent postoperative complications in patients undergoing tension-free hernioplasty.
Results: We included 6 RCTs conducted around the world in our analysis. Compared with the control condition, antibiotic prophylaxis was associated with a lower incidence of incision infection (odds ratio [OR] 0.45, 95% confidence interval [CI] 0.26–0.77, p = 0.004). There were no significant differences in risk for incision hematoma (OR 1.57, 95% CI 0.60–4.10, p = 0.35), respiratory infection (OR 1.00, 95% CI 0.17–5.79, p > 0.99) or urinary tract infection (OR 1.81, 95% CI 0.38–8.52, p = 0.45) between the 2 conditions.
Conclusion: Antibiotic prophylaxis use in patients undergoing tension-free hernioplasty decreases the rate of incision infection by 55%.
Tension-free hernioplasty is rapidly becoming the most popular technique for repairing inguinal hernias.1–6 More than 80% of abdominal wall hernias occur in the groin, and most are repaired with prosthetic mesh. Incision infection is the most frequent complication in tension-free hernioplasty.7 Some studies have identified risk factors for incision infection: sex (greater risk among women), age (> 70 yr), comorbidity, duration of surgery, and routine use of drainage and prostheses.8–11 Incision infection is associated with a longer length of stay in hospital, increased costs and a decrease in quality of life.12,13
It remains uncertain whether antibiotic prophylaxis is indicated to prevent postoperative incision infection after mesh repair of inguinal hernias. The incidence of infection after inguinal hernia repair has been reported to vary from 0% to 9%.14 When a foreign body, such as a polypropylene mesh, is used, prevention of an incision infection is more important. A 2004 Cochrane review15 concluded that antibiotic prophylaxis for elective inguinal hernia repair could not be firmly recommended or discarded because the number of patients in randomized controlled trials (RCTs) was limited. However, new RCTs involving patients having tension-free hernioplasty have been published in recent years, increasing the number of patients evaluated. We conducted a new meta-analysis to assess the effectiveness of antibiotic prophylaxis in preventing postoperative complications after tension-free hernioplasty.
Methods
Study selection
We searched different databases, including the Cochrane Central Register of Controlled Trials (January 1966 to May 2010), MEDLINE (January 1966 to May 2010), EMBASE (January 1966 to May 2010) and the China Biological Medicine Database (January 1978 to May 2010), using the terms “hernia” and “antibiotic prophylaxis.” We manually searched the reference lists of pertinent articles to identify any additional studies relevant to our analysis. Two independent investigators reviewed all articles yielded by our search against the following selection criteria. Included studies must have been prospective RCTs involving patients aged 18 years or older who were scheduled to undergo tension-free hernioplasty. The studies must have included a control group (placebo or no antibiotic) of adults without contraindications for antibiotic use and without immunosuppression caused by diseases or medications. We excluded quasirandomized trials and nonrandomized studies. We also excluded studies that compared groups receiving different types of antibiotics rather than 1 type of antibiotic and a control group. Finally, if our search yielded more than 1 version of the same study, only the most recent version was included.
The studies were independently evaluated by 2 of us (K.-X.S., H.-G.L.) on the basis of 4 outcomes — 1 primary outcome (incision infection) and 3 secondary outcomes (incision hematoma, respiratory infection and urinary tract infection). Discrepancies in the evaluation of some studies were resolved through discussion between the reviewers.
Assessment of study quality
The quality of included reports was scored using the Jadad composite scale,16 which assesses descriptions of randomization, blinding and dropouts (withdrawals). The quality scale ranges from 0 to 5 points, with a low-quality report receiving a score of 2 or less and a high-quality report receiving a score of at least 3.
Statistical analysis
We performed statistical analyses using Review Manager software from the Cochrane Collaboration, and odds ratios (ORs) were calculated for each outcome using a Mantel–Haenszel fixed-effects model. The number needed to treat was calculated from the ORs and the background risk of incision infection in patients in the control group. We also performed a sensitivity analysis adjusted by study quality. Heterogeneity was assessed with the Q test (results were considered to be significant at p < 0.05), and the influence of heterogeneity on OR value was determined using an I2 test.17
Results
Primary outcome
We considered incision infection as the primary outcome. Of the 124 studies yielded in our search, 6 RCTs exclusively evaluated tension-free hernioplasty and met our inclusion criteria.18–23 The characteristics and quality of each selected study are shown in Table 1. The studies were homogeneous in terms of clinical and methodologic criteria. The RCTs selected included a total of 2235 patients: 1119 in the antibiotic group and 1116 in the control group (Table 2). The incision infection rate was 19 of 1119 (1.70%) patients in the antibiotic group and 42 of 1116 (3.76%) in the control group. The OR was 0.45 (95% confidence interval [CI] 0.26–0.77, p = 0.004), resulting in a number needed to treat of 48. Statistical heterogeneity was not identified (Q test for heterogeneity, p = 0.27; Fig. 1). A sensitivity analysis by quality, excluding the study by Celdran and colleagues21 owing to its early conclusion and small sample, revealed an overall OR of 0.49 (95% CI 0.28–0.85, p = 0.010; Fig. 2).

Effect of antibiotic prophylaxis on incision infection in patients who have had tension-free hernioplasty. CI = confidence interval.
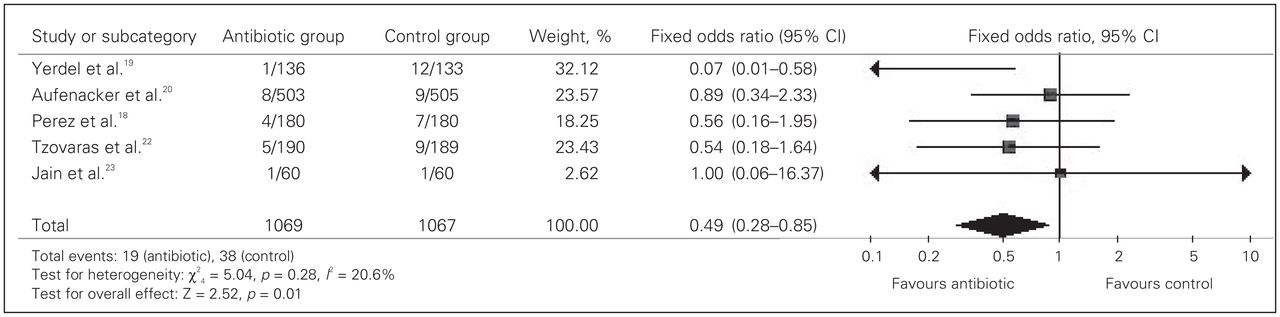
Sensitivity analysis by quality, excluding the study by Celdran and colleagues.21 CI = confidence interval.
Study characteristics and quality evaluation of each selected study on the use of antibiotic prophylaxis to prevent postoperative complications in patients undergoing tension-free hernioplasty
Patient and outcome data
Secondary outcome
Incision hematoma, respiratory infection and urinary tract infection were considered as secondary outcomes. For incision hematoma, data were extracted from 3 RCTs.18,19,23 These trials included a total of 749 patients, 18 of whom had an incision hematoma. Among these patients, 11 were in the antibiotic prophylaxis group and 7 patients were in the control group, indicating that antibiotic prophylaxis did not reduce the incidence of incision hematoma compared with the control condition (OR 1.57, 95% CI 0.60–4.10, p = 0.35; Fig. 3).

Effect of antibiotic prophylaxis on secondary outcomes in patients who had tension-free hernioplasty. CI = confidence interval.
For respiratory infection, data were extracted from 2 RCTs.20,22 These trials included a total of 749 patients, 4 of whom had a respiratory infection. Among these patients, 2 were in the antibiotic prophylaxis group and 2 were in the control group, indicating that antibiotic prophylaxis did not reduce the incidence of respiratory infection compared with the control condition (OR 1.00, 95% CI 0.17–5.79, p > 0.99; Fig. 3).
For urinary tract infection, data were extracted from 2 RCTs.20,22 These trials included a total of 1387 patients, 6 of whom had a urinary tract infection. Among these patients, 4 were in the antibiotic prophylaxis group and 2 were in the control group, indicating that antibiotic pro-phylaxis did not reduce the incidence of urinary tract infection compared with the control condition (OR 1.81, 95% CI 0.38–8.52, p = 0.45; Fig. 3).
Discussion
It is well documented that antibiotic prophylactic coverage of most “clean-contaminated” surgical procedures can significantly prevent infectious complications, including incision infection, thereby affecting the overall rate of death and complications.24 There is also no doubt that antibiotic prophylaxis is needed in selected “clean” surgical procedures where a prosthesis is implanted, because the consequences of a graft infection can be severe or even fatal.25,26 Hip or knee arthroplasties25 and cardiac or vascular graft implants26 are “clean” procedures in which peri-operative antibiotic coverage has been shown to be beneficial and is clearly indicated. However, the benefit of antibiotic prophylaxis in other “clean” surgical procedures, such as tension-free hernioplasty, has been considered questionable. A previous meta-analysis by Sanchez-Manuel and Seco-Gil15 reported no statistical difference in incision infection rates between antibiotic and control groups. However, a subgroup analysis suggested that a protective effect may have existed in tension-free hernioplasty but was undetectable owing to the small sample size.
Incision infection rates in inguinal hernia repair vary from 0% to 9%, with a mean value around 4%. To perform an RCT with enough power to detect a 55% decrease in incision infection rates, it is necessary to include about 1700–3000 patients, depending on the sample size formula used and the base rate of incision infection. Larger samples would be needed to detect larger decreases. To perform such an ideal study would be difficult. However, a meta-analysis is a design that allows merging results of small RCTs, increasing the possibility of detecting an intervention effect. Antibiotic prophylaxis in tension-free hernioplasty is an example of an intervention where meta-analysis could help to detect a beneficial effect.
Results from the present meta-analysis showed a 55% protective effect of antibiotic prophylaxis on decreasing the incision infection rate in patients undergoing tension-free hernioplasty and favoured the routine use of antibiotic prophylaxis in these patients. Neither clinical nor statistical differences were found among included studies, which makes our results stronger and generalizable. However, we found no significant differences in the rates of incision hematoma, respiratory infection or urinary tract infection between the antibiotic prophylaxis and control groups. The antibiotic was administered 30 minutes before the operation, and the half-life of the antibiotic was short; however, most respiratory and urinary tract infections were diagnosed after hospital discharge, so the antibiotic could not have prevented those infections.
Conclusion
The argument about the clinical use of antibiotic prophylaxis is still open. It must be specifically determined if antibiotic prophylaxis must be administered in all patients or if there are some risk factors that could help to select the best candidates. The studies included in our analysis only assessed low-risk patients, so conclusions can be generalized only to such patients. However, as can be seen in Figure 1, studies with higher rates of incision infection showed a stronger positive response to antibiotic prophylaxis use, and these findings suggest that improvement is greater in these clinical settings. In many other studies, the incision infection rate is exceedingly low. Therefore, surgeons and hospitals must assess their own incision infection rates to define if antibiotic prophylaxis should be used widely. For clinical settings with low rates of incision infection, selective use of antibiotic prophylaxis based on patients’ basal risk factors could be a better therapeutic strategy. Nonetheless, this strategy can only be probed with a specifically designed study.
Another subject that must be assessed in antibiotic prophylaxis is cost-effectiveness. As can be seen, incision infection rates could be as low as 1% in some centres. In these cases, the costs of antibiotic administration must be carefully evaluated against the potential benefits. Only studies particularly designed to answer this question could solve it.
Footnotes
Competing interests: None declared.
Contributors: J.-F. Li, D.-D. Lai and X.-D. Zhang designed the study, acquired the data and wrote the article. K.-X. Sun and H.-G. Luo analysed the data. J.-F. Li, D.-D. Lai, A.-M. Zhang, K.-X. Sun, H.-G. Luo and Z. Yu reviewed the article. All authors approved its publication.
- Accepted July 16, 2010.
References

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.