


Abstract
Background: Heart rate variability (HRV) has been used as a measure of stress and mental strain in surgeons. Low HRV has been associated with death and increased risk of cardiac events in the general population. The aim of this study was to clarify the effect of a 17-hour night shift on surgeons’ HRV.
Methods: Surgeons were monitored prospectively with an ambulatory electrocardiography device for 48 consecutive hours, beginning on a precall day and continuing through an on-call (17-h shift) day. We measured HRV by frequency domain parameters.
Results: We included 29 surgeons in our analysis. The median pulse rate was decreased precall (median 64, interquartile range [IQR] 56–70 beats per minute [bpm]) compared with on call (median 81, IQR 70–91 bpm, p < 0.001). Increased high-frequency (HF) activity was found precall (median 199, IQR 75–365 ms2) compared with on call (median 99, IQR 48–177 ms2, p < 0.001). The low-frequency:high-frequency (LF:HF) ratio was lower precall (median 2.7, IQR 1.9–3.9) than on call (median 4.9, IQR 3.7–6.5, p < 0.001). We found no correlation between the LF:HF ratio and performance in laparoscopic simulation.
Conclusion: Surgeons working night shifts had a significant decrease in HRV and a significant increase in pulse rate, representing sympathetic dominance in the autonomic nervous system.
Trial registration NCT01623674 (www.clinicaltrials.gov).
Shifting work hours, sleep deprivation and stress have been shown to affect surgeon performance.1–3 At the same time, there is a negative effect on the health of surgeons themselves.4 The negative effects are burnout and poor mental health.5–7 This stress induces changes in the autonomic nervous system that can be recorded noninvasively by an ambulatory electrocardiography (ECG) device with subsequent statistical analysis of heart rate variability (HRV). Heart rate variability has been used as a measure of mental strain in surgeons performing laparoscopic versus conventional surgery8 and in surgeons performing laparoscopic surgery in modern operating rooms compared with standard ones.9 Furthermore, HRV has been used as a measure of stress in surgeons before, during and after night shifts with a standardized resting period of 10 minutes.10 The HRV correlated with perceived stress, showing decreased stress levels during the night shift. A study by Nishi and colleagues11 stated that the lifespan of surgeons and obstetrician/gynecologists was shorter than that of physicians in basic medical sciences and internal medicine; the authors suggested that one of the reasons for this shorter lifespan was the degree of stress from work conditions. Furthermore, a systematic review and meta-analysis of 34 studies found that shift work was associated with increased risk of myocardial infarction and ischemic stroke.12 However, no increased mortality was associated with shift work.
Low HRV has a prognostic value in patients with myocardial infarction as a predictor of death and as a tool for risk stratification after myocardial infarctions.13 In the general population, low HRV has been associated with death and increased risk of cardiac events.14,15 To our knowledge, no previous study has investigated the development of HRV during an entire night shift among medical personnel. Our aim was to clarify the effect of a 17-hour night shift on surgeons’ HRV.
Methods
Design
Surgeons were monitored prospectively with an ambulatory ECG device for 48 consecutive hours. The monitoring period started at 8 am on the morning precall and continued through the second day, on which the surgeons worked a 17-hour night shift from 3:30 pm to 8:30 am. The ECG monitoring was discontinued at 8 am on the morning postcall. Overall, the surgeons were monitored for psychomotor performance, cognition, circadian rhythm, sleep and fatigue over a period of 4 consecutive days. Data on psychomotor performance, cognition and sleep have been published separately.16
Participants
We included male and female interns, residents and attending surgeons from an academic surgical department in a prospective monitoring study. The participants did not work night shifts in the 72 hours preceding the study in order to avoid pre-existing sleep deprivation. They were instructed to get their habitual amount of nighttime sleep during this period. Furthermore, individuals receiving medical treatment for known endocrine, autoimmune or heart conditions were excluded, as were those with a previously diagnosed sleep disorder. Pregnant or breastfeeding women were not included. Consumption of alcohol or stimulants in the 24 hours preceding the study and during the study was not allowed. As we wished to monitor the surgeons in the habitual state, we did not restrict their intake of liquids containing caffeine.
HRV recording
We started a 48-hour ECG recording on the morning of the precall day, and recording continued through the on-call day. The ECG recording was discontinued on the morning postcall. We performed HRV monitoring using the Medilog AR12 recorder (Oxford Instruments Tubney Woods) with a 3-channel, 5-lead recording. We analyzed the HRV parameters using Medilog Darwin software (Huntleigh Healthcare). Mean values of short-term 5-minute recordings were manually viewed and excluded for noise, ectopy and missing beats; only normal-to-normal R waves were included to obtain reliable data. The normal-to-normal R waves are known as the NN interval. Only intervals with more than 90% valid data were included.
The parasympathetic (vagal) and sympathetic activity constantly interact. The vagal afferent stimulation leads to excitation of vagal efferent activity and, by reflex, inhibits sympathetic efferent activity.17 The opposite effects are mediated by the stimulation of sympathetic activity. The efferent vagal activity is a major contributor of high- frequency (HF) power. However, the interpretation of the low-frequency (LF) power is more controversial; some believe it represents sympathetic activity, whereas others argue it represents a parameter that includes both sympathetic and parasympathetic activity.17 In the present study, an increase of the LF power was used as a measure of sympathetic and parasympathetic activity,18,19 and HF power was used as a measure of increase in parasympathetic activity.17,20 The LF:HF ratio was used as an index of the sympathovagal balance.19,21,22 An increase in this ratio represented a larger sympathetic influence on the HRV, and a decrease represented a larger vagal influence.
Data analysis
Analysis was performed according to the guidelines of the HRV task force.17 The HRV power spectra were calculated using fast Fourier transformation.17 Two main spectral components were distinguished: an LF component of 0.04–0.15 Hz and an HF component of 0.15–0.4 Hz. The power and frequency of each spectral component were calculated as absolute units (milliseconds squared). We measured heart rate from the mean NN values. The medians of the 5-minute intervals were determined for every hour. Then we determined the medians of the hourly intervals from 4 pm to 8 am precall and on call for every participant.
Ethics and permissions
Our trial fully complied with the Helsinki declaration on biomedical research. The Danish Regional Committee on Biomedical Research Ethics evaluated and approved the trial (H-4–2011–095). The Danish Data Protection Agency approved the collection, analysis and storage of data (2011–41–6384). All participants gave their informed consent before inclusion in the study. Participation in the study was voluntary; all participants received 500 Danish kroner (equivalent to $90 USD) at the end of the study. The trial was registered at www.clinicaltrials.gov (NCT01623674).
Statistical analysis
We used SPSS software version 19.0 for data entry and statistical analysis. Group values are presented as medians and interquartile ranges (IQRs). We used the Wilcoxon test for paired intragroup comparisons and the Friedman test for repeated intragroup comparisons. We considered results to be significant at p < 0.05.
Results
Thirty surgeons participated in the study; however, we included the data for only 29 participants in our analyses. One surgeon was excluded because she received a diagnosis of myxoedema 8 weeks after her participation in the study. Thus, the results are based on data from 9 interns, 11 residents and 9 attending surgeons. The median work experience was 5 (IQR 1–9) years. Participant characteristics are presented in Table 1.
The age, weight and height of the participants
The development of HF power from 4 pm to 8 am precall and on call is shown in Figure 1. We found a significant difference in the development over time for both precall and on-call values. The median pulse rate is presented as a box plot in Figure 2A. The precall pulse rate was lower (median 64, IQR 56–70 beats per minute [bpm]) than the on-call pulse rate (median 81, IQR 70–91 bpm, p < 0.001). High-frequency activity is presented as a box plot in Figure 2B. The vagal activity was higher precall (median 199, IQR 75–365 ms2) than on call (median 99, IQR 48–177 ms2, p < 0.001). Fig. 2C illustrates the LF:HF values as a measure of sympathovagal balance, with a median of 2.7 (IQR 1.9–3.9) precall and 4.9 (IQR 3.7–6.5) on call (p < 0.001). There were no significant differences between precall values and on-call values in LF power (Fig. 2D). In order to account for differences in training levels, we conducted subgroup analyses for the interns, residents and attending surgeons for the LF:HF ratio as a representative for the sympathovagal balance. No significant differences were found (Kruskal–Wallis test). In order to examine the association between HRV and performance in the laparoscopic simulator, we used the Spearman correlation test for the LF:HF ratio and performance for the precall and on-call day. Performance was measured as time in laparoscopic simulation, as this was the primary outcome of the overall study.16 No correlation was found between the LF:HF ratio and time in laparoscopic performance (precall: r = −0.20, p = 0.92; on call: r = −0.24, p = 0.20).

The development of high-frequency (HF) power from 4 pm to 8 am (16:00–08:00) for the precall and on-call days. Squares represent precall values with a p < 0.001. Circles represent on-call values with a p < 0.001. The p values were determined using the Friedman test. The decrease in HF power from 10 pm to 7 am (22:00–07:00) on call represents a decrease in vagal activity.
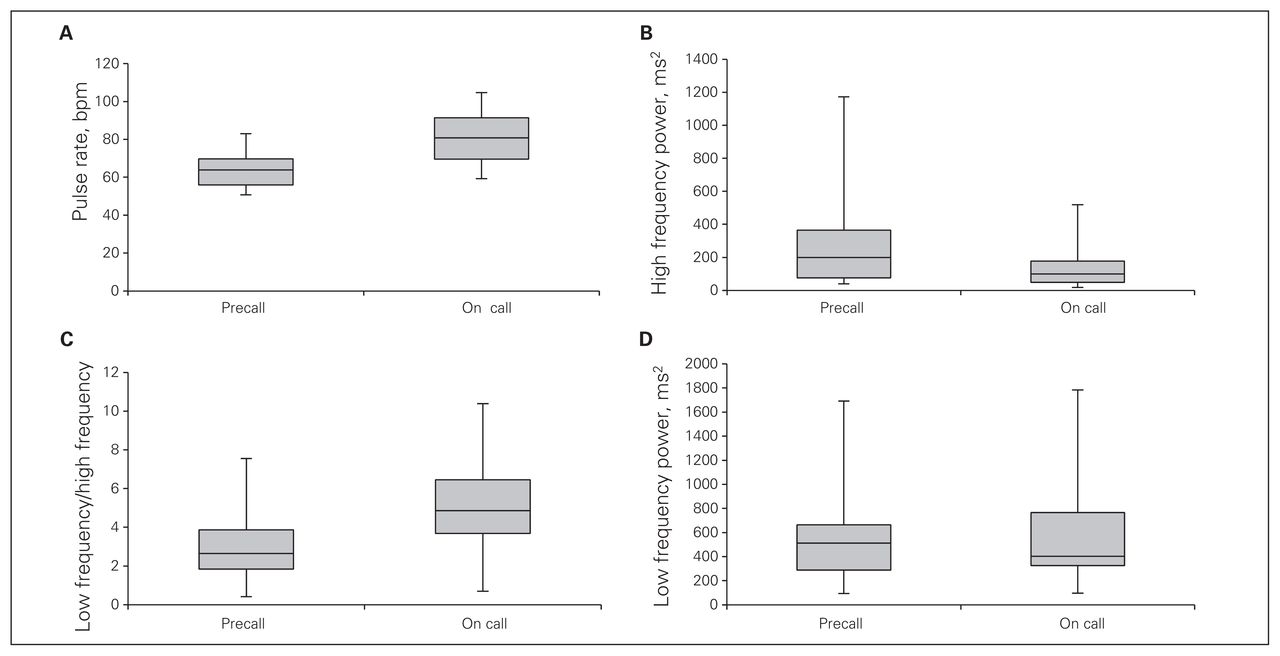
(A) Median pulse rate from 4 pm to 8 am precall and on call (p < 0.001, Wilcoxon test). (B) High-frequency (HF) power from 4 pm to 8 am precall and on call (p < 0.001, Wilcoxon test). The median precall HF value was higher and had a wider interquartile range (IQR) than the on-call value, demonstrating a greater parasympathetic influence. (C) The LF:HF ratio as a measure of the sympathovagal balance from 4 pm to 8 am precall and on call (p < 0.001, Wilcoxon test). The decrease in the LF:HF ratio precall represents a larger vagal influence, and the increase on call represents a larger sympathetic influence on heart rate variability. (D) Low- frequency (LF) power from 4 pm to 8 am precall and on-call (p = 0.39, Wilcoxon test). Boxes represent the IQRs. Lines within the boxes represent the medians. Whiskers represent minimum and maximum IQR values.
Discussion
Our results showed a change in the autonomic nervous system activity, with sympathetic dominance in the nighttime on-call values compared with precall values. The HF values were significantly increased on the precall night compared with the on-call night, demonstrating a higher vagal influence (Figs. 1 and 2A). The surgeons had a significantly higher pulse rate (Fig. 2A) during the 17 hours they worked on a night shift, which supported the findings of sympathetic dominance of the autonomic nervous system activity while on call. The decrease in LF:HF ratio supported a larger vagal influence on the sympathovagal balance precall, and the increase in LF:HF ratio on call demonstrated a sympathetic dominance (Fig. 2C). However, the LF values did not differ significantly when precall values were compared with on-call values (Fig. 2D), possibly owing to LF values representing both vagal and sympathetic influence on the HRV. The overall findings may be explained solely by surgeons being awake overnight; still, the findings demonstrate physiologic stress regardless of surgeons’ training levels.
Our study also showed that surgeons had decreased HRV during on-call hours, as the vagal activity was significantly reduced. A previous study examined anesthesiologists, pediatricians and otolaryngologists and compared their HRVs from 9 pm to 10 pm after daytime work, on a night shift and on the day after a night shift.23 The study found decreased HRV after daytime work and on a night shift in anesthesiologists compared with the other specialists, indicating higher physiologic stress. The tasks of anesthesiologists can be compared with the tasks of surgeons, as both have a large workload at night because acute situations may arise at all times.
It has been shown previously that low HRV from a 2-minute rhythm strip predicted increased mortality due to poor general health.24 The authors selected a random sample of 900 patients without prevalent coronary heart disease at baseline. The patients with low HRV determined from a 2-minute rhythm strip had an adverse cardiovascular risk profile and elevated risk of death from all causes, including cancer. This may imply that the night shifts causing a reduced HRV and higher pulse rate in surgeons may have a negative impact on their general health in the long run and may cause increased mortality.
Surgeons’ stress and ways to reduce or cope with stress have been described previously. A study used an anonymous self-report questionnaire and a randomized response technique (RRT), with a high degree of anonymity, to assess the use of prescribed or illicit drugs solely with the purpose of cognitive or mood enhancement among surgeons.25 According to the questionnaire, 8.9% of surgeons reported that they had used drugs at least once, merely for cognitive enhancement; however, the RRT revealed a prevalence of 19.9%. For mood enhancement, 2.4% of the surgeons stated on the questionnaire that they had used antidepressants; again, the RRT revealed a higher prevalence (15.1%). The use of drugs is hardly recommended as a coping strategy for stress in surgeons. A study found that scheduled intraoperative breaks reduced surgeons’ cortisol levels by 22%, without prolonging the operation.26 A systematic review looking at residents’ health found 2 studies on protected sleep time to reduce residents’ fatigue.27 Further studies on scheduled breaks and protected sleep time with a focus on how surgeons’ stress can be reduced are needed.
The strengths of the present study were that HRV monitoring and analysis were performed continuously for the 17-hour periods of evening and nighttime both precall and on call, providing solid insight on the sympathovagal balance of the entire recording period. Unfortunately, we did not perform postcall HRV monitoring. This would have strengthened the study further, as it would have shown when a normalization of the sympathovagal balance took place.
Conclusion
Our study showed a significant decrease in HRV and a significant increase in pulse rate in surgeons working night shifts compared with nighttime hours off call. Future studies could investigate methods to reduce sympathetic dominance during night shifts, as the decreased HRV may be harmful to surgeons’ health.
Acknowledgements
The study was financially supported by the Tryg Foundation and The Danish Medical Association. The sponsors played no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review, or approval of the manuscript.
Footnotes
Competing interests: None declared.
Contributors: I. Amirian, J. Rosenberg and I. Gögenur designed the study. I. Amirian and L. Andersen acquired the data, which all authors analyzed. I. Amirian and I. Gögenur wrote the article, which all authors reviewed and approved for publication.
- Accepted February 7, 2014.
References
In this issue

{kind=link}
{kind=link}
Article tools





