


Summary
The ability to tie surgical knots efficiently and effectively is an essential surgical skill for medical procedures, especially pacemaker implantation. Device generators and their leads need to be safely anchored with sutures during implantation to prevent dislodgement and inadequate packaging in the pacemaker pocket. With most knot tying techniques, a generous amount of suture slack is required. We introduce a new technique that is a variation of the 2-handed surgical square knot and the 1-handed surgeon’s knot that allows one to finish or tie a knot when left with little slack.
There are many ways to tie a suture during a surgical procedure.1–3 Depending on the surgeon’s experience and familiarity with a technique, most knots can be completed fairly rapidly. The 1-handed knot technique, or surgeon’s knot, is a common method.1–3 With most knot tying techniques, a generous amount of suture slack is required. We introduce a technique that is a variation of the 2-handed surgical square knot and the 1-handed surgeon’s knot that will allow one to finish or tie a knot when left with little slack. Depending on the finger size of the surgeon, with this new technique a knot can be made with a few centimeters or less of suture slack, obviating the need for a new suture or an instrument tie. This new technique allows greater efficiency and allows salvaging a knot during the crucial part of a procedure. This new 1-handed knot tying technique, which we term the “frugal tie,” allows the completion of a knot with very little slack.
The frugal tie technique
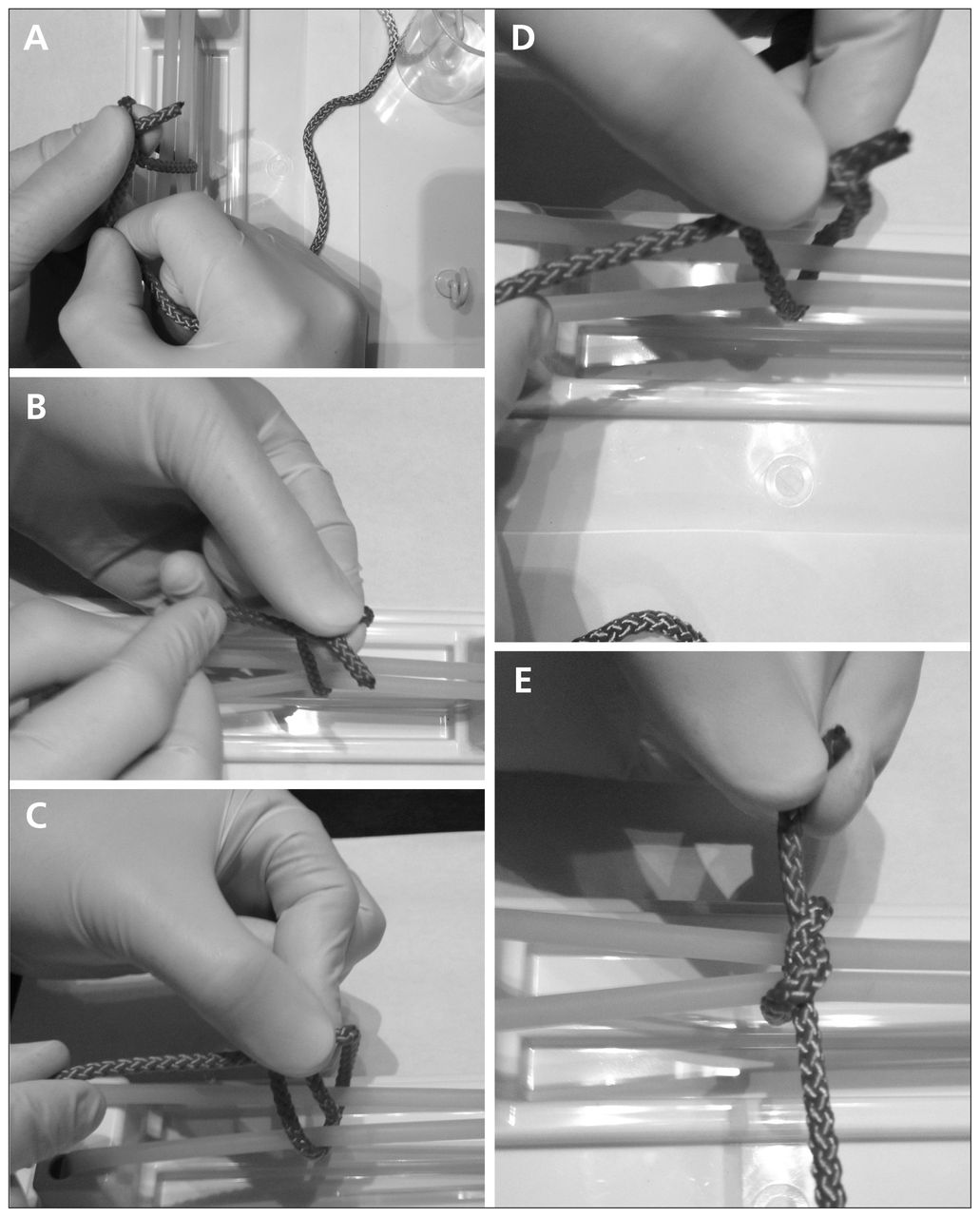
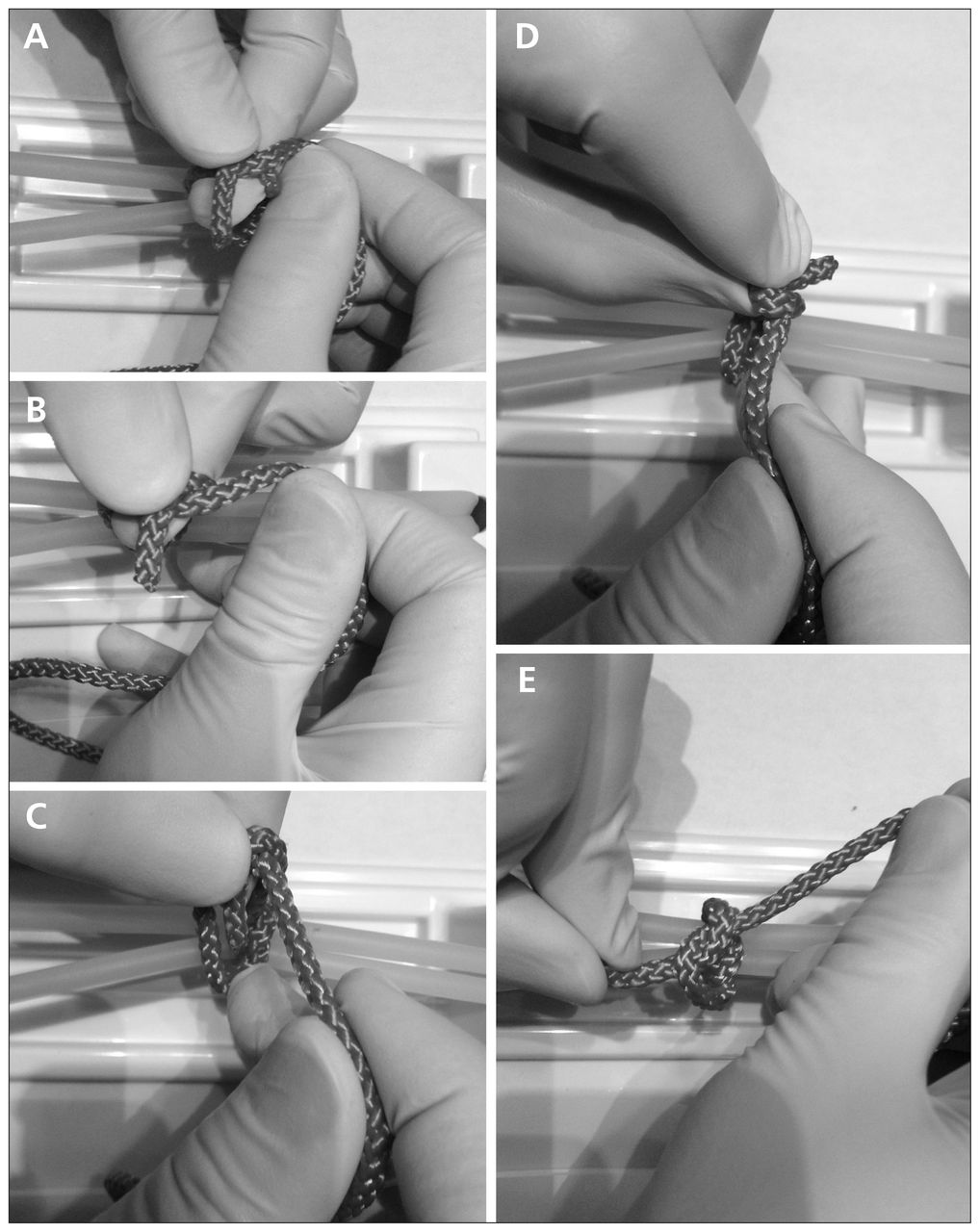
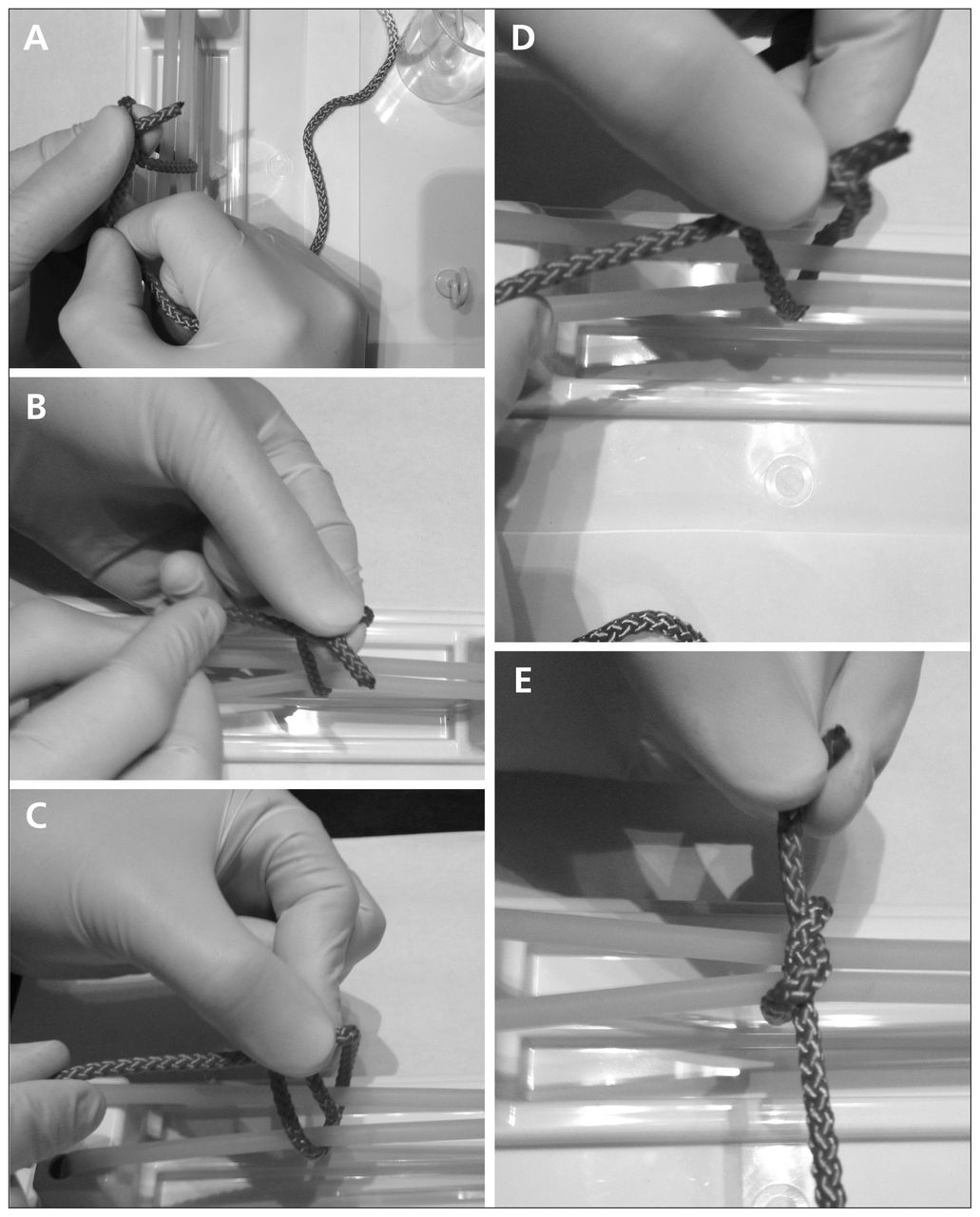
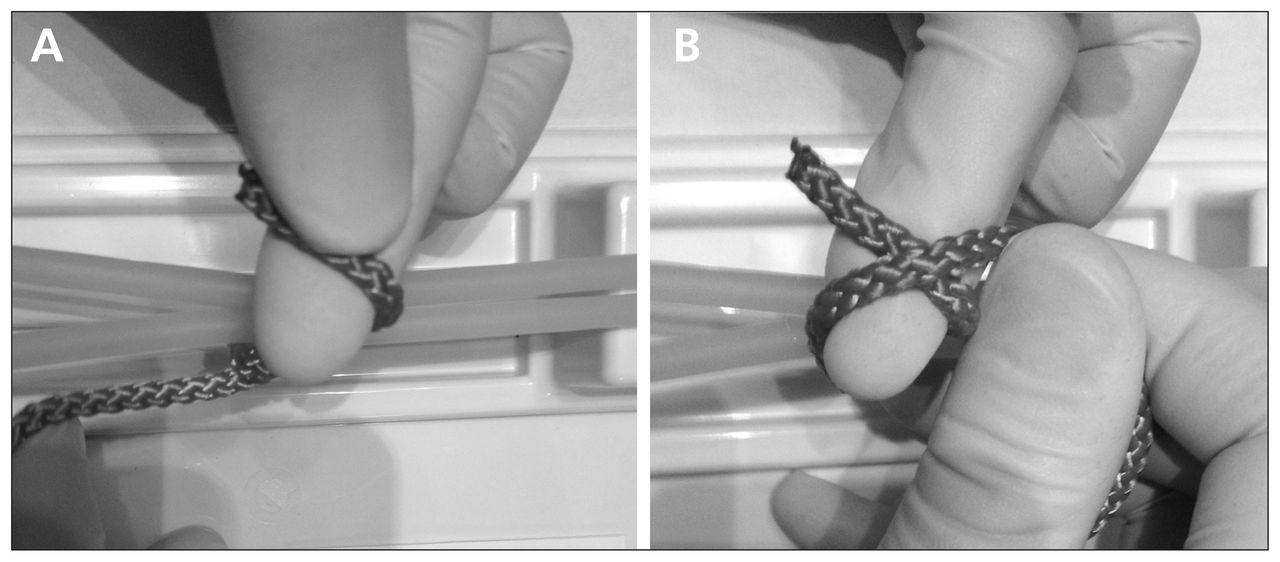
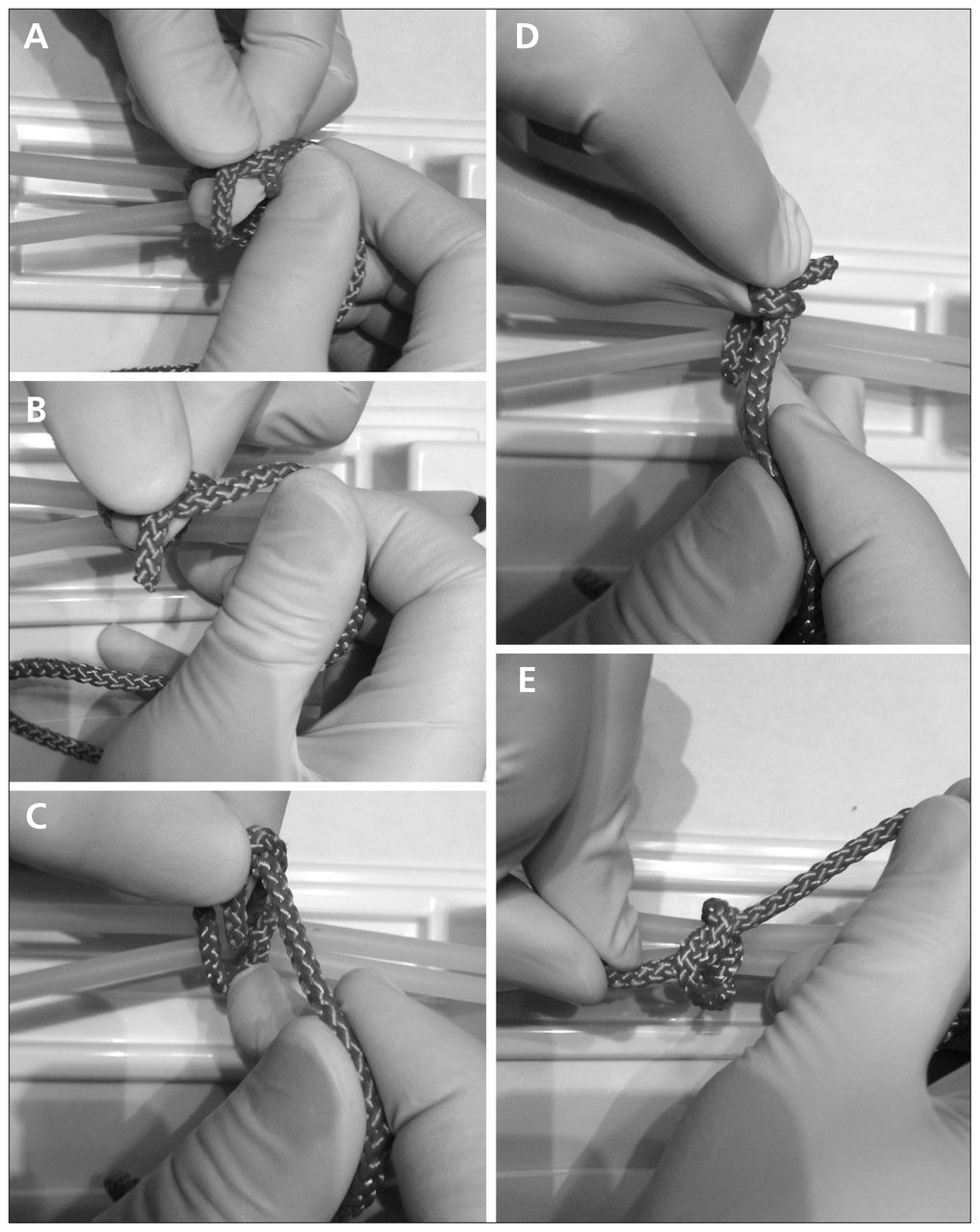
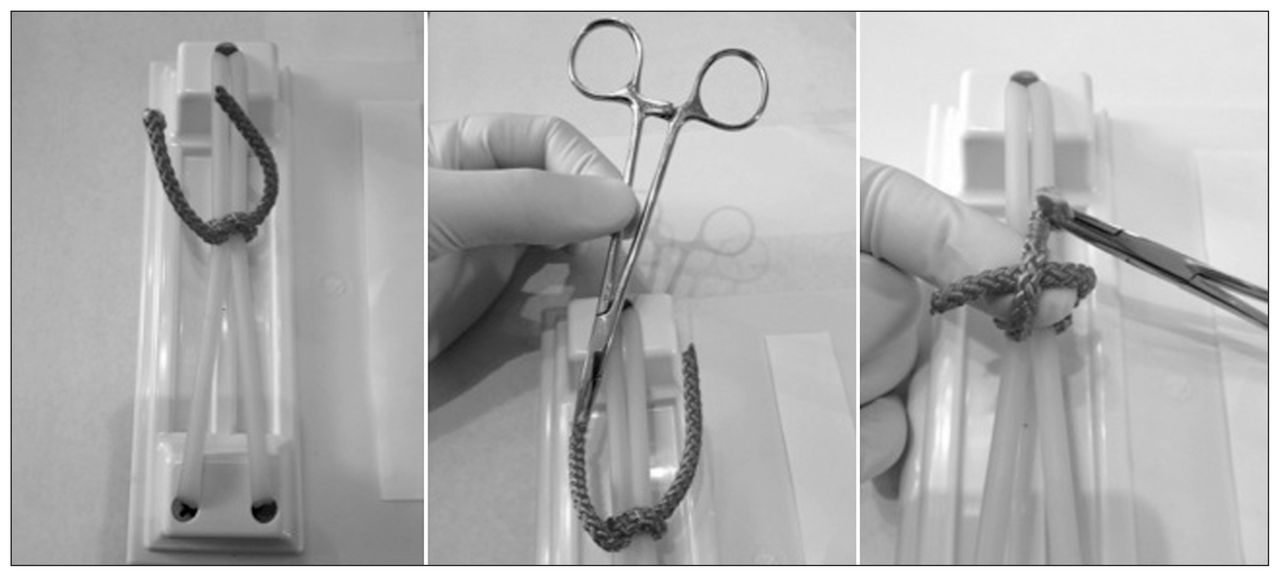
To start the knot, the short end of the suture is wrapped below the index finger (step 1; Fig. 1A). The long end of the suture then locks the short end in place (step 2; Fig. 1B). Using the thumb of the hand holding the short end of the suture, the short end is folded over the long end (step 3; Fig. 2A) and then folded over the short end of the suture (step 4; Fig. 2B). The folded end of the suture is pinched by the thumb and passed through the loop (step 5; Fig. 2C). The short end of the suture is then grasped by the same thumb and index fingers or the same thumb and middle finger once passed through the loop and the knot placed down over the anticipated area (steps 6 and 7; Figs. 2D and E). Steps 3–7 are completed in a continuous motion. To lock/reverse the tie, complete the second throw by wrapping the short end of the suture above the index finger instead of below it, as in step 1 (step 8; Fig. 3A). The long end of the suture locks the short end in place (step 9; Fig. 3B). As in step 3, using the thumb of the hand holding the short end of the suture, the short end is folded over the long end (step 10, Fig. 4A) and the knot is completed as described in steps 5–7; the short end of the suture is subsequently grasped by the same thumb and index fingers or the same thumb and middle finger once passed through the loop, and the knot is placed down over the anticipated area. Steps 10–14 are also completed in a continuous motion (Fig. 4C–E). Figure 5 shows the final configuration of the frugal tie, similar to a surgeon’s knot. Figure 6 shows a variation of the frugal tie technique using a needle driver when both ends of the suture are very short; the end of the suture held by the needle driver becomes the long end represented in Figure 1, and the described technique to complete the frugal tie is performed.
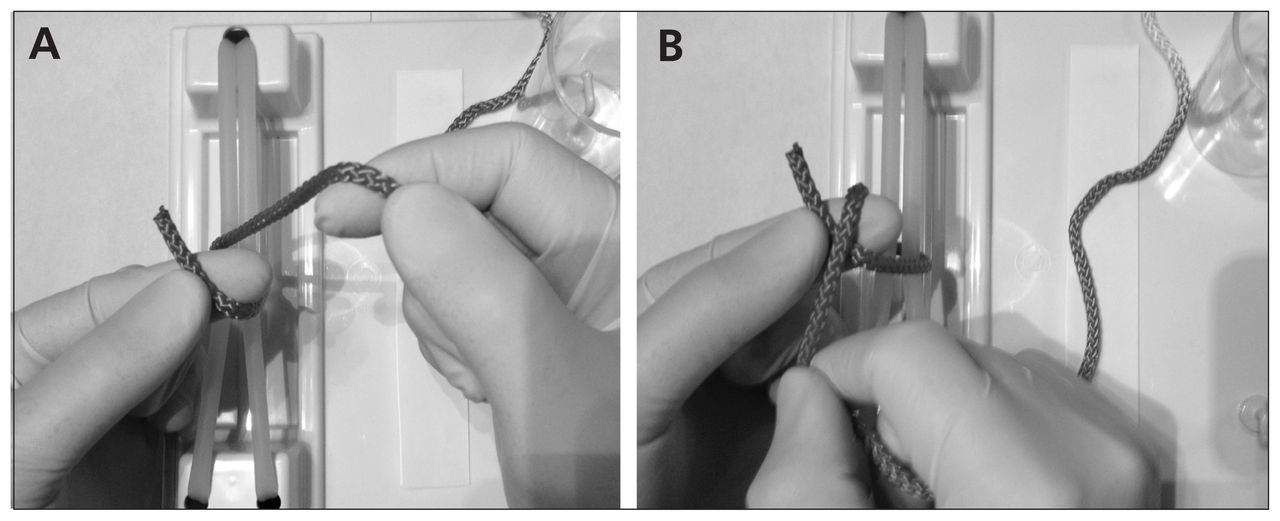
(A) Step 1: to start the knot, the short end of the suture is wrapped below the index finger (B) Step 2: the long end of the suture locks the short end in place.
(A) Step 3: using the thumb of the hand holding the short end of the suture, the short end is folded over the long end and then (B) folded over the short end of the suture. (C–E) Steps 5–7: the folded end of the suture is pinched by the thumb and passed through the loop. The short end is subsequently grasped by the same thumb and index fingers or the same thumb and middle finger once passed through the loop and the knot placed down over the anticipated area. Steps 3–7 are completed in a continuous motion.

(A) Step 8: Locking/reverse tie. To place the second throw, the short end of the suture is wrapped above the index finger instead of below, as in step 1. (B) Step 9: the long end of the suture locks the short end in place.
(A) Step 10: as in step 3, using the thumb of the hand holding the short end of the suture, the short end is folded over the long end. (B) Step 11: the short end of the suture is folded over. (C–E) Steps 12–14: the folded end of the suture is pinched by the thumb and passed through the loop. The short end of the suture is subsequently grasped by the same thumb and index fingers or the same thumb and middle finger once passed through the loop and the knot placed down over the anticipated area. Steps 10 to 14 are completed in a continuous motion.

Final configuration of the frugal tie. Note that the configuration is similar to a surgeon’s knot.

Variation on the frugal tie technique using a needle driver when both ends of the suture are very short. The end of the suture held by the needle driver becomes the long end represented in Fig. 1, and the same technique to complete the frugal tie is performed.
Discussion
In the surgical field, knot tying is an essential component of the procedure. In experienced hands surgical knots can be tied quickly, but they typically require a generous amount of suture slack. We introduce a knot tying technique that is a variation of the 2-handed surgical square knot and the 1-handed surgeon’s knot that allows one to finish or tie a knot with very little slack on the suture. If completed properly with adequate tension, this modified technique will have similar strength as the 1-handed surgeon’s knot as they both have similar locking principles in their throws (Fig. 5). The flat square knots and surgeon’s knot have been shown to have similar tension at failure and similar likelihood of untying.2 Given the similarity in the knot configuration to the surgeon’s knot, the frugal tie technique will offer the same reliability as this standard approach.
Acknowledgements
Dr. Exner is Canada Research Chair in Cardiovascular Clinical Trials. Images provided by Joseph Rizkallah Photography.
Footnotes
Completed poster presentations at the Libin Research Day, Apr. 8, 2014, and at the Cardiostim EHRA Europace conference, June 18–21, 2014.
Competing interests: None declared.
Contributions: All the authors read, approved, and contributed to the manuscript.
- Accepted April 3, 2014.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.