


Abstract
Background: Low-dose ionizing radiation from medical imaging has been indirectly linked with subsequent cancer and increased costs. Computed tomography (CT) is the gold standard for defining pancreatic anatomy and complications. Our primary goal was to identify the temporal trends associated with diagnostic imaging for inpatients with pancreatic diseases.
Methods: Data were extracted from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample (NIS) database from 2000 to 2008. Pancreas-related ICD-9 diagnostic codes were matched to all relevant imaging modalities.
Results: Between 2000 and 2008, a significant increase in admissions (p < 0.001), but decrease in overall imaging procedures (p = 0.032), for all pancreatic disorders was observed. This was primarily a result of a reduction in the number of CT and endoscopic retrograde cholangiopancreatography examinations (i.e., reduced radiation exposure, p = 0.008). A concurrent increase in the number of inpatient magnetic resonance cholangiopancreatography/magnetic resonance imaging performed was observed (p = 0.040). Intraoperative cholangiography and CT remained the dominant imaging modality of choice overall (p = 0.027).
Conclusion: Inpatients with pancreatic diseases often require diagnostic imaging during their stay. This results in substantial exposure to ionizing radiation. The observed decrease in the use of CT may reflect an improved awareness of potential stochastic risks.
Pancreatic diseases include, but are not limited to, both acute and chronic pancreatitis as well as pancreatic neoplasia. These conditions represent some of the most debilitating and life-threatening diagnoses in all of surgery. As a result, pancreatic diseases challenge our clinical, social and financial resources. Not surprisingly, this patient population is at significant risk for perioperative morbidity and postoperative mortality during their time as inpatients. They also often undergo extensive outpatient imaging surveillance protocols for years of follow-up.1
The current noninvasive, gold standard modality for the detection and assessment of nearly all pancreatic diseases is computed tomography (CT) with intravenous contrast medium.2 Although pancreatic ductal anatomy is better evaluated with magnetic resonance cholangiopancreatography (MRCP), and fluid analysis is clearly superior via endoscopic ultrasonography, high-fidelity CT remains the dominant workhorse in high-volume pancreatic centres. In addition to the inherent risk of contrast-associated nephropathy, CT imaging exposes patients to a measurable dose of ionizing radiation.3–6 Considering the frequent need for multiple CT scans during the course of their inpatient care (i.e., necrotizing pancreatitis or postoperative complications after pancreatic procedures), a patient’s radiation exposure can be substantial. The increasing use of CT imaging7–12 coupled to the growing incidence of both pancreatitis13–17 and pancreatic tumours (i.e., intraductal papillary mucinous neoplasm [IPMN]), makes this public health issue especially topical.
The primary aim of this study was to identify temporal trends in diagnostic imaging procedures for patients with diseases of the pancreas using a large national database.
Methods
Data source
All data were collected from the Healthcare Cost and Utilization Project central distributor via the National Inpatient Sample (HCUP-NIS) database (2000–2008). The HCUP-NIS represents the largest publicly available database of hospital admissions in the United States, with all-payer sources (Medicaid, Medicare, privately insured, and uninsured). It is a discharge-based registry (i.e., each entry represents a single hospital admission) that contains primary and secondary diagnoses and procedures, patient demographic characteristics, and other clinical and nonclinical data elements of inpatient discharge records from community hospitals in participating states. The individual state inpatient databases are uniformly formatted to allow representative sampling into NIS and multistate analyses. Progressive increases in sampling frame (from 8 states in 1988 to 48 at present) and constant review of sampling design have optimized U.S. population representativeness over the years. The HCUP-NIS currently approximates a 20% stratified sample of discharges from community hospitals in the United States, representing more than 95% of the U.S. population. All available information is de-identified, and different admissions for the same patient are registered as distinct entries. Accounting for changes in NIS design over the years, NIS supplemental files containing revised discharge weights were used to consistently represent United States nationwide data trends.
Study population
We used ICD-9-CM codes to define eligible participants and for data abstraction from the HCUP-NIS. All hospitalizations from 2000 to 2008 with a primary diagnosis of acute pancreatitis (code 577.0); chronic pancreatitis (code 577.1); or neoplasia of the head (code 157.1), body (code 157.0), or tail (code 157.2) of the pancreas were included. A search of the ICD-9-CM code conversion table revealed no changes to the included codes during the study period (i.e., ICD-9-CM diagnostic terminology consistently represents this subpopulation of discharges throughout the study period).
Data elements
The number of imaging procedures performed during hospitalization was abstracted and computed separately for distinct imaging modalities under each primary diagnosis group. Imaging modalities were selected according to clinical relevance based on the primary diagnosis (acute and chronic pancreatitis; neoplasia of the head, body and tail):
diagnostic ultrasonography of the abdomen (codes 88.76 and 88.76)
axial CT of the abdomen (code 88.01)
magnetic resonance imaging (MRI) of the abdomen (code 88.87)
endoscopic retrograde colangiopancreatography (ERCP; codes 51.10, 51.11, and 52.13)
intraoperative cholangiography (IOC; code 87.53)
percutaneous hepatic cholangiography (PTC; code 87.51), and
endoscopic ultrasonography of the abdomen (211.1)
Analysis
We assessed and analyzed primary diagnosis groups independently, except for neoplasm of the body and tail of the pancreas. These were considered together as neoplasia of the distal/left pancreas.
The frequency of each imaging modality was computed for the entire population during the study period. U.S. nationwide estimates of the number of discharges and imaging procedures were obtained using revised NIS discharge weights.
We calculated the proportion of hospitalizations, including imaging procedures, for each imaging modality as annual utilization percentages. The total number of discharges in a specific calendar year with at least 1 imaging procedure performed was ascertained as the numerator, whereas the denominator corresponds to the total number of discharges in the respective year.
Count data were summarized as frequencies or proportions. A combination of descriptive statistics with linear regression adjusted per year was used to analyze the data. We considered 2-sided p values < 0.05 to represent statistical significance for all evaluations. Two-way plots were used to illustrate the temporal change in the proportion of NIS admissions over time. All statistical testing was performed using Stata/IC software version 12.0 (Stata Corp.).
Results
Acute and chronic pancreatitis
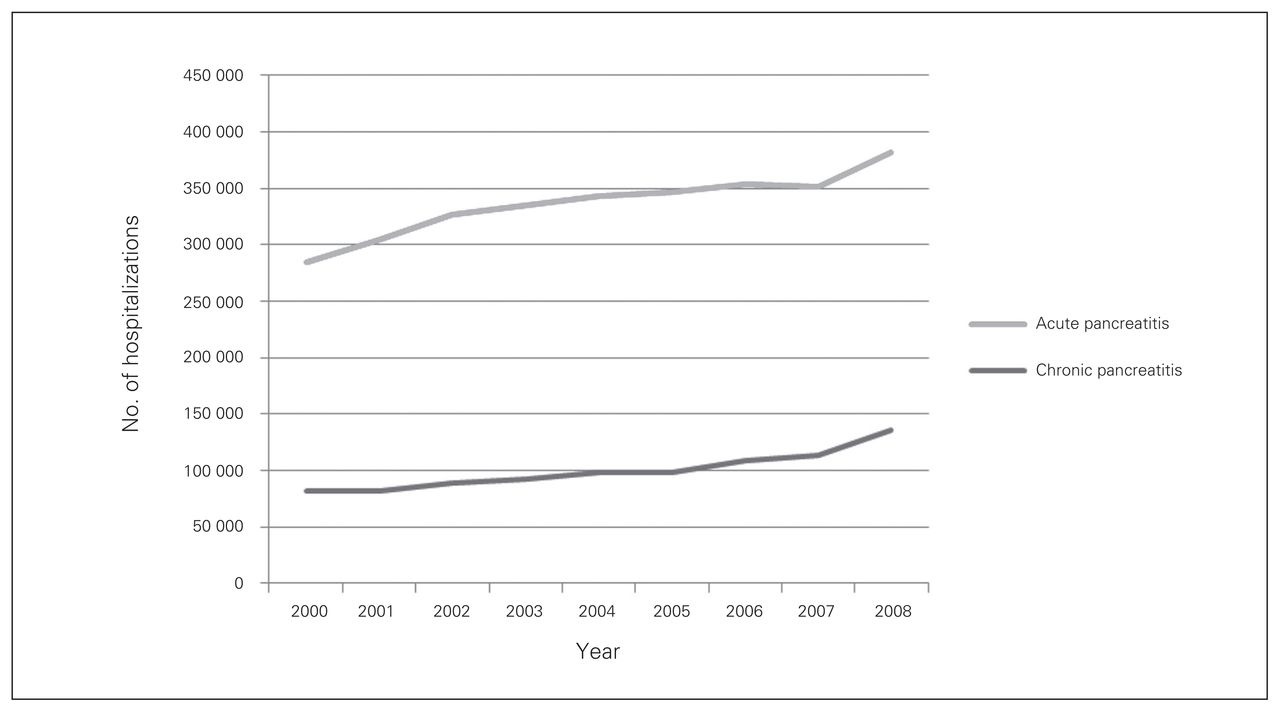
From 2000 to 2008, we noted an increase of 34.2% in hospital admissions attributed to the primary diagnosis of acute pancreatitis (284 718–382 038 hospitalizations) and 65.7% for chronic pancreatitis (82 176–136 198 hospitalizations) (p < 0.001). Described as a ratio of all inpatient admissions, this increased from 2.85 to 3.82 per 100 000 NIS admissions for acute pancreatitis and 0.82 to 1.36 per 100 000 NIS admissions for chronic pancreatitis (p < 0.001). This totals 3.9 million hospitalizations for pancreatitis in the United States over the 9-year study interval (3 028 128 acute pancreatitis; 901 549 chronic pancreatitis; Fig. 1).
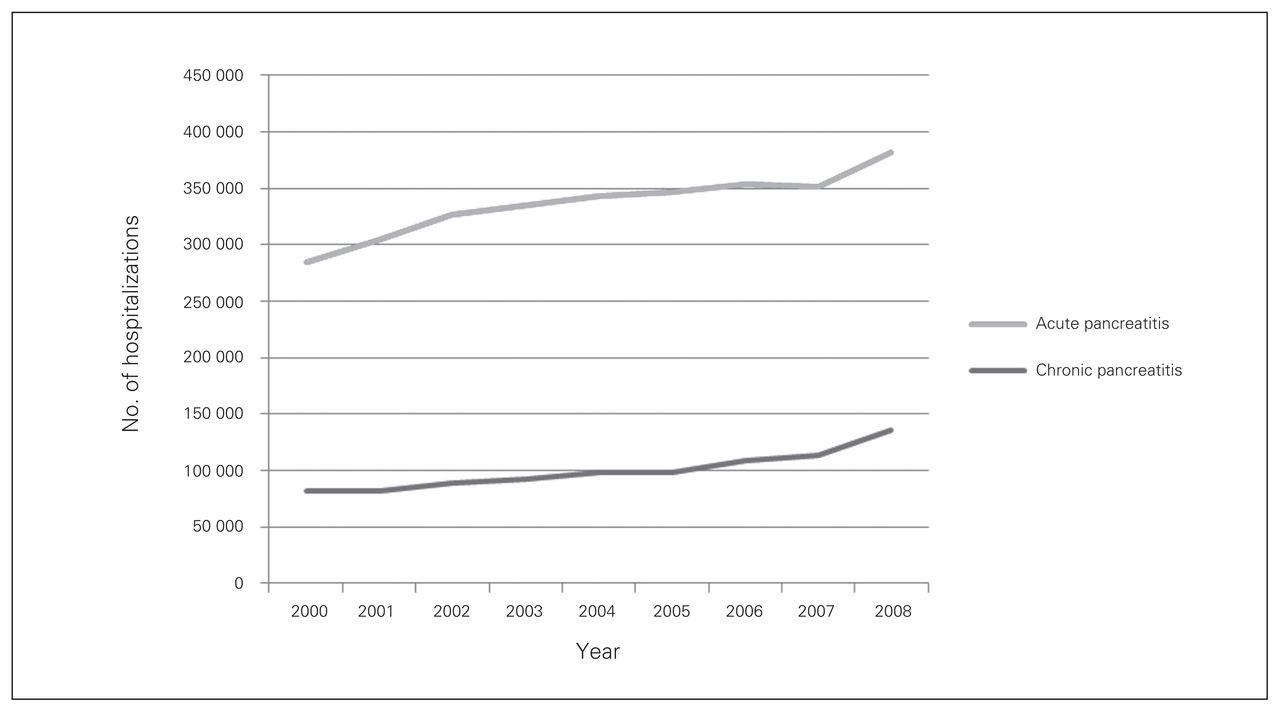
National trends over the study period (2000–2008) in number of hospitalizations with primary diagnosis of acute and chronic pancreatitis.
We observed a reduction in the overall use of imaging procedures (1 imaging procedure per 4.3 patients admitted with pancreatitis in 2000 to 1 per 6.7 patients in 2008, p < 0.001). During the study period, 68 647 diagnostic abdominal ultrasounds, 136 285 CT scans; 126 501 ERCPs, 254 185 IOCs, 23 030 MRCP/MRIs and 6485 PTCs were performed for patients admitted with a primary diagnosis of pancreatitis.
Trends in imaging modality utilization — acute pancreatitis
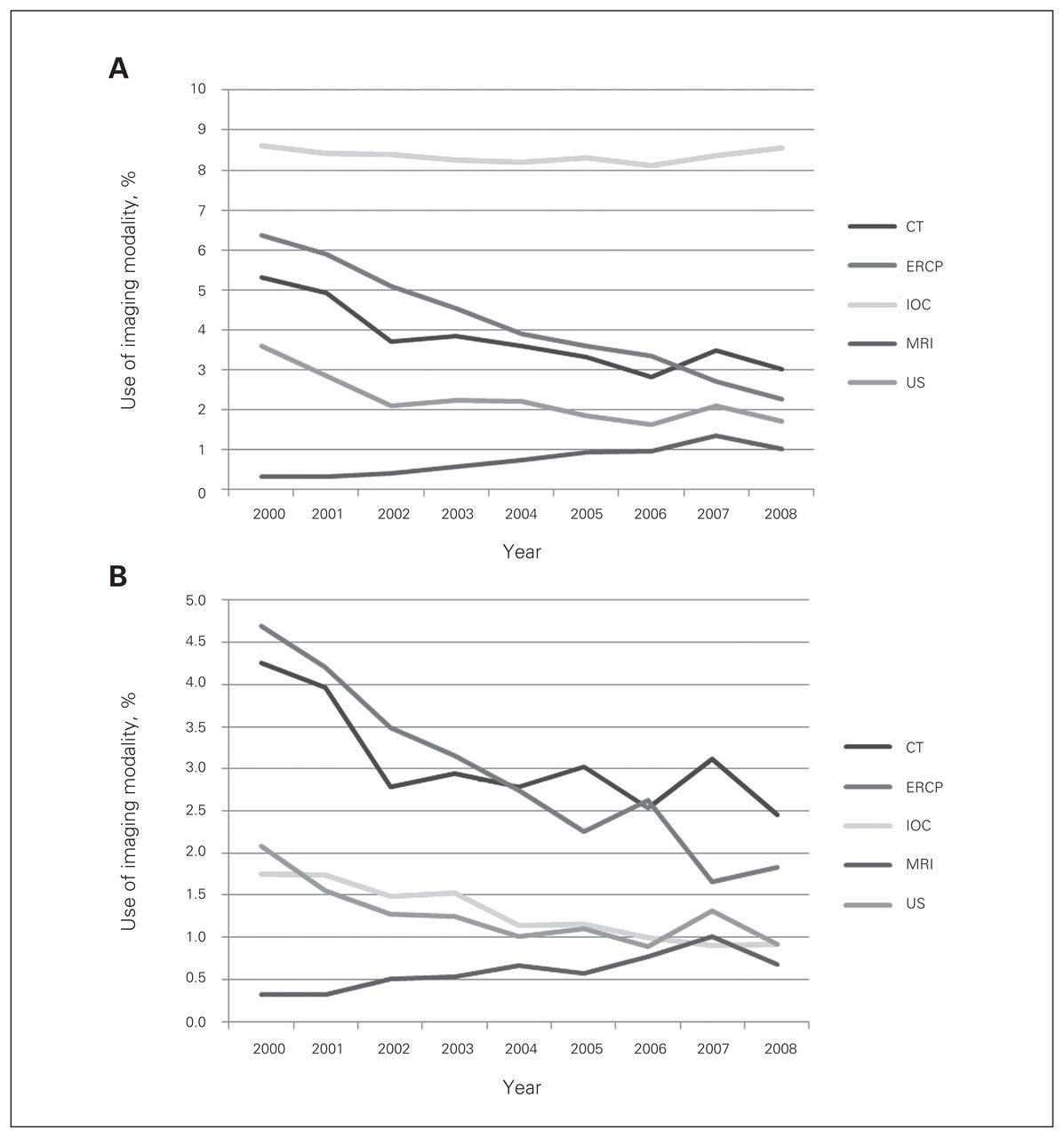
The IOC remained the most common imaging procedure, with an average annual utilization of 8.4%. The utilization of MRI increased from 0.3% in 2000 to 1.0% in 2008 (p < 0.001). There was a progressive reduction in the use of CT from 5.3% in 2000 to 3.0% in 2008 (p = 0.022). The use of ultrasonography decreased from 3.6% in 2000 to 1.7% in 2008 (p = 0.019). The largest observed decrease occurred with ERCP (6.3% in 2000 to 2.3% in 2008, p < 0.001; Fig. 2A).
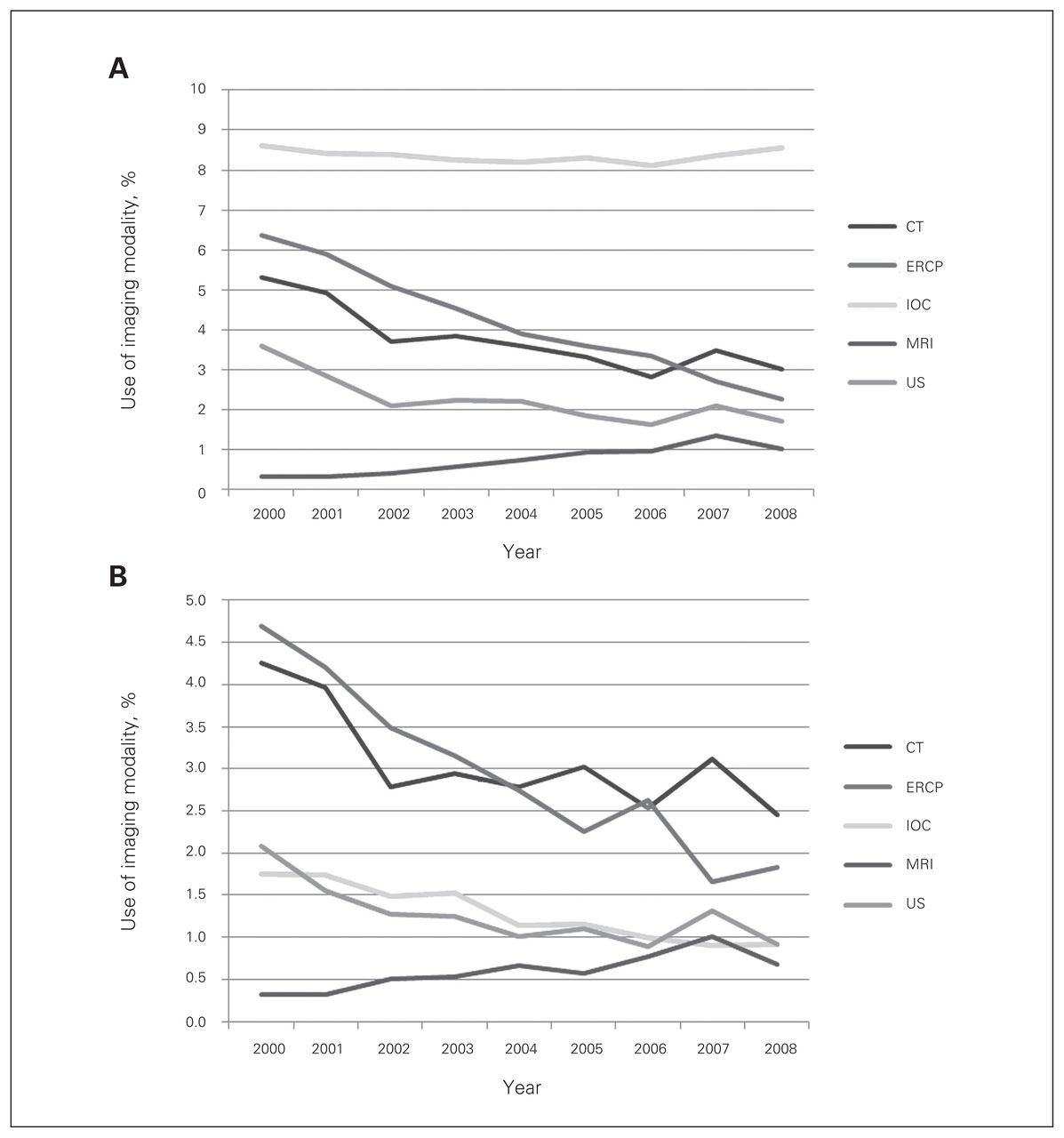
National trends over the study period (2000–2008) in utilization of imaging modalities for patients admitted with primary diagnosis of (A) acute pancreatitis and (B) chronic pancreatitis. CT = computed tomography; ERCP = endoscopic retrograde cholangiopancreatography; IOC = intraoperative cholangiography; MRI = magnetic resonance imaging; US = ultrasonography.
Trends in imaging modality utilization — chronic pancreatitis
Magnetic resonance imaging was the only modality noted to increase for hospitalized patients with chronic pancreatitis (0.3% in 2000 to 0.7% in 2008, p = 0.034). All other imaging modalities showed a reduction in use, particularly ERCP (4.7% in 2000 to 1.9% in 2008) and CT (4.3% in 2000 to 2.5% in 2008, p = 0.007; Fig. 2B).
Pancreatic neoplasia
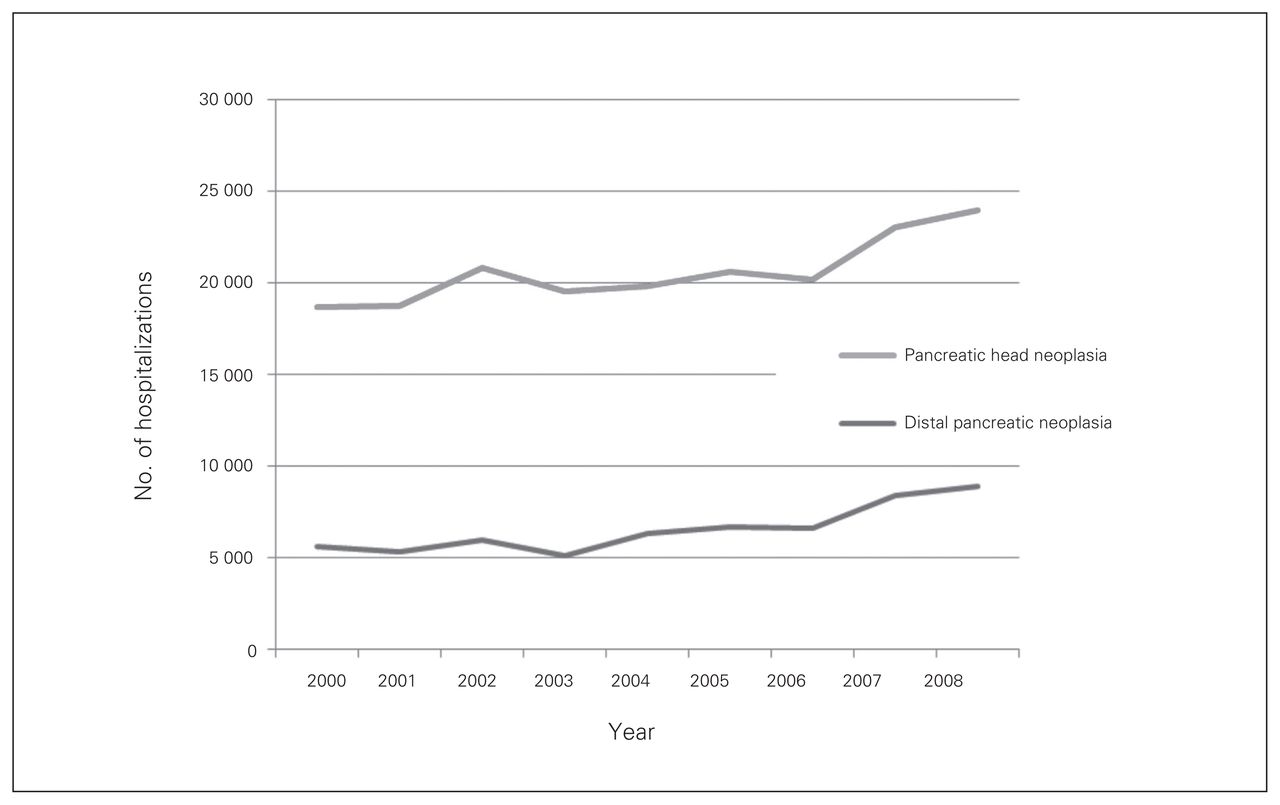
Pancreatic neoplasia resulted in a total of 244 220 hospitalizations, with an increase of 35.6% between 2000 and 2008 (24 244 to 32 869 admissions, p < 0.001). Described as a ratio of all inpatient admissions, this increased from 0.24 to 0.33 per 100 000 NIS admissions (p < 0.001). The most common tumour site (75.9%) was the head of the pancreas (185 463 admissions; Fig. 3). Hospital admissions for pancreatic neoplasia resulted in a total of 50 839 imaging procedures (3554 ultrasounds, 13 508 CT scans, 21 235 ERCPs, 1478 MRIs and 11 064 PTCs).

National trends over the study period (2000–2008) in number of hospitalizations with primary diagnosis of neoplasias of the pancreatic head and distal (left) pancreas.
Trends in imaging modality utilization — pancreatic neoplasia
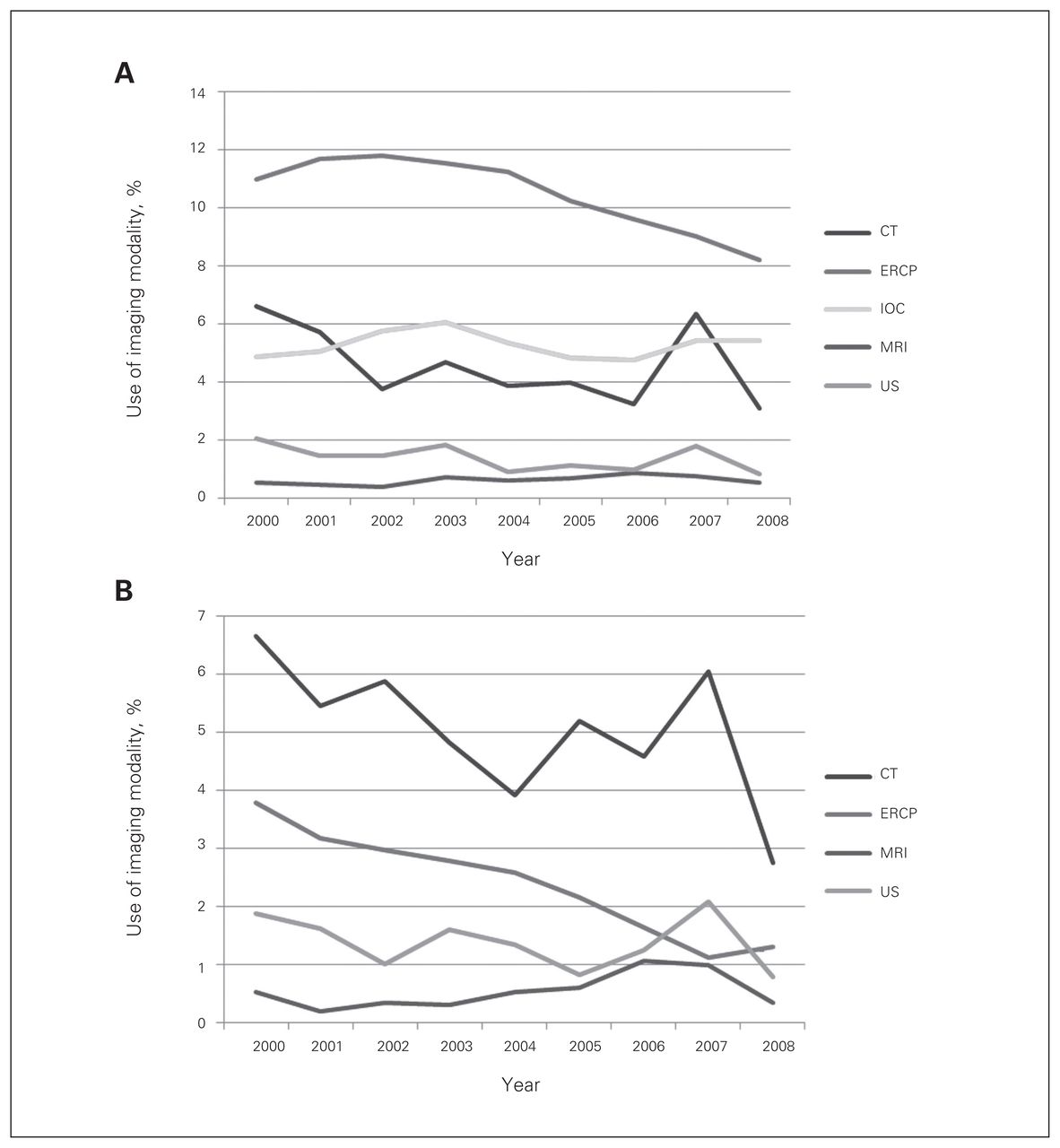
From 2000 to 2008, there was a consistent reduction in the utilization of ERCP for patients admitted with neoplasia of both the pancreatic head (11.0% to 8.2%) and distal gland (3.8% to 1.3%) (p = 0.044). Utilization of CT also decreased from 6.6% to 3.1% for neoplasia of the pancreatic head and from 6.7% to 2.8% for the left pancreas (p = 0.003). Ultrasonography and MRI utilization remained below 2.0% of hospital admissions for pancreatic neoplasms of the head and distal pancreas. Utilization of PTC in patients admitted with pancreatic head neoplasia remained unchanged, with an average annual utilization of 5.3% (p = 0.23; Fig. 4A and Fig. 4B).
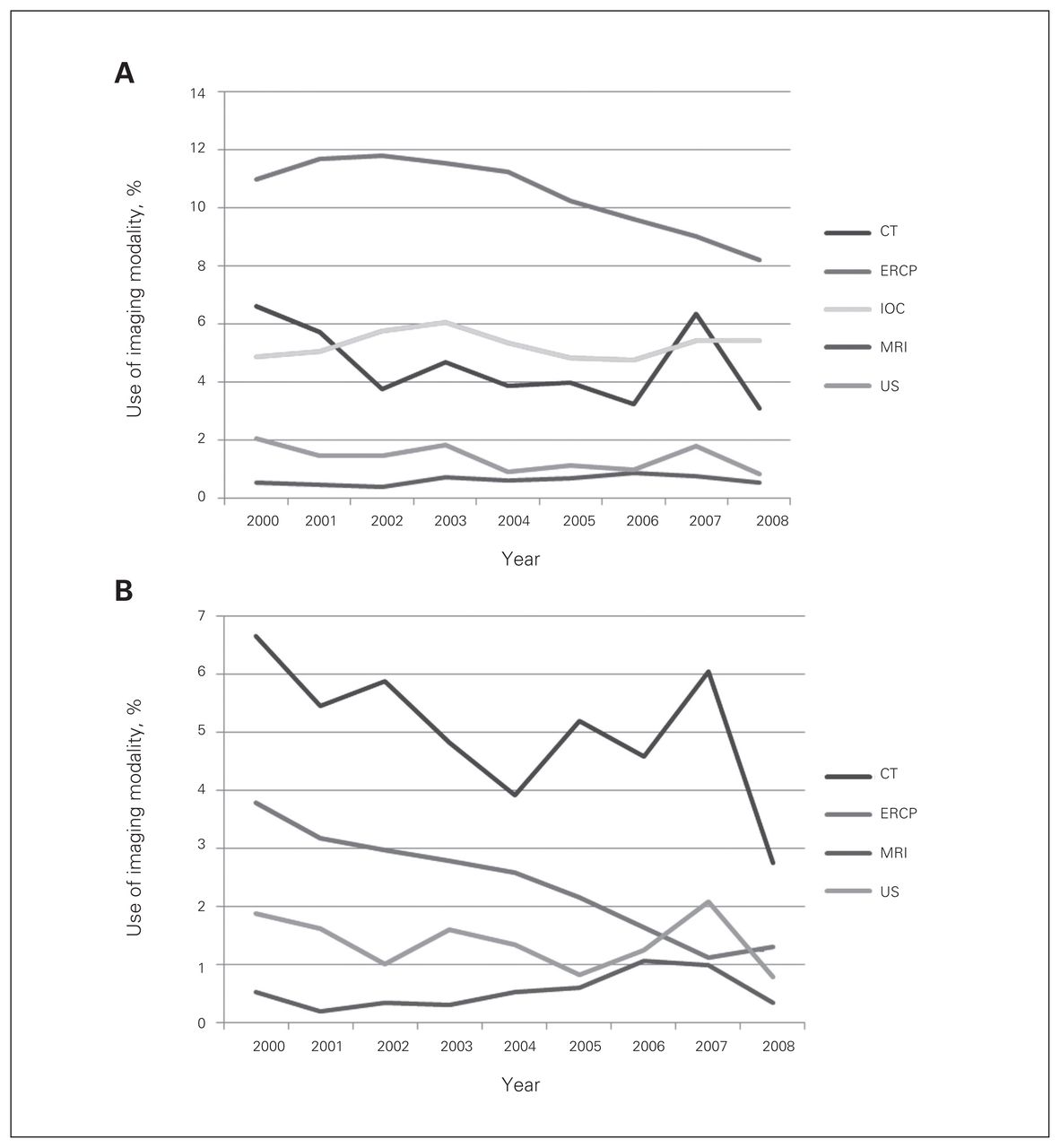
National trends over the study period (2000–2008) in utilization of imaging modalities for patients admitted with primary diagnosis of neoplasia of the (A) pancreatic head and (B) distal pancreas. CT = computed tomography; ERCP = endoscopic retrograde cholangiopancreatography; IOC = intraoperative cholangiography; MRI = magnetic resonance imaging; US = ultrasonography.
Discussion
From 2000 to 2008, the total volume of admissions for pancreatic diseases increased significantly. Whether discussing raw admission numbers or ratios per 100 000 NIS admissions, the observed 34.2%, 65.7% and 35.6% increases for acute pancreatitis, chronic pancreatitis, and pancreatic cancer, respectively, strongly suggest a true increase in the incidence of each of these diseases. Given that this total inpatient volume approaches 39 million visits, the hospital and physician resources required to care for this patient population are extensive. To our knowledge, this study is the first modern population-based description of increasing pancreatic volumes.
Although CT remains the single most important imaging modality for pancreatic diseases (diagnosis and prognosis),2 additional tests are also frequently required. These include transabdominal ultrasonography and MRCP. Invasive tests are also not uncommon and incorporate ERCP (i.e., biliary stent placement), IOC (i.e., define retained choledocholithiasis) and endoscopic ultrasonography (i.e., characterization and/or biopsy of lesions). While ultrasonography, MRCP and endoscopic ultrasonography have the benefit of avoiding the delivery of ionizing radiation to patients, CT and the fluoroscopy associated with ERCP and IOC carry potential stochastic risks. Given the explosion in CT scanner use and indications1,7,18–28 (3 million CTs performed in 1980 v. 62 million in 2006),8 radiation exposure is always a public health concern. This is evident in the nearly 6-fold increase in the per capita radiation exposure delivered from medical imaging.4 More specifically, while the majority (80% to 85%) of human radiation exposure arises from equal amounts of solar and radon sources (background dose 1–3 mSv/yr), medical imaging creates most of the remaining 15% to 20%.3,27,29,30 Furthermore, abdominal CT imaging accounted for up to 31% of the annual cumulative effective dose from medical imaging procedures in a study of nearly 1 million nonelderly adults.4
Although many clinicians would argue that the vast majority of inpatient imaging is necessary to the care of pancreatic patients, it is clearly important that as physicians we evaluate both the volume of our imaging, as well as its true utility (i.e., ability to alter care). The essential nature of this issue is supported by the observation that at least 75% of CT imaging is obtained in a hospital setting, with up to half being scans of the torso.31 This was noted to be even higher (89%) in a recent postresection pancreatic cancer–specific study.32 Furthermore, in an evaluation of the impact of CT-based ionizing radiation on patients with pancreatitis, less than 31% had subsequent alterations in their care.1 It has also been recently reported in a large registry-based study of pancreatic cancer that no benefit in survival was noted with scheduled or routine CT scans in the postoperative/postdischarge period.32 These data surrounding the issue of appropriate diagnostic tests do not begin to account for the costs associated with overly liberal imaging policies.1,32
While the true stochastic risks of DNA mutations and therefore carcinogenesis following exposure to medical imaging are unknown1 (i.e., absence of large-scale epidemiologic data),33 the potential life expectancy of the patient population must be considered. The effective dose of 40 mSv among patients with acute pancreatitis1 is identical to that reported for patients with pancreatic cancer during their first year (40.1 mSv).6 Unfortunately, patients with pancreatic cancer have substantially shorter life expectancy as evidenced by an overall 5-year exposure of only 68.8 mSv per patient.6 Given the known challenge of recovering well enough from postoperative complications to receive adjuvant chemotherapy, it can easily be argued that the radiation exposure associated with multiple CT scans in this scenario is irrelevant from a stochastic standpoint. When this concept is applied to our data set, the observed reduction in CT imaging over the study interval would have resulted in a theoretical reduction in the absolute number of patients who developed a radiation-induced fatal cancer per year of 3 for acute pancreatitis and 1 for both chronic pancreatitis and pancreatic neoplasia. As a result, the core of this issue lies in the specific discussion surrounding both benign diseases, such as pancreatitis, as well as in the frequency of altering treatment regimes based on additional imaging tests (Table 1).1
Radiation equivalents for various imaging modalities
Given the highly publicized nature of exposure to medical radiation,1,34 it was interesting to note the significant decrease in the volume of CT scans performed for patients with both pancreatitis and neoplasia. Upon discussing this observation at an international panel, audience members anecdotally felt that their own practice reflected this reality.35 This decrease in the frequency of CT clearly resulted in fewer overall diagnostic imaging tests for patients as a whole. A significant increase in the use of MRCP/MRI (3-fold) was also noted and likely reflects a move away from modalities associated with ionizing radiation (i.e., particularly benign conditions). Similar arguments can be made for the impact of endoscopic ultrasonography. Not surprisingly, given that the majority of cases of acute pancreatitis are biliary-related (choledocholithiasis), IOC remained the most common imaging modality overall. Furthermore, despite ultrasonography being the most frequent initial diagnostic test for cases of acute pancreatitis, its observed decrease may reflect an increased volume of outpatient ultrasonography performed before acute attacks requiring hospital admission.
It was also interesting to note that the frequency of ERCP decreased significantly. Given the strong evidence that most (75.9%) cancers are located in the head of the pancreas and that preoperative ERCP and biliary stent placement increases the risk of postoperative complications,36 this observation is likely reflective of evidence-based changes in practice over time. More specifically, in a country with rapid access to the operating theatre for resective procedures (e.g., Whipple), preoperative biliary stents have become relatively contraindicated. In the context of prolonged wait times, Canadian surgeons continue to struggle with this issue. This pattern also reflects strong evidence against the use of ERCP in patients with acute pancreatitis in the absence of persistent biliary obstruction or cholangitis.37 It is furthermore evident that the overall frequency of diagnostic ERCP has decreased substantially in the context of acute biliary diseases in a large U.S. database study.38
Limitations
This study has several limitations. First, as a result of the aggregated or ecological nature of the data, our results can be interpreted only as associations on a population level, and therefore not causative at the individual level. This limitation extends to deriving any individual level patient conclusions. Second, although the HCUP-NIS database leads to strong observations based on the volume of data, there is no specific confirmation of compliance in reporting of a particular data field by a given centre. As a result, while the pattern of change in diagnostic tests remains reliable over time, the reported specific incidence is subject to error. Third, the NIS data set is limited to inpatient admissions, and as a result does not allow commentary on the volume or frequency of outpatient CT imaging that likely occurs and potentially predominates the care of patients with neoplastic pancreatic diseases. Fourth, the inability of this data set to discriminate between mild and severe/critical acute pancreatitis also limits the interpretation of the rate of CT imaging. A higher rate of CT examinations would clearly be expected for more severe variants of pancreatitis. Similarly, patients with pancreatic neoplasia would also be expected to display a higher rate of CT imaging following resection compared with nonresection admissions. Finally, extrapolation of the specific ionizing radiation exposure to a patient group is difficult given the population-based nature of the data. The delivered effective dose can vary significantly based on the individual CT scanner (i.e., number of slices). The reported effective dose for a standard single-phase abdominal CT scan ranges from 1.5 to 10 mSv depending on the number of channels,3,11 although the generally recognized average effective dose is 8 mSv (Table 1). In comparison, exposure for both pilots/flight crews (1000 flight h/yr) and occupational radiation workers approximate 5 mSv per year. Recent estimates of the lifetime risk of radiation-induced cancer approximate 1 person in 100 for those exposed to 100 mSv (relative risk 1.024; Table 1).39 The lifetime risk of cancer from all other causes is 42 in 100, and the risk of dying from a motor vehicle crash in the United States is 1 in 77.28,40–42
Conclusion
In summary, despite an increasing overall volume of admissions for pancreatic diseases, the frequency of inpatient CT imaging is decreasing while the use of MRCP/MRI is increasing. This observation is notable in the context of potential patient and physician concerns regarding the stochastic risks of ionizing radiation. The observed reduction in ERCP use among patients with pancreatic neoplasia is likely a reflection of the strong evidence favouring the avoidance of preoperative biliary stenting and therefore proceeding directly to operative resection in a timely manner.
Footnotes
Competing interests: None declared.
Contributors: J.-F. Ouellet, E. Dixon, S. Grondin, R. Myers, R. Mohamed and C. Ball designed the study. J.-F. Ouellet, D. Tanyingoh, G. Kaplan and C. Ball acquired the data, which A. Bressan, J.-F. Ouellet, D. Tanyingoh, G. Kaplan, R. Myers and C. Ball analyzed. A. Bressan, S. Grondin and C. Ball wrote the article, which all authors reviewed and approved for publication.
- Accepted February 25, 2016.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.