


Abstract
Background: The increasing incidence of hip fractures in our aging population challenges orthopedic surgeons and hospital administrators to effectively care for these patients. Many patients present to regional hospitals and are transferred to tertiary care centres for surgical management, resulting in long delays to surgery. Providing timely care may improve outcomes, as delay carries an increased risk of morbidity and mortality.
Methods: We retrospectively reviewed the cases of all patients with hip fractures treated in a single Level 1 trauma centre in Canada between 2005 and 2012. We compared quality indicators and outcomes between patients transferred from a peripheral hospital and those directly admitted to the trauma centre.
Results: Of the 1191 patients retrospectively reviewed, 890 met our inclusion criteria: 175 who were transferred and 715 admitted directly to the trauma centre. Transfer patients’ median delay from admission to operation was 93 hours, whereas nontransfer patients waited 44 hours (p < 0.001). The delay predominantly occurred before transfer, as the patients had to wait for a bed to become available at the trauma centre. The median length of stay in hospital was 20 days for transfer patients compared with 13 days for nontransfer patients (p < 0.001). Regional policy changes enacted in 2011 decreased the median transfer delay from regional hospital to tertiary care centre from 47 to 27 hours (p = 0.005).
Conclusion: Policy changes can have a significant impact on patient care. Prioritizing patients and expediting transfer will decrease overall mortality, reduce hospital stay and reduce the cost of hip fracture care.
Hip fractures are among the most common orthopedic injuries requiring hospital admission. As the incidence of hip fractures increases, surgeons and administrators are increasingly challenged to provide care for these patients effectively and efficiently. Providing timely care may substantially improve patients’ outcomes, as delay carries an increased risk of morbidity and mortality. Increased mortality, postoperative infections and length of hospital stay have all been correlated with surgical delay.1–7
Tertiary care trauma centres are often responsible for the care of injured patients referred from regional hospitals in the surrounding area. Many hospitals may lack the resources required to provide the necessary surgical services or to care for patients with severe comorbidities. As a result, a proportion of patients require transfer to a tertiary care centre for surgical management. Transfer patients may have longer delays to surgery than patients admitted directly to a tertiary care centre.
Population size and vast geographic area create many challenges in providing timely care for patients with hip fractures. Considering tertiary care centres manage acute life-threatening injuries, patients with hip fractures are generally considered a lower priority, and patients are transferred on a nonurgent basis. In April 2011, a regional hip fracture protocol was established in southwestern Ontario. This protocol was designed to facilitate timely surgery for patients with hip fractures, with a goal of providing surgical care for 90% of patients within 48 hours of their admission to a centre with the capacity to provide surgical care. Concurrently, the priority for patients with hip fractures to be transferred from a nonsurgical to a surgical centre was increased.
The purpose of the present study was to retrospectively compare patients transferred to a tertiary care centre with those admitted directly. Primary outcomes were surgical delay, length of hospital stay (LOS) and the effect of regional policy changes on wait times.
Methods
We retrospectively reviewed the cases of all patients with proximal femur fractures treated in a tertiary care, Level 1 trauma centre between 2005 and 2012. All patients with isolated femoral neck, intertrochanteric and subtrochanteric fractures were eligible for inclusion in this analysis. The study was approved by our institution’s review board.
Patient information was obtained from our institution’s electronic patient database, Powerchart (Cerner Corporation). This database also allowed us to follow patients upon repatriation to home hospital. The patient information recorded included sex; age; American Society of Anesthesiologist (ASA) score; duration of surgery; inhospital mortality; blood transfusion requirement; and incidence of deep venous thrombosis, pulmonary embolism, pneumonia, urinary tract infections (UTIs) and myocardial infarctions. We also documented the precise time and date of admission to referring centre, admission to tertiary care centre, start and end of operation, discharge from tertiary care centre and ultimate discharge from referring centre.
Our exclusion criteria were age younger than 60 years, pathologic or pending pathologic fracture, revision surgery, polytrauma, unrelated hemorrhagic complication, admission to hospital for diagnosis different than hip fracture, intraoperative complications, fracture diagnosis missed for longer than 1 week, electronic charts with inadequate documentation, and long-term anticoagulation or documented hematologic disease.
Statistical analysis
Statistical analysis was performed using χ2 and Fisher exact tests to compare transfer and nontransfer patients.
Results
Of the 1191 patients retrospectively reviewed, 890 satisfied our inclusion criteria. We excluded 31 polytrauma patients, 114 receiving long-term anticoagulation therapy, 17 with unrelated hemorrhagic complications, 38 admitted to hospital for a different diagnosis, 44 with pathologic fractures, 27 who underwent revision surgery, 10 who experienced intraoperative complications, 12 with inadequate documentation and 8 with missed fractures. There were no differences in age, sex, fracture type, fixation method, duration of surgery and ASA score between the transfer and nontransfer patients (Table 1).
Demographic and clinical characteristics of the study sample*
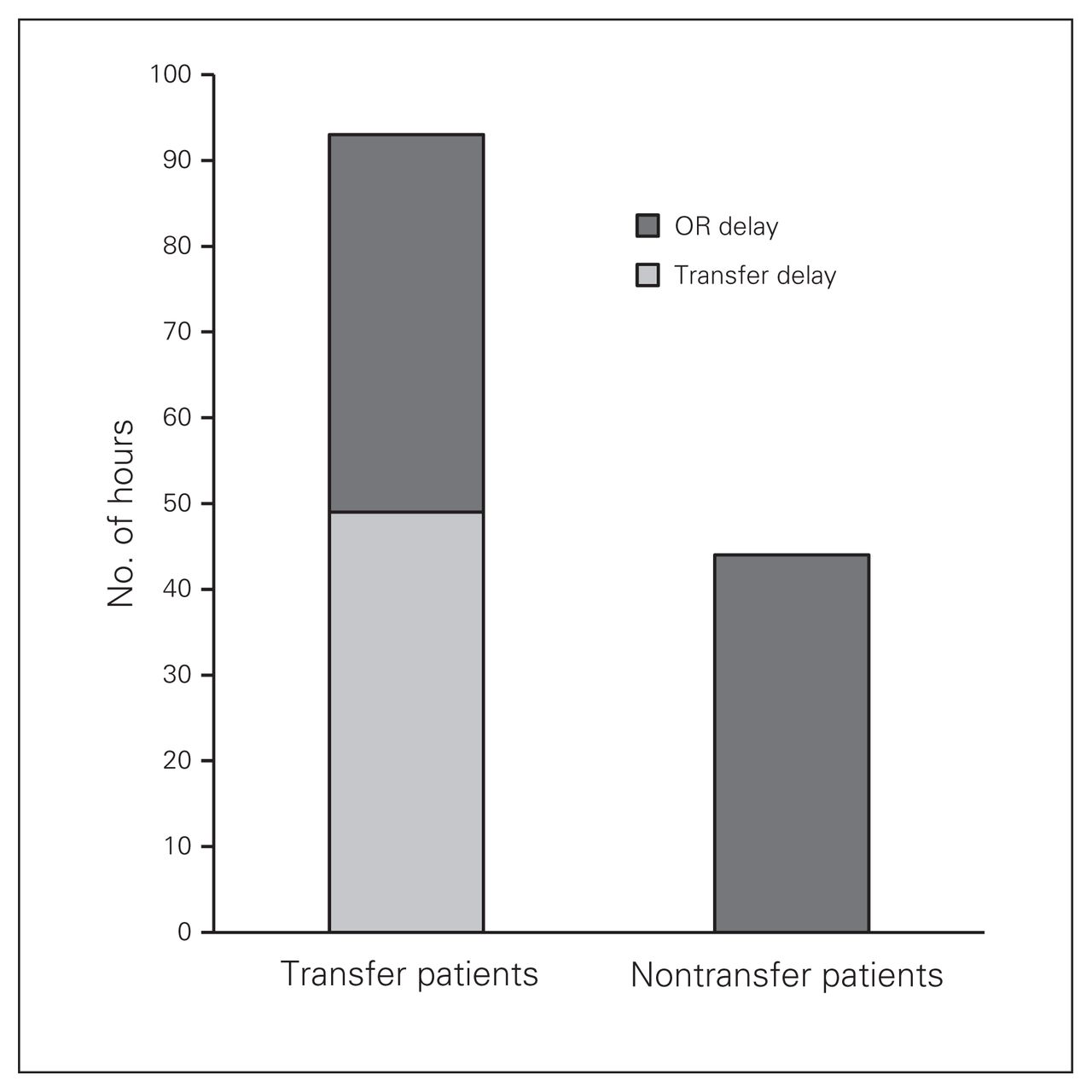
Transfer patients had a median transfer delay from admission to regional centre to admission to tertiary centre of 49 hours. These patients waited an additional 44 hours from admission to tertiary centre to operation, for a total median delay of 93 (range 6–398) hours. Nontransfer patients waited 44 (range 4–743) hours from admission to operation (p < 0.001; Fig. 1). After policy changes were enacted in April 2011, a shorter transfer delay resulted; prior to policy changes, the median transfer delay was 47 hours, whereas after these changes the median transfer time decreased to 27 hours (p = 0.005).

Delay to surgery. Nontransfer patients had a delay of 44 hours from admission to operation, whereas transfer patients had a transfer delay to tertiary care hospital of 49 hours, then a delay from admission to tertiary care hospital to operation of 44 hours, for a total delay of 93 hours (p < 0.001). OR = operating room.
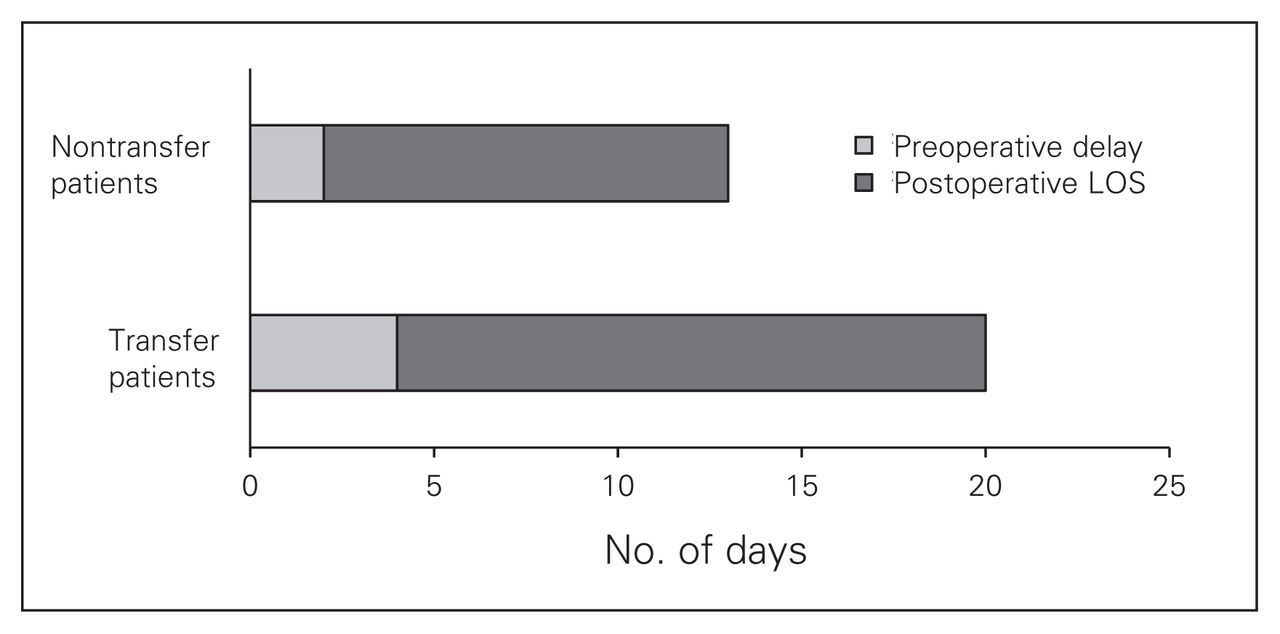
Transfer patients had a median LOS of 20 days compared with 13 days for nontransfer patients (p < 0.001; Fig. 2). There were no statistical differences in complications between the 2 groups (all p > 0.05; Table 2). The only difference was that the nontransfer group had a higher rate of UTIs (9.0% v. 1.7%, p < 0.001). There was no change in total LOS after policy changes were enacted in April 2011.
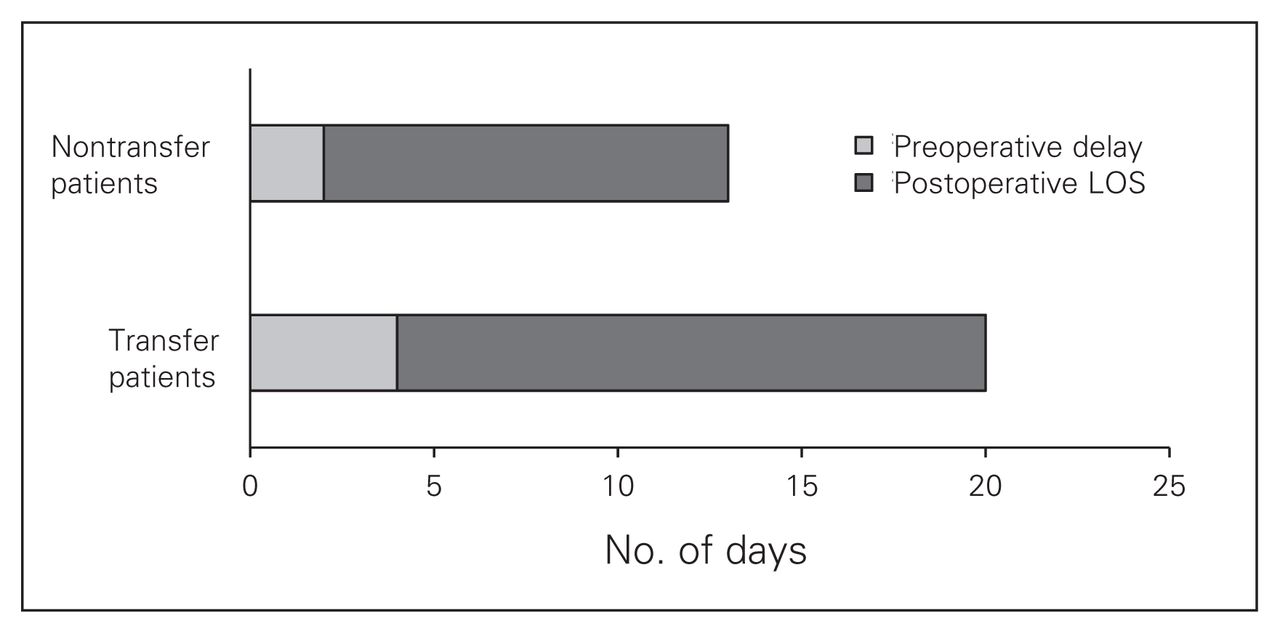
Total length of hospital stay (LOS). Nontransfer patients waited 2 days for surgery and stayed 11 days postoperatively prior to discharge. Transfer patients waited 4 days for surgery and stayed 16 days postoperatively (p < 0.001).
Postoperative complications of the study sample
Discussion
Both transfer and nontransfer patients waited approximately 44 hours from admission to tertiary care centre to operation. Transfer patients waited an additional 49 hours between admission to referring hospital and admission to tertiary care centre. Regional policy changes, however, can have a significant impact on transfer times. After April 2011, when patients with hip fractures were given a higher transfer priority, transfer time decreased from 47 to 27 hours (p = 0.005). These findings demonstrate the true effect that prioritizing patients with hip fractures has on overall wait times. Based on previously mentioned large cohort studies, this decrease in transfer time has a significant impact on overall mortality.1–3
We also found that transfer patients had a greater total LOS than patients directly admitted to the tertiary care centre. Transfer patients had a median total LOS of approximately 20 days compared with 13 days for nontransfer patients (p < 0.001). Prolonged preoperative recumbency accelerates deconditioning and affects nutritional status, all of which may result in a prolonged period of recovery postoperatively. During the postoperative course, most patients were repatriated back to the presenting hospital. This increased travel may have interrupted the patients’ rehabilitation, further delaying their discharge from the referring hospital. The disparity in discharge protocols between community and tertiary care centres may also contribute to the delay in discharge. Dedication to physical therapy, access to short- and long-term care facilities and differing pressure on making beds available may all play a role in delaying discharge from community hospitals. This delay brings into question whether all patients with hip fractures should be treated, rehabilitated and discharged in a dedicated centre. This centre would be dedicated to prompt admission, optimization by internal medicine and short surgical delay, followed by dedicated physical therapy and social work for discharge planning. Treatment in a dedicated centre could decrease both surgical delay and LOS.
In addition to the detrimental effects on patients, the cost of hip fracture care is also greatly increased with a prolonged LOS. In Canada, it is estimated that the basic cost per day for the care of a surgical patient is $1500. This does not include the cost of surgical intervention, medications or transportation for the transfer of patients to and from referring hospitals. Transfer patients’ LOS was approximately 20 days, which translated to a cost of about $30 000; nontransfer patients stayed 13 days, which translates to a cost of about $19 500. With our aging population and increasing life expectancy, it is estimated that the number of hip fractures occurring worldwide will increase from 1.66 million in 1990 to 6.26 million in 2050.8 This increased frequency of hip fractures will result in significantly increased cost of hip fracture care. Providing expedited transfer of patients would result in shortened LOS and would help mitigate overall costs.
Limitations
There are limitations to this study that should be considered. First, although this study included 890 patients, these numbers remain insufficient to detect differences in uncommon events. However, we are able to extrapolate our wait time and LOS data with previous large cohort studies.3 Second, there may be an inherent difference in the transferred and nontransferred patients that could not be determined by this retrospective, observational study. Transfer patients who had longer delays to surgery may have had more medical comorbidities, which in turn may have increased their baseline risk for mortality and complications. However, based on our patient demographic characteristics, there are likely no major differences between the two populations.
Conclusion
Patients with hip fractures who were transferred from referring hospitals had an extended surgical delay compared with those admitted directly to the tertiary care centre. After policy changes were enacted prioritizing patients with hip fractures, transfer time significantly decreased. Transfer patients also had a significantly longer LOS than patients admitted directly to the trauma centre. Based on the results of the present study, we believe that further prioritization of patients with hip fractures and expediting transfer will decrease overall mortality, reduce LOS and substantially reduce the total episodic cost of hip fracture care. Also, treating all patients with hip fractures in a dedicated centre with internal medicine, orthopedic, physiotherapy and social work services may be beneficial.
Footnotes
Competing interests: None declared.
Contributors: S.J. Desai, A.-R. Lawendy and D. Sanders designed the study. S.J. Desai, J. Patel and H. Abdo acquired and analyzed the data. All authors wrote and reviewed the article and approved the final version for publication.
- Accepted March 29, 2013.
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.