


Abstract
Background: Trauma remains a leading cause of death worldwide. The development of trauma systems in low-resource settings may be of benefit. The objective of this study was to describe operative procedures performed for trauma at a tertiary care facility in Kigali, Rwanda, and to evaluate geographical variations and referral patterns of trauma care.
Methods: We retrospectively reviewed all prospectively collected operative cases performed at the largest referral hospital in Rwanda, the Centre Hospitalier Universitaire de Kigali (CHUK), between June 1 and Dec. 1, 2011, for injury-related diagnoses. We used the Pearson χ2 and Fisher exact tests to compare cases arising from within Kigali to those transferred from other provinces. Geospatial analyses were also performed to further elucidate transfer patterns.
Results: Over the 6-month study period, 2758 surgical interventions were performed at the CHUK. Of these, 653 (23.7%) were for trauma. Most patients resided outside of Kigali city, with 337 (58.0%) patients transferred from other provinces and 244 (42.0%) from within Kigali. Most trauma procedures were orthopedic (489 [84.2%]), although general surgery procedures represented a higher proportion of trauma surgeries in patients from other provinces than in patients from within Kigali (28 of 337 [8.3%] v. 10 of 244 [4.1%]).
Conclusion: To our knowledge, this is the first study to highlight geographical variations in access to trauma care in a low-income country and the first description of trauma procedures at a referral centre in Rwanda. Future efforts should focus on maturing prehospital and interfacility transport systems, strengthening district hospitals and further supporting referral institutions.
An estimated 5.8 million people die annually from injury-related events, representing more than 10% of deaths worldwide each year. The 3 most common causes of injury-related deaths — road traffic crashes, homicide and suicide — are expected to rise substantially in the coming years, joining the top 20 causes of death by 2030.1 Not all groups are equally vulnerable to injuries. Trauma is 1 of the top 3 leading causes of death in people between the ages of 5 and 44 years, the most productive portion of the population. Moreover, approximately 90% of injury-related deaths occur in low- and middle-income countries (LMICs).1
The development of trauma systems, including regionalized trauma care and the utilization of referral trauma centres, has been shown to significantly decrease injury-related mortality in high-income nations.2–4 There is evidence that the development of trauma systems in LMICs, specifically prehospital care, could yield similar results.5,6
Nonetheless, the vast majority of studies evaluating trauma care in LMICs rely on evaluations of hospital-based resources.7–10 Although these studies provide valuable information regarding the potential capacity to treat injuries, there is a paucity of evidence regarding the actual utilization of resources in trauma and barriers to access definitive care. With the recent launch of the Lancet Commission on Global Surgery,11 increasing attention is being paid to this issue; however, primary data collection, particularly hospital-based data, appears to be invaluable for advocacy efforts.12
In this context, the objective of our study was to describe operative procedures performed for trauma at a tertiary care facility in Kigali, Rwanda, and to evaluate geographical variations and referral patterns of trauma care in Rwanda.
Methods
Context
The Centre Hospitalier Universitaire de Kigali (CHUK) is the largest of 4 referral hospitals in Rwanda and is 1 of the 2 referral hospitals located in Rwanda’s most populated and capital city, Kigali. The CHUK serves an estimated population of more than 6.2 million.13,14 With approximately 513 beds, the CHUK provides the following services: surgery, obstetrics/gynecology, internal medicine, pediatrics, radiology, ophthalmology, dermatology and laboratory services. Critical care support is available, but bed capacity is limited. The anesthesia program is well developed and has been described previously.15 The hospital contains a total of 14 operating rooms separated into multiple distinct physical locations. The main operating theatre has 6 operating rooms; 2 are used for urgent operations and the remaining 4 are used for elective procedures by the departments of general surgery, orthopedics, urology, otorhinolaryngology and neurosurgery. There are separate theatres for minor surgery, oromaxillofacial surgery and ophthalmology.
During off-hours, there is 1 operating room available in the main operating theatre for nonelective cases. At the time of the study, the CHUK employed 5 general surgeons, 3 orthopedic surgeons, 1 neurosurgeon, 1 urologist, 3 otorhinolaryngologists, 1 oromaxillofacial surgeon, 2 ophthalmologists and 5 obstetricians and gynecologists. There is a fully supported surgery residency program associated with the National University of Rwanda with 24-hour resident coverage under attending surgeon supervision. All operations are performed with surgical residents and attending surgeons present.
Data collection
We retrospectively reviewed all operative cases performed at the CHUK between June 1 and Dec. 1, 2011, for injury-related diagnoses. All patients who underwent a surgical procedure for nontraumatic acute care or who underwent elective surgery were excluded. We obtained ethics approval from the CHUK and McGill University.
The CHUK operating room case logs are prospectively completed in a handwritten record by the circulating operating room nurse participating in the operative intervention. The data collected for the purpose of this study included basic patient demographics (age, sex, district of residence in Rwanda), diagnosis, procedure performed, type of anesthesia and booking category (urgent v. nonurgent). Urgent operations were defined as any operation performed with the patient transferred directly to the operating room from the Accident and Emergency Area. In addition, the type of anesthesia administered was recorded and divided into 3 categories: local, regional and general. The procedures were categorized based on the surgical specialties (general surgery, orthopedics, neurosurgery and urology) originally transcribed into the logbooks. Similar methods have been described previously.16 For the purposes of this study, general surgery was defined as any surgery involving the thoracic or abdominal cavity (excluding the genitourinary system), the head/neck (thyroid) and the abdominal wall (including the inguinal region). Authors with specialty training in general surgery (E.G.W, M.C.R., M.D., M.W. and D.L.D.) retrospectively classified the operations into traumatic, nontraumatic acute care and elective surgery based on the diagnoses and the procedures performed. Traumatic operations were defined as any procedure performed specifically for an injury.
Statistical analysis
Handwritten case logs were collected and transcribed into an electronic database (Microsoft Excel). We initially used descriptive statistics to tabulate patient, diagnosis and procedure characteristics. Comparisons between cases originating from within Kigali city and from other provinces were performed using the Pearson χ2 test and the Fisher exact test for cells containing values of 5 or less. Statistical analyses were performed using Stata IC software version 13.1 (StataCorp).
In order to further evaluate geographical patterns, we also performed geospatial analyses. We determined longitude and latitude coordinates of the patients’ residences using Batchgeocoding at www.findlatitudeandlongitude.com (David B. Zwiefelhofer). We used ArcGIS mapping software (Esri) to graphically represent the patients undergoing surgery for injuries at the CHUK from the different districts and provinces of Rwanda.
Results
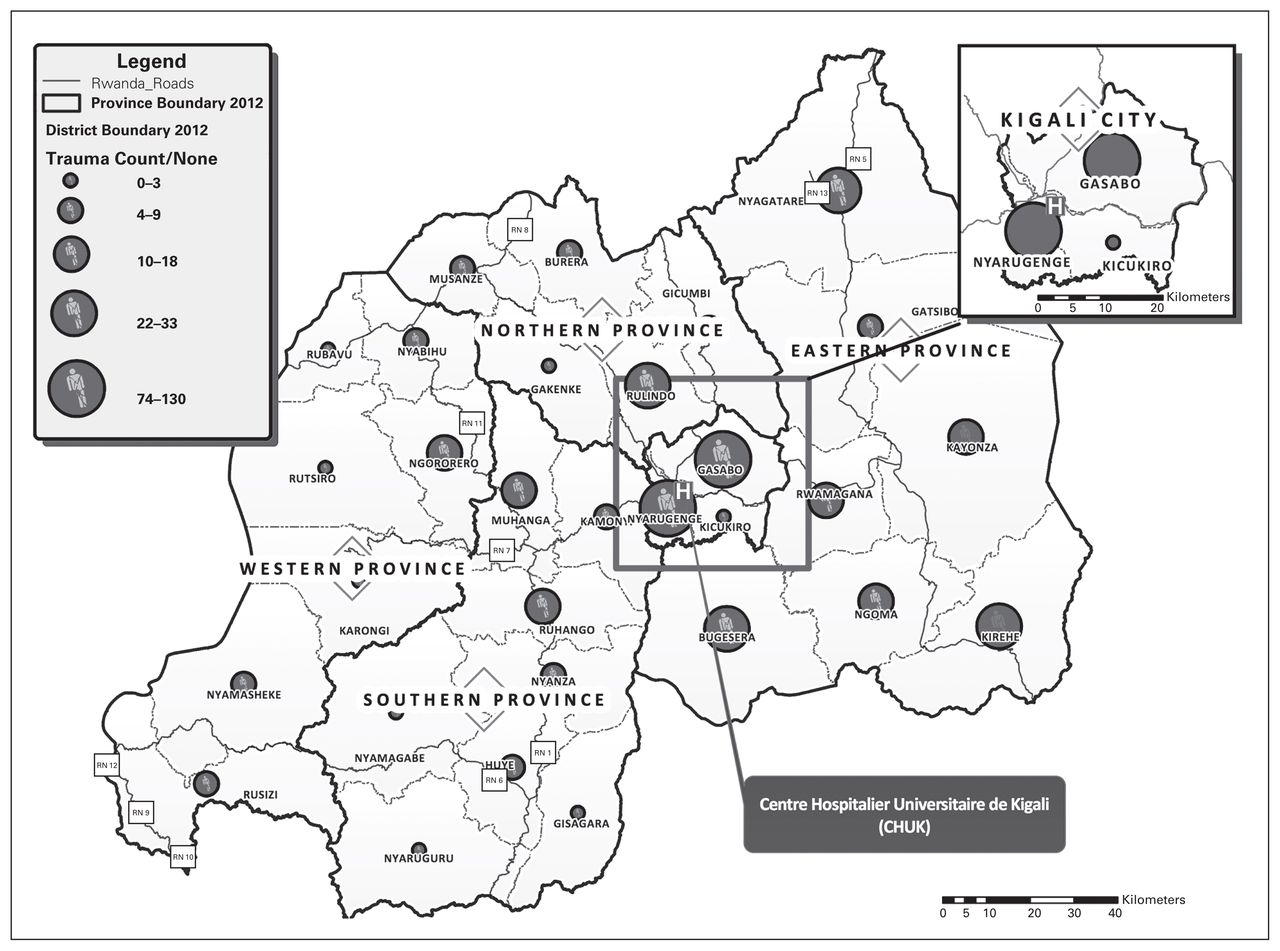
Over the 6-month study period, 2758 surgical interventions were performed at CHUK, spanning all surgical subspecialties and including both urgent and elective procedures. Of these, 653 (23.7%) were performed for trauma. The geographical origins were available for 581 (90.0%) of these patients, whose cases were retained for further analysis. Figure 1 illustrates the point of origin of these patients. The majority of patients resided outside of Kigali city, with 337 (58.0%) patients transferred from other provinces and 244 (42.0%) from within Kigali.

Geographic mapping of origin of patients undergoing injury-related operations at the Centre Hospitalier Universitaire de Kigali (CHUK) in Rwanda between June 1 and Dec. 1, 2011.
Table 1 presents the patient, anesthesia and procedure characteristics according to the geographical origin. Overall, 174 of the 581 (30.0%) patients were children, and proportions were similar between patients from within and outside Kigali. Significantly more patients from other provinces than from Kigali were older than 50 years (84 of 337 [24.9%] v. 38 of 244 [15.6%]). Most patients were between the ages of 18 and 49 years (285 of 581 [49.1%]). Most patients who required operative treatment for trauma were male (411 of 581 [70.7%]), and this proportion was similar regardless of geographical origin.
Demographic and clinical characteristics of trauma patients treated at the Centre Hospitalier Universitaire de Kigali in Rwanda between June 1 and Dec. 1, 2011, by geographical origin
Most of the 581 procedures were performed with the patients under general anesthesia (348 [59.9%]), but some patients received regional (214 [36.8%]) or local (12 [2.1%]) anesthesia. Most operations were performed in an urgent fashion (307 [52.8%]). The proportions of anesthesia modalities and urgent procedures did not differ significantly between patients originating from within Kigali and those from other provinces.
Overall, the vast majority of trauma procedures were orthopedic (489 [84.2%]), followed by neurosurgery (53 [9.1%]), general surgery (38 [6.5%]) and urology (1 [0.2%]). When looking at differences in proportions based on the geographical origins of patients, orthopedic procedures were more prominent in patients from Kigali than in those from outside Kigali (227 of 244 [93.0%] v. 262 of 337 [77.7%]). Interestingly, general surgery procedures represented a higher proportion of trauma surgeries in patients from outside of Kigali than in those from within Kigali (28 of 337 [8.3%] v. 10 of 244 [4.1]). In other words, 73.7% of general surgery operations for injuries were performed on patients from other provinces.
All injuries requiring an operative intervention are detailed in Table 2. The 2 leading indications were fractures (444 [76.4%]) and dislocations (37 [6.4%]). Both of these diagnoses were more common in patients from Kigali (80.7% and 10.3%, respectively) than in patients from outside Kigali (73.3% and 3.6%, respectively). Although neurosurgical indications accounted for a minority of the total number of cases, epidural hematomas (17 [2.9%]) and intracerebral hemorrhages (12 [2.1%]) were the 2 most common neurosurgical indications, and both were more common in patients from other provinces (4.2% and 3.3%, respectively) than in patients from within Kigali (1.2% and 0.4%, respectively). Abdominal trauma represented only 15 (2.6%) traumatic surgical indications overall, but were more frequent in patients from other provinces (13 of 337 [3.9%]) than in patients from within Kigali (2 of 244 [0.8%]); therefore, the vast majority (13 of 15 [86.7%]) of abdominal trauma patients were transferred from outside of Kigali.
Operative indications for trauma at the Centre Hospitalier Universitaire de Kigali in Rwanda between June 1 and Dec. 1, 2011, by geographical origin
Specific operative procedures performed for trauma are displayed in Table 3. Fracture reduction and fixation predominated (416 [71.6%]), followed by wound debridement, drainage or suturing (47 [8.1%]) and craniotomy or craniectomy (40 [6.9%]). Exploratory laparotomy accounted for a minority (11 [1.9%]) of all traumatic procedures. When comparing procedures based on geographical origin, fracture reduction/fixation represented a higher proportion of procedures in patients from Kigali (202 of 244 [82.8%]) than in patients from other provinces (214 of 337 [63.5%]). Neurosurgical procedures, such as craniotomies or craniectomies, were more prominent in patients transferred from outside Kigali (34 of 337 [10.1%]) than in patients from within Kigali (6 of 244 [2.5%]). We observed the same pattern for exploratory laparotomies, with 9 of 11 (85.0%) procedures performed on patients transferred from other provinces.
Operative procedures for trauma at the Centre Hospitalier Universitaire de Kigali in Rwanda between June 1 and Dec. 1, 2011, by geographical origin
Discussion
To our knowledge, this study was the first to evaluate trauma caseloads at the largest referral centre in Rwanda and the first to describe geographical variations in access to operative trauma care. Surgical procedures for trauma represented a large proportion of all operations performed at the CHUK, and a vast majority of these were orthopedic in nature. In fact, fractures and dislocations were the most common indications for surgery, and fracture reductions and fixations were the most commonly performed procedures. Approximately 58% of trauma patients were transferred from outside Kigali. Interestingly, almost three-quarters of general surgery procedures for trauma were performed on patients transferred from other provinces.
This study therefore has important implications. The sheer volume of surgical procedures — more than 2700 performed within a 6-month period — is impressive by any standard and attests to the surgical teams in this resource-limited setting. Nonetheless, a countrywide survey of unmet surgical needs conducted in 2011 revealed that 6.4% of the population had a current operative condition.17 This implies that future efforts should continue to augment hospital-based surgical capacity, even in the largest tertiary care centre in the country. The predominance of orthopedic procedures provides a specific alley for operative resource planning, ranging from mobilization and training of human resources to improvement of the material resource capacity. Ultimately, improved surgical and trauma capacity will go hand in hand.
It is estimated that 17% of the Rwandan population has experienced an extremity injury in their lifetime;18 this, in addition to the fact that more than 80% of trauma procedures at the CHUK were orthopedic, points to an important selection bias. It is likely that individuals with injuries affecting more life-threatening anatomic regions do not survive transport to a definitive care centre. Consequently, the finding that three-quarters of patients who underwent a general surgery procedure were transferred from outside Kigali is likely an underestimation of the surgical need required to address injuries to the trunk outside of Kigali. This has important implications in the development of trauma systems, both at the prehospital level and in terms of strengthening district hospitals. In fact, a systematic review of barriers to surgical care in LMICs identified geographical distance, absence of suitable transport and lack of funds as the major obstacles.19 Recent evidence from Rwanda shows that 77.0% of households lack the funds for travel to the nearest referral hospital and 70.4% are located more than 2 hours away from the nearest operative services.17 In the present study, the selection bias leading to a predominance of orthopedic procedures highlights the importance of strengthening the prehospital and transfer system not only to better manage orthopedic injuries, but also to expedite the care of patients with trunk injuries who are likely not surviving the prolonged transfer times to definitive care. A large proportion of prehospital transport and first aid in LMICs is currently provided by commercial drivers and layperson bystanders.20 Training programs for layperson first responders build on available resources and have been successful in some settings.21,22 Future efforts may therefore focus on maturing the prehospital system by expanding first responder training programs and transport mechanisms between hospital centres and underserved areas.
The role of district hospitals in the development and regionalization of trauma systems cannot be overemphasized. A comprehensive review of emergency surgical capacity in Rwanda revealed that, although 80% of operating theatres were located in district hospitals, 80% of the surgical workforce was located in the capital city.14 A recent review of district hospitals across 17 countries, including Rwanda, reported that less than one-third were capable of providing basic resuscitation and 39% were not capable of performing laparotomies.23 Deficiencies at the district level inevitably translate into delayed presentations at the referral hospitals. Strengthening district hospitals, in terms of the care for orthopedic and thoracoabdominal injuries for example, may improve outcomes while freeing resources at the referral level. This is corroborated by the finding that orthopedic procedures were more common in patients from within Kigali city, which is likely explained by geographical proximity rather than provincial variations in mechanisms of injury. Moreover, it is unclear why most general surgery procedures performed for trauma at the CHUK were for patients transferred from other provinces; this may be explained by deficiencies in human and material resources at the district level for basic general surgery procedures, such as laparotomies. As prehospital systems mature, valuable resources at referral centres will be indispensable in addressing the influx of salvageable patients. Ultimately, hospital and trauma centre designations, such as those put forward by the American College of Surgeons’ Committee on Trauma,24 may contribute to better organizing referral systems.
The provision of trauma care is therefore a complex interplay of agencies, including prehospital, hospital (both district and tertiary), and interfacility services. The organization of this system will inevitably require input at the ministry level. Several educational initiatives have already been implemented, including the Trauma Team Training (TTT) and Advanced Trauma Life Support (ATLS) courses.25 The Human Resources for Health initiative is an example of health care development on a grander scale stemming from the Ministry of Health.26 Although the evaluation of the impact of these interventions is difficult given the multiagency and multifactorial nature of trauma care, this study provides evidence that deficiencies still exist and that specific future directions include strengthening district facilities, maturing prehospital and interfacility systems and further supporting referral centres.
Limitations
This study does present limitations. It is a retrospective review over a short period of time in a single institution. As trauma volumes may vary over time and among institutions, the findings may not be generalizable. Moreover, our study did not include other referral institutions, such as the Centre Hospitalier Universitaire de Butare, the Kanombe Military Hospital and the King Faisal Hospital, and it remains unclear why patients originating from regions closer to these hospitals were treated at the CHUK. A better understanding of the referral patterns among these institutions would be essential in regionalizing the trauma system. However, as the CHUK represents the largest referral centre in the country, its surgical volume is central to the development of this system. In select cases, geographical data may have limited validity if the trauma occurred at a site distant from the patient’s place of residence. This study does not include any outcomes data, which would be an important next step in evaluating and monitoring the trauma system. Nevertheless, our study provides an essential first step in describing the utilization of trauma resources at the CHUK.
Conclusion
To our knowledge, this is the first study to highlight geographical variations in access to trauma care in a low-income country and the first to describe trauma procedures at a referral centre in Rwanda. Future efforts should focus on maturing prehospital systems, strengthening hospitals at the district level and further supporting referral institutions as they strive to address the plight of injury in resource-limited settings.
Acknowledgments
We are grateful to all members of the surgery department at the CHUK for their dedication to patient care and data collection. The Centre for Global Surgery of the McGill University Health Centre provided financial support for travel expenses related to the work presented in this manuscript.
Footnotes
Financial support: Centre for Global Surgery, McGill University Health Centre.
Competing interests: G. Ntakiyiruta and P. Kyamanywa have received travel support from McGill University Health Centre. A.S. Liberman has received speaker fees from Covidien. T. Razek is a board member (unpaid) for the Canadian Network for International Surgery. No other competing interests declared.
Contributors: G. Ntakiyiruta, T. Razek, P. Kyamanywa and D.L. Deckelbaum designed the study. M.C. Rousseau, L. Ruhungande and M. Wilson acquired the data, which G. Ntakiyiruta, E.G. Wong, M.C. Rousseau, A.L. Kushner, A.S. Liberman, K. Khwaja, M. Dakermandji, T. Razek, P. Kyamanywa and D.L. Deckelbaum analyzed. E.G. Wong, M.C. Rousseau, M. Dakermandji and D.L. Deckelbaum wrote the article, which all authors reviewed and approved for publication.
- Accepted November 9, 2015.
References
In this issue

{kind=link}
Article tools





